Gallstone ileus is an uncommon complication of calculous cholecystitis, which can lead to a gastro-intestinal obstruction. A non-specific clinical presentation is frequent. Imaging studies can present characteristic radiological signs. We present a 56-year-old female patient with constipation for the past 72 hours, colicky intermittent abdominal pain and vomiting. Plain CT-scan showed Rigler's triad. Gallstone ileus was diagnosed and laparotomy was performed with stone extraction by enterolitotomy. Significant morbimortality is associated to a delayed diagnosis more often in the context of elderly patients. Complementary imaging studies are needed for conclusive diagnosis, Rigler's triad, Petren and Forchet sign are pathognomonic for gallstone ileus. Surgical approach is essential in the resolution of this entity.
Gallstone ileus, Rigler's triad, Computerized tomography (CT), Enterolithotomy
Gallstone ileus (GSI) is an uncommon complication of cholelithiasis, and a rare cause of GI obstruction. This condition occurs when gallstones migrate to the bowel through a cholecystoenteric fistula, causing mechanical small bowel obstruction. The ileo-cecal valve is the most frequently affected, involved in 60-75% of cases [1-7]. It was described by Thomas Bartholin in 1654 [6].
Its etiology can be resumed as an impaction of a gallstone in the gastrointestinal tract after passing through a biliary-enteric fistula. It manages to open its way through the gallbladder wall, due to local "pericholecystic" inflammation and necrosis which results in erosion, