Cronobacter sakazakii is an opportunistic foodborne pathogen that causes diseases like meningitis, necrotizing enterocolitis, and bacteremia in immunocompromised, low weight individuals, neonates, infants, and elders. Cronobacter sakazakii has the ability to persist in extremely dried foods such as powdered infant formula (PIF). Infant food contamination by this bacterium is attributed to biofilm which are microbial communities attached to biotic or abiotic surfaces using a self-produced matrix of extracellular polymeric substances. Cronobacter sakazakii can form biofilms on food, food processing surfaces, and equipment that leads cross-contamination. Cronobacter sakazakii also showed multidrug resistance to some antibiotics. Biofilm formation accompanied by antibiotic resistance is worrisome for medication. Therefore, to prevent or reduce risk contamination infant food companies, health sectors, caregivers, aid providers, and other concerned bodies must be informed and alerted about this hidden bacterium. Thus, this review article gives a brief overview of the role of Cronobacter sakazakii in infant food contamination and its survival strategies in hostile conditions.
Cronobacter sakazakii, Infant food contamination, Biofilms, Antibiotic re-sistance, Dry tolerance
Cronobacter sakazakii (formerly Enterobacter sakazakii) is one of an opportunistic pathogen that can contaminate a wide range of foods and causes different disease like meningitis, necrotizing enterocolitis and bacteremia in immunocompromised, low weight individuals, neonates and infants with a mortality rate of 40-80% [1-58]. As Almajed and Forsythe [6] indicated in their research Cronobacter sakazakii clinical isolates are able to overcome host barriers and evade the host immune response indicating their capacity to cause diseases such as necrotizing enterocolitis (NEC) and meningitis. Henry and Fouladkhah [7] reported that there have been a few recent outbreaks and sporadic cases of Cronobacter sakazakii infections in the country and around the world associated with infant mortality and morbidity. Cronobacter sakazakii is a gram-negative, facultative anaerobic, motile with peritrichous flagella, rod-shaped and non-spore forming bacterium. It belongs to the genus Enterobacter and Enterobacteriaceae family and becomes risky to infant health [8,9]. Bacterial infection is a concern for all age groups [10], but infants, elders, and immuno-compromised individuals are highly vulnerable age groups [11,12]. The same is true for Cronobacter sakazakii that causes infections in all age groups, but it threatens infants and other susceptible individuals [8]. This is because Cronobacter sakazakii is found in high-risk foods such as powdered infant formula, dried infant foods and can cause infections after consumption [13,14] (Figure 3). This bacterium can survive and persists in powdered infant formula and preparation equipment which have been linked to different complications among infants [7,15] (Figure 3). Cronobacter sakazakii has several strategies such as osmotic and dry tolerance, tolerating a wide range of growth temperatures, biofilm formation, and antibiotic resistance are tremendous for the survival of this bacterium on hostile environments [9,16,17]. As many research works revealed biofilm-related infections are an increasing health threat in medical sectors [18], which can cause chronic infections and antibiotic resistance [19]. Biofilm-related infections are serious since microbes undergo physiologic and structural changes that are tolerant of hostile conditions such as antibiotics, sanitizing agents, and host immune systems [20]. Cronobacter sakazakii is resistant to many antibiotics such as ampicillin, cefotaxime, cephalothin, and ceftriaxone [21]. Therefore, biofilm formation along with antibiotic resistance becomes an escalating problem in health sector. Although Cronobacter sakazakii is known in scientific communities, mothers, caregivers, elders, infant food companies, aid providers, communities in refugee camps, food packing companies, baby bottle manufacturers and other concerned bodies must be alerted about this hidden bacterium. Therefore, this review article gives a brief overview of the role of Cronobacter sakazakii in infant food contamination and its survival strategies in hostile conditions
Age is one of the critical determinants of the immune system [22]. Infants, elders, pregnant women, and people who have debilitated immune systems are susceptible populations to foodborne diseases [23]. For example, Cronobacter sakazakii is one of life-threatening bacterium for immunocompromised, low weight individuals and premature infants whose age is less than 28 days [3,24-29]. The infection caused by Cronobacter can be serious for older people and for people whose immune systems are weakened by other illnesses or conditions [30]. Generally, this bacterium targets immunocompromised, low weight individuals, neonates, and infants [1]. The ability of Cronobacter sakazakii to survive osmotic stress and low water activity environments for as long as two years further provides acceleration in the likelihood of this disease occurrence in these vulnerable populations [7]. Due to these reasons, it has been ranked by The International Commission for Microbiological Specification for Foods as a bacterium having "severe hazard for restricted populations, life-threatening or substantial chronic sequelae or presenting effects of long-duration [31]".
The principal and forefront infant food providers are mothers who feed their sterile breastfeeding. According to Centers for Disease Control and Prevention (CDC) breastfeeding is one of the best things you can do for your baby’s health and development [30]. Therefore, it is a precious gift given by mothers to their infants [32]. From a nutritive and health point of view, breastfeeding is the safest infant nutrition. However, when mothers are infected with communicable diseases, breastfeeding may not be given to their infants [33-35]. Cronobacter sakazakii is a critical threat for infants of HIV-positive mothers since breastfeeding aggravates the viral transmission. Unless intervention is taken the virus can be transmitted from mother-to-child via breastfeeding [36]. In this case, infants may use alternative feedings such as infant formula but these products are not sterile enough because of microbial cross-contamination like Cronobacter sakazakii [3,14,37,38]. The other contributing factors that lower the rate or early cessation of breastfeeding is that mothers might be informed not to breastfeed or the mother may take medication [34], or infants born from working-class mothers. The employment of mothers, especially full-time employment, has a negative influence on the duration of breastfeeding [39]. This is because mothers do not have enough time to nurse their infants so that they may use alternative feedings such as infant formula [40]. But infant foods can be contaminated with Cronobacter sakazakii and other pathogens that can cause serious health problems and even death in newborns and children [41]. If the health status of mothers is good enough it is better to resume breastfeeding to prevent infants and children from Cronobacter sakazakii or other pathogens.
Foods can be contaminated during harvesting, manufacturing, processing, packing, distribution, retailing, handling, preparation, storing, reconstitution and consumption [23]. According to Food and Agriculture Organization (FAO) reports powdered infant formula (PIF) can be intrinsically contaminated with Cronobacter sakazakii. That is why risk assessment considers preparation, storage and feeding of PIF to infants [42]. Therefore, food contamination is a critical issue in food safety because of the transmission of opportunistic foodborne pathogens such as Cronobacter sakazakii [43]. Infant food contamination by this bacterium can exert pressure on food industries, families, infant health, mothers, health sectors and global markets. The microbiological safety of powdered infant formula has got increasing attention due to contamination by Cronobacter sakazakii and its causative agents of life-threatening neonatal infections [29]. However, attention is not given for this bacterium especially in developing nations. For instance, in Ethiopia it is assumed that the number of infections caused by Cronobacter sakazakii is under reported. Unlike the vast majority of main foodborne pathogens, Cronobacter sakazakii infections are not currently a reportable disease in nearly all states [7]. Cronobacter sakazakii is a threat to infant, neonatal and other susceptible age groups resulted from utilizing contaminated powder infant formula or utensils such as spoons used for reconstitution (Figure 1). Cronobacter sakazakii outbreaks is linked to contamination of powdered infant formula (PIF) or contaminated utensils used for PIF reconstitution [27] (Figure 3). Cronobacter spp. were isolated from the manufacturing environment, intermediate powder, and finished products and from those isolates Cronobacter sakazakii was the most prevalent when compared to others [44]. This was also in agreement with a study conducted by Hochel, et al. and Lee, et al. that indicated Cronobacter sakazakii was the most prevalent species recovered from food samples analyzed when compared to other Cronobacter spp. [45]. Therefore, powdered infant formula is the greatest reservoirs of Cronobacter sakazakii. As reported by numbers of scholars this bacterium has been isolated from different samples such as clinical specimens, environmental, foodstuffs and food processing environments [46,47]. Cronobacter sakazakii has been isolated from a wide range of environmental sources and several foods of animal and plant origins such as cereal, fruit and vegetables, legume products, herbs, spices, milk, meat, fish, infant milk formula, milk powder, herbal teas, cheese products, and even isolated from environmental samples such as in dust [8,13,28,44,48-50]. Cronobacter sakazakii was also identified from the mouths of stroke patients [51]. It is the most frequently clinically isolated species of the Cronobacter genus [6]. As reports revealed reconstituted infant formula in neonatal intensive care unit was contaminated by Cronobacter sakazakii that causes infections and this alarms caregivers, industries, scientific communities, and other stakeholders to improve neonatal health care units [14]. For instance, in a neonatal intensive care unit Cronobacter sakazakii infections had occurred in 1994 in France and 17 neonates were infected and showed enterocolitis, septicemia, and meningitis with different prevalence [4]. Cronobacter sakazakii is ubiquitous [48], but it is profoundly linked with infant formula powders which are implicated in infant infections [52]. Intrinsic contamination reports are coming up frequently that indicates the product is not sterile. For instance, in Canada, United States, Europe, and Asia-Pacific region there was a recall of infant formula from the market because of contamination of the product with Cronobacter [53,54]. Similarly, contamination of PIF with these opportunistic pathogens was quite common in German in the early 2000’s [55]. In support of this notion, Cronobacter spp has been recovered from previously unopened tins of powdered infant formula, indicating intrinsic contamination [14]. One of the possible sources of contamination might be from the factories because of the ineffectiveness of methods to remove all microbes from powdered infant formula once and for all [34,56] or maybe from the ingredients added that may carry foodborne pathogens such as Cronobacter sakazakii. This is because various thermo-labile raw ingredients are added to PIF without heat treatment [57]. As the World Health Organozation (WHO) report revealed a single contamination report in the food sector has the power to recall tones of food products from where they are found and leads to the economic crisis, tourism reduction and trade embargo and it has the power to darken the country reputation as well [58]. As reports revealed Cronobacter sakazakii is the cause of product recalling from the market. In addition to Cronobacter sakazakii, other bacteria such as Listeria monocytogenes, Staphylococcus aureus, Escherichia coli O157: H7, Salmonella spp., Vibrio parahaemolyticus, Streptococcus agalactiae and Pseudomonas fluorescens can contaminate milk and meat products such as cheese, milk powder, fermented milk, and sausage [59]. Infant formula powder samples had been contaminated by pathogens like Klebsiella pneumoniae, Klebsiella oxytoca, and Enterobacter cloacae [60]. As reported by Zhou, et al., Cronobacter sakazakii and Klebsiella pneumoniae cause morbidity and mortality in infants after consuming contaminated powdered infant formula [61]. A study conducted by Cho, et al. revealed that Cronobacter sakazakii, Salmonella enterica, Staphylococcus aureus are major pathogens associated with infantile fatal diseases which can contaminate powdered infant formula from different sources such as hands or skins of food handler or materials like spoons used for reconstituting [62] (Figure 3). Salmonella enterica can contaminate powdered infant formula and grouped with Cronobacter sakazakii, under category "A" which causes illness in infants [37]. Cronobacter sakazakii is not the only problem for human beings but also other organisms such as chicks. As recent studies indicated Cronobacter sakazakii can also contaminate fertilized eggs which may result in weak chicks, poor chick growth increased mortality of embryos, lower hatch ability and increased early chick mortality [63]. Generally, even if this bacterium can contaminate various foodstuffs, it is an obscure danger in infant formulas and baby foods [56].
The effects of bacterial infections depend on health status, nutrition, hygiene, age, and bacterial related virulence factors such as toxins, structures, and enzymes [23]. Some pathogenic microbes possess structural, enzymatic, or toxic virulence factors that have a decisive role in their pathogenicity (Figure 2). That is why microbes possessing such kinds of virulence factors are deadly pathogens and infectious. Even if we have an array of "radar" like the immune system, these deadly pathogens have the power to dismantle our immune system using virulence factors. Although Cronobacter sakazakii is an opportunistic foodborne pathogen that can cause life-threatening meningitis and necrotizing enterocolitis in premature infants, much was not known about its virulence determinants [65]. Cronobacter sakazakii possesses virulence factors that aid in tissue adhesion, invasion and host cell injury [9,17]. The specific virulence factors associated with the pathogenesis are outer membrane proteins, enterotoxin, outer membrane protease, sialic acid utilization, iron acquisition system, efflux system, proteolytic enzymes, lipopolysaccharides, and type III hemolysin [17] (Figure 2). As reports revealed Cronobacter sakazakii strains were able to adhere to cell lines, HT-29, and N1E-115 cells and the majority of them demonstrated diversified virulence factors [9]. As reported by Almajed and Forsythe [6], Cronobacter sakazakii was able to persist and multiply in phagocytic macrophage and microglial cells. A study conducted by Parra-Flores, et al. confirmed that Cronobacter sakazakii strains isolated from powdered infant formula were more invasive than other Enterobacter spp. which might be the attributes of virulence factors [21]. New and novel virulence factors known as labp have been discovered in Cronobacter sakazakii that promote the production of lipid A by using a binding partner called LpxA [65]. Virulence genes that encode various proteins involved for motility, synthesis of iron-chelating such as Enterobactin, metabolism of sugars like galactose, and mannose are critical for virulence [64]. Besides virulence factors of Cronobacter sakazakii, patient’s susceptibility, age, level of contamination of food, tolerance to temperature, speed of growth, infectious dose and biofilm formation [17] are critical factors contributing for increasing infections [66]. Biophysical growth factors such as the formation of biofilms are critical for Cronobacter sakazakii that makes this bacterium to be a potential pathogen [17]. Microbes either causing infection or spoilage can be attached to biotic or abiotic surfaces which have a detrimental impact on the medical and food sectors. When they are attached on these surfaces they come together within a group of microbial communities known as biofilms. These surface-attached microbial communities can be a source of continual contamination of foods that has food safety and economic implications [67]. As it has been reported this bacterium can tolerate desiccation which might be the attributes of biofilm formation. The other critical issue that is accompanied by biofilm formation is antibiotic resistance of microbes that worsen the problem. Cronobacter sakazakii showed multidrug resistance to some antibiotics [68]. A study conducted by Parra-Flores, et al. revealed that all isolated strains of Cronobacter sakazakii showed resistance to more than one antibiotic [21]. Biofilm formation and multiple antibiotic resistance were highly interconnected irrespective of the source, type, and environment of the isolates [19]. There was also a correlation between putative virulence factors and antibiotic resistance among the tested Cronobacter species [69].
From a food preservation point of view, hyperosmolarity and desiccation are paramount to hinder food spoilers and foodborne pathogens. However, this food preservation technique is not applicable for all groups of microbes because some groups of microbes encode mechanisms to survive and withstand these stresses [70]. The prolonged persistence of pathogens in the desiccated state is important especially in contaminating dried foods that have low water activity [47,71]. Cronobacter sakazakii can survive in such kinds of dried habitats and other hostile environments for long periods [7,17,72-74]. Cronobacter spp. adapt to dry stress in relative to other Enterobacteriaceae family membrers. The ability of this bacterium to tolerate desiccation is a tremendous advantage to persist in dry environments, such as in milk powder factories, on food processing surfaces and food preparation utensils and so that it can be source of post-contamination for the final food product [75-77]. The ability of this bacterium to produce biofilm is paramount in resisting dry and other hostile environmental conditions. This is because biofilm by its nature has a "spongy" like structure that can absorb water and prevent bacteria from desiccation. Therefore, biofilm is resistant to adverse conditions such as antibiotics, desiccation, and immune defenses and are key contributors to many chronic infections [78]. As a general Cronobacter sakazakii is more resistant than other Enterobacteriaceae to various environmental cues and stresses, such as low water activity, pH, temperature and dryness [77]. Biofilm formation, possession of virulence factors, high resistance to elevated osmotic, low pH, heat, oxidation, and desiccation are critical features of Cronobacter sakazakii that help this bacterium to survive in hostile dried foods such as powdered infant formula and cause disease in infants and other susceptible age groups [79]. Accessory genes, existing as sessile and planktonic life form, resistant genes, virulence and niche-specific genes enables Cronobacter sakazakii to adapt in diverse and hostile environments [64]. Generally, Cronobacter sakazakii can survive in extremely arid environments such as powdered infant formula and becomes a critical problem for all age groups, especially infants and neonates are highly susceptible age groups [73].
Biofilm is a microbial community that is attached to biotic or abiotic surfaces or interface onto each other and embedded in a self-produced matrix of extracellular polymeric substances [80]. Bacterial biofilm formation requires a series of stepwise processes accompanied by physiological and structural changes. This dynamical process comprises 1) Initial attachment; 2) Irreversible attachment; 3) Microcolony formation; 4) Maturation; 5) Dispersion [81] (Figure 1). Biofilm formation is cyclical, therefore, bacteria have the means to disrupt their biofilms and return to their free-form or planktonic lifestyle. For these cyclical events enzymes played a tremendous role in cleaving basic components of the biofilm matrix and thus weakening the biofilm architecture which allowed dispersion [82] (Figure 1). Biofilms formation on food and food processing surfaces depends on the interactions of different cues such as physical, chemical, and biological processes, nutrient availability and types, temperature, molecular cross-talks, production of extracellular polymeric substance (EPS), maturation of biofilm, and dispersal steps [83]. A plethora of bacteria including food spoilage bacteria and pathogens can have the ability to form biofilms on different surfaces such as food processing surfaces which could be a source of food contamination or spoilage [84]. This is because surface-attached microbial community harbor pathogens and food spoilers [67,85,86].
Cronobacter sakazakii is foodborne pathogen that can affect food safety by forming biofilms on a number of different food processing surfaces [86]. Cronobacter sakazakii forms a biofilm on the surfaces of equipment and processing environments which is an important source of persistent contamination in food samples. Biofilm of Cronobacter sakazakii on the surfaces of equipment and processing environments is an important source of persistent contamination in food samples [87] (Figure 3). The Cronobacter sakazakii has the potential to survive and persist on various biotic and abiotic surfaces such as preparation area in healthcare facilities and form biofilm communities that are more resistant to antimicrobial interventions [7]. As shown in Figure 1 persistent cells are escaped from their "caves" and dispersed and seek new conducive environments for their next phase. The ability to be attached to different surfaces, including rubber, silicon, polycarbonate, and stainless steel, is an evidence for the persistence of Cronobacter sakazakii on infant formula preparation equipment and in food-processing environments [16,52] (Figure 3 and Figure 4). Therefore, biofilm formation by Cronobacter sakazakii and other pathogens on enteral feeding tubes constitutes a risk factor for susceptible neonates [89] (Figure 3). As shown on Figure 3, Cronobacter sakazakii can be attached on the surface of spoons, trays, tin, and other materials used for reconstituting artificial infant feeding so that it will be source of contamination. Poor sanitation practice as well as biofilm formation on food contact surfaces, materials, and food processing environments has its own role on outbreaks of foodborne disease [90]. Cronobacter sakazakii has the ability to attach and form biofilm on infant-feeding equipment and preparation areas such as latex, silicon, enteral feeding tubes and stainless steel [88,91] (Figure 3 and Figure 4). Powder infant formula can be contaminated during production, reconstitution, addition of ingredients, handling or storage of reconstituted product [92] (Figure 3). As indicated on Figure 3 extrinsic contamination can occur when contaminated utensils such as spoons, blenders, bottles, teats are used for reconstituting or feeding PIF, or contamination may occur from the preparation environment [34]. Cronobacter sakazakii can cause infection via contaminated expressed breast milk, and it has been recovered from neonatal feeding tubes of neonates [21] (Figure 3). Therefore, we can infer that materials that we used for preparing infant feeds must be cleaned using appropriate methods, otherwise it will be source of contamination as depicted on Figure 3. From disinfection point of view Cronobacter sakazakii could produce biofilm and protect the cells from being affected by disinfectants. It is also more difficult to wash such bacteria off from the surface they attached with biofilm and the chance of cross-contamination could increase [93]. In addition to producing biofilm, their ability to grow in a wide range of temperatures is also paramount. Cronobacter sakazakii was able to grow in PIF at a wide range of temperature between 6 °C and 45 °C and its optimum temperature being 37 °C to 43 °C [88]. During preparation, handling, feeding, and storage the powdered infant formula might be subjected to different temperatures that can either increase or decrease the concentration of Cronobacter sakazakii [71].
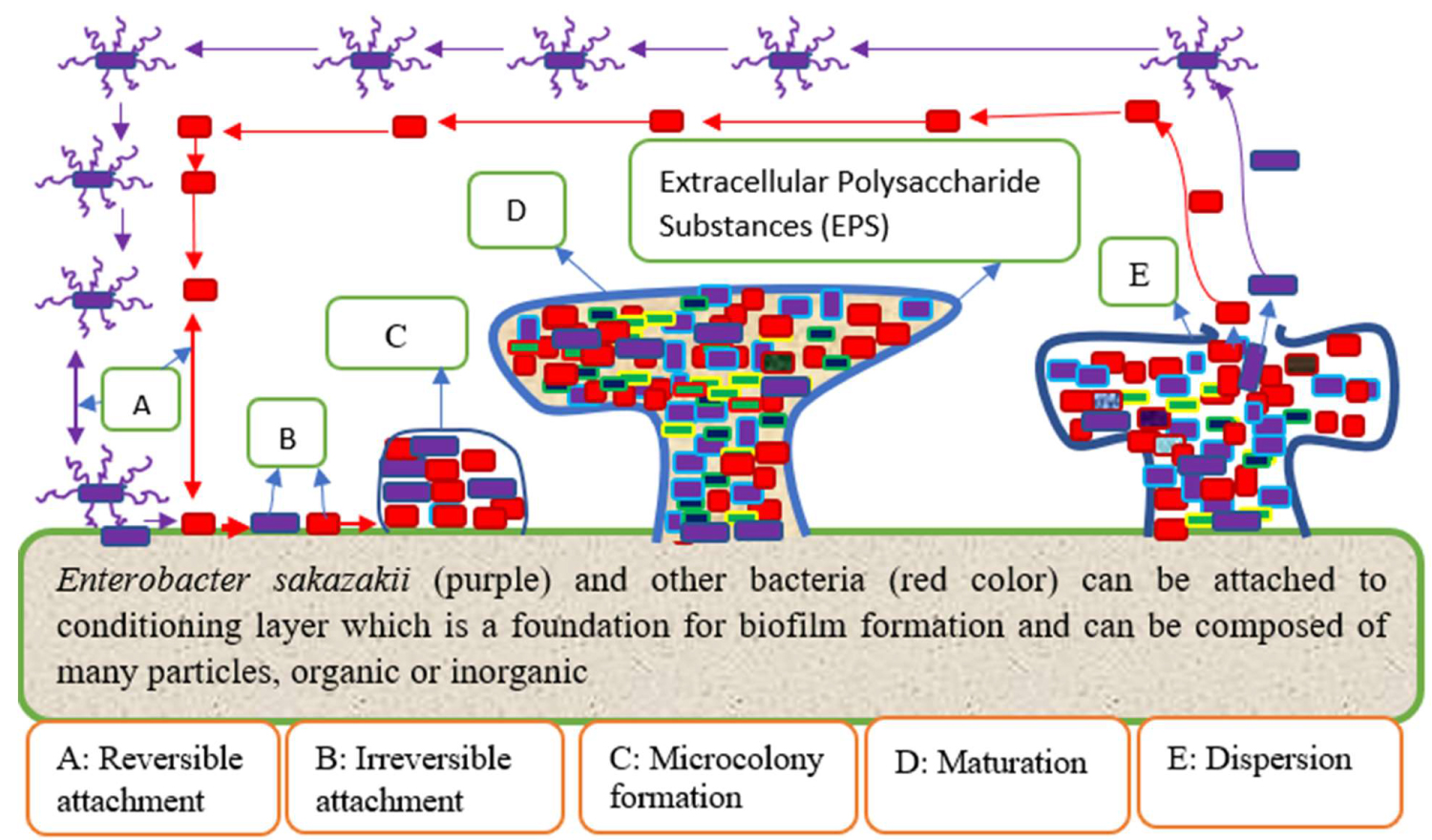 Figure 1: Stages of biofilm formation by Cronobacter sakazakii (own source). View Figure 1
Figure 1: Stages of biofilm formation by Cronobacter sakazakii (own source). View Figure 1
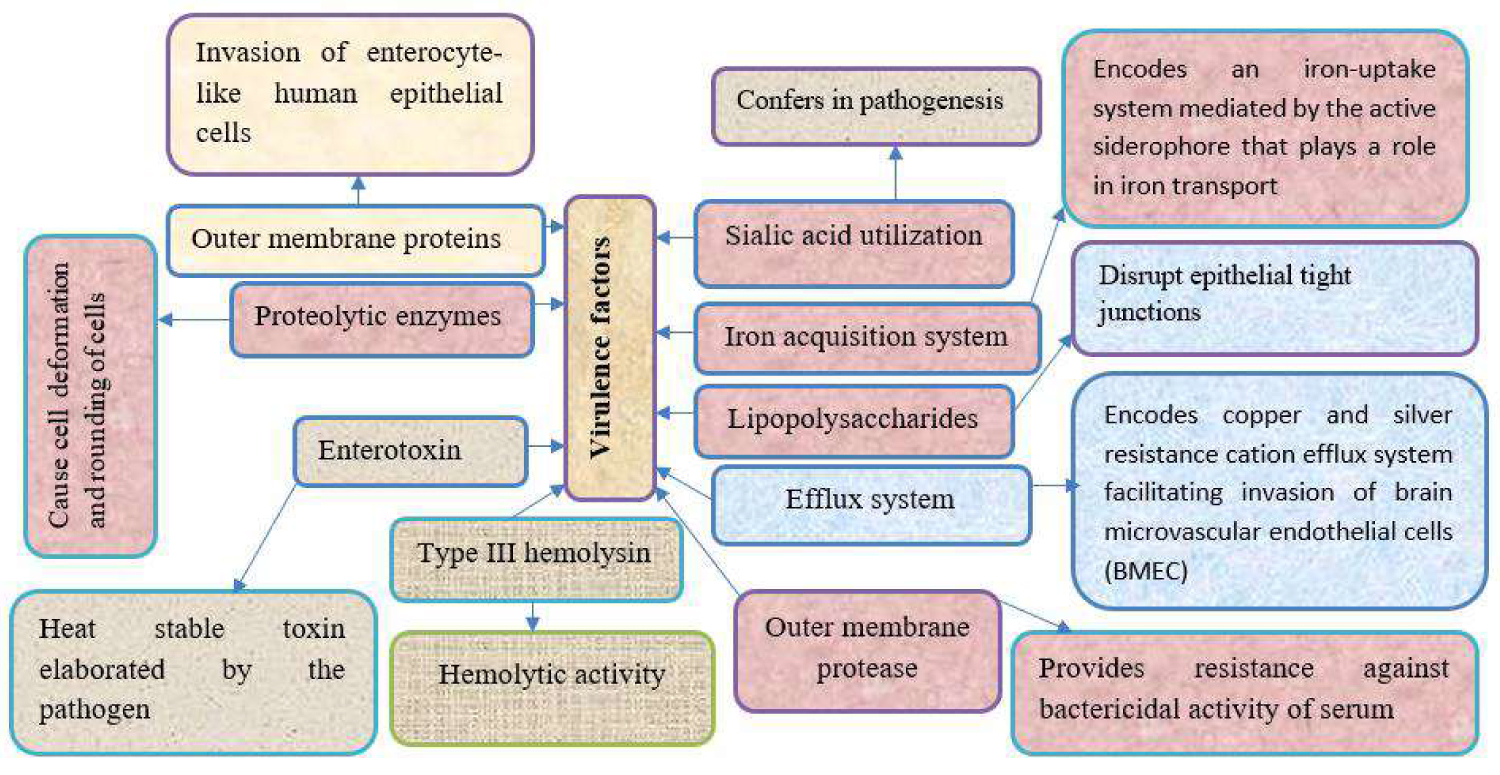 Figure 2: Virulence factors of Cronobacter sakazakii with their respective role [64]. View Figure 2
Figure 2: Virulence factors of Cronobacter sakazakii with their respective role [64]. View Figure 2
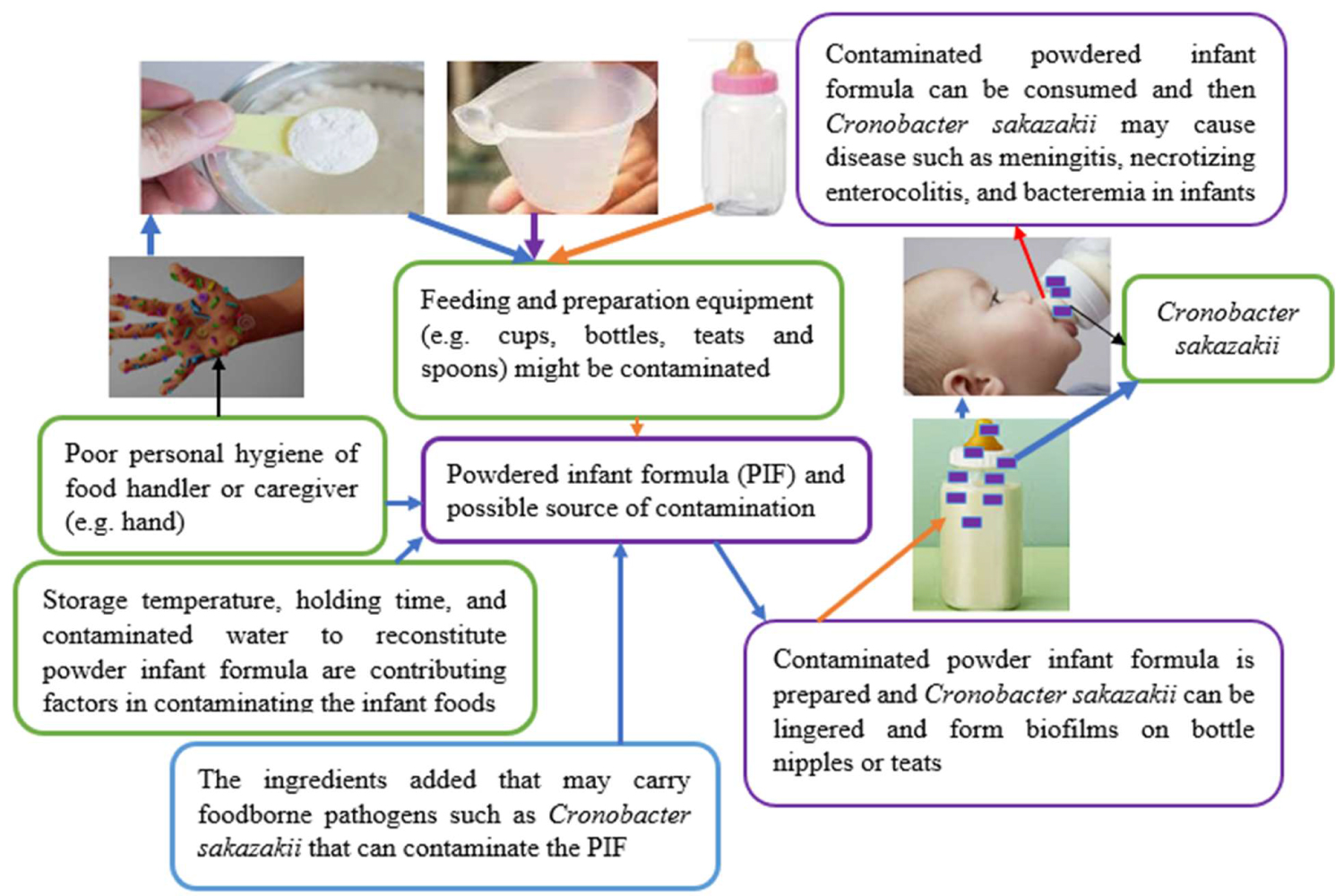 Figure 3: An example of possible source of bacterial cross-contamination [62] with major own modification. View Figure 3
Figure 3: An example of possible source of bacterial cross-contamination [62] with major own modification. View Figure 3
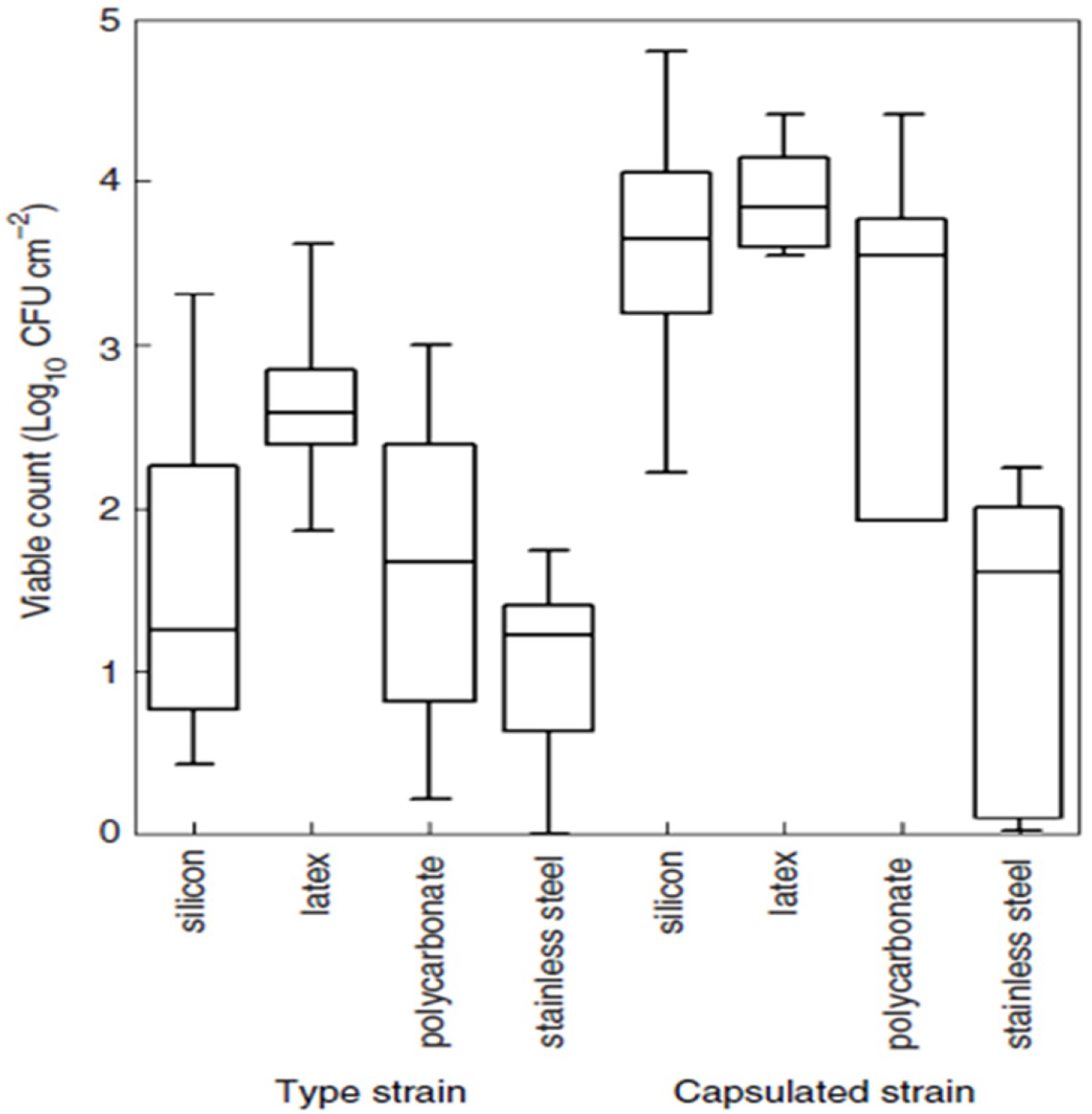 Figure 4: Biofilm formation by Cronobacter sakazakii on infant-feeding equipment and work surfaces using infant formula milk as growing medium [88]. View Figure 4
Figure 4: Biofilm formation by Cronobacter sakazakii on infant-feeding equipment and work surfaces using infant formula milk as growing medium [88]. View Figure 4
Therefore, knowing its optimum temperature is important to reduce their concentration that can be found either on the infant food or processing surfaces, and preparation equipment. Thus, the temperature of the water that we used to reconstitute or wash these materials must be beyond its optimum temperature to reduce or kill the attached bacterium. In addition to forming biofilms on the surfaces of these materials, reconstituted infant milk formula (IMF) is also a conducive nutrient for biofilm formation which can be source of contamination and infection [93]. Therefore, microbial biofilms are critical issues in food industry and food saftey, since biofilm formation on raw materials or food contact surfaces could be a sources of food contamination with spoilers or pathogenic microorganisms [27].
Antimicrobial resistance and microbial biofilm formation by bacteria lead to medical treatment failures [10]. The ability of bacteria to form biofilm and antibiotic resistance has a critical role in increasing bacterial pathogenicity and the risk of death. Antibiotic resistance is increasing with an alarming rate which poses a health hazard. If antibiotic resistance is increasing in such momentum really medication will be in trouble so that microbial infections will not be treated using antibiotics. Overdose utilization of antibiotics and spread of antibiotic resistant bacteria are the forefront factors for the emergence of resistance besides natural resistance [94]. Overdose utilization of antibiotics is just like "training bacteria" to develop resistant mechanisms from antbiotics and they will be fit for new antibiotics and challenge. Cronobacter sakazakii and Klebsiella pneumoniae isolated from PIF showed multi-drug resistant and produced enzymes such as extended spectrum β-lactamase (ESBL) that can inactivate antibiotcs. Even if this threatens infants worldwide, the severity is very high in developing nations where antibiotics were used wrongly [61]. A similar report also revealed that extensive utilization antibiotics will born multidrug-resistant bacteria that can devise their own mechanisms against new drug launched in the clinic [95]. Similarly, Cronobacter sakazakii is resistant to different antibiotics that worsen the medication. A study conducted by Kilonzo-Nthenge, et al. revealed that Cronobacter sakazakii showed multidrug resistance to penicillin, tetracycline, ciprofloxacin, and nalidixic acid [68]. However, as antimicrobial susceptibility test conducted by Fei, et al. revealed that Cronobacter strains were senstive to most of the antibiotics and whereas some strains were resistance to amoxicillin-clavulanate, ampicillin, and cefazolin [96]. In on the contrary to this report most Cronobacter spp. isolates were susceptible to ampicillin, tetracycline, and chloramphenicol [25]. As Kilonzo-Nthenge, et al. [81] reported Cronobacter sakazakii showed multidrug resistance to tetracycline. As so many research works indicated biofilm formation is accompanied by antibiotic resistance. Therefore, it can be said biofilm formation and antibiotic resistance are "two sides of the same coin". Biofim formation paves ways to antibiotic resistance. Physiological and structural change within biofilm enables microbes be resistant against most antibiotics. Structural barriers along with persist cells within biofilm plays a decisive role for antibiotic resistance [82]. Cronobacter sakazakii possess functional genes that are responsible for biofilm formation which may have the potential to cause risks to food safety [87]. Biofilm forming bacteria is resistant to antibiotics when when compared to their planktonic counterparts due to the above mentioned advantages [19]. Biofilms generally microbial protect the cells from antimicrobial action and other hostile environmental conditions so that they can stay for long periods by adhering to biotic or abiotic surfaces. As general antimicrobial resistance along with biofilm formation has become an escalating health threat and food safety worldwide.
Cronobacter sakazakii is one of the emerging and opportunistic pathogens linked with outbreaks of life-threatening necrotizing enterocolitis, meningitis, and sepsis in neonates, infants, and other susceptible age groups. Even if Cronobacter sakazakii can contaminate a wide range of foods, especially powdered infant formulas, it is underreported bacterium in different areas. Cronobacter sakazakii is also believed to be found in risky areas such as in refugee camps where they depend artificial feeding but no report found in such area. This bacterium has the potential to survive in dried environments for extended periods which allows it to persist in dried foods such as powdered infant formula and other foodstuffs. Biofilm formation by Cronobacter sakazakii paved the way for antibiotic resistance. Biofilm formation, dry resistance, and antibiotic resistance are not the only strategy but it is also armed with diversified virulence factors that can dismantle the host immune system. Generally, this bacterium is hidden bacterium that needs further investigation across the globe.
The following recommendations are forwarded based on the above review paper:
• The safety of the food can’t be maintained by a single person rather it is an issue of all individuals who are involved from farm to fork. All responsible person who is involved from the very beginning of its production up to consumption must give attention to contamination scenarios such as manufacture, processing, handling, preparation, storing, and reconstitution.
• If the health status of mothers is good enough, then there is no substitute for breastfeeding in terms of safety and nutrition. Breastfeeding advocacy is necessary and must be resumed. This is because powdered infant formula and other infant foods are the main vectors for Cronobacter sakazakii.
• Mothers and caregivers should be informed to follow up on the guidelines by prepared product manufacturer, WHO or FAO while they are reconstituting, preparing, and storing powdered infant formula.
• Cronobacter sakazakii is capable of forming biofilms on infant food processing surfaces and food preparation utensils such as spoons and bottle nipples or teats. Therefore, strict hygienic practice must be employed and the stakeholders should be seriously alerted to clean the feeding utensils especially bottle nipples or teats must be cleaned and disinfected frequently along with handwashing to prevent microbial attachment and biofilm formation. Additionally, the temperature of the water used for reconstituting the formula or washing these utensils must be sufficient enough to inactivate this bacterium.
• The current prevention methods appear to be insufficient to ensure that such foods are free of Cronobacter sakazakii. Therefore, the scientific community should device novel methods that can exclude this bacterium from infant foods without affecting the nutritive value of the food. Product recalling from the market will not solve the problem rather infant food companies and concerned bodies should formulate their protocols to check up and follow up any failures through food processing stages. Therefore, to detect any failures at the infant stages Good Manufacturing Practice (GMP) and Hazard Analysis and Critical Control Point (HACCP) and Cleaning-in-place (CIP) play pivotal roles that save the infant food companies from economic losses and health defects.
The data used to support the findings of this study are available from the corresponding author upon request.
I declare that there are no conflicts of interest in regard to the publication of this paper.
The author would like to thank Wolaita Sodo University but no fund is taken to conduct this research.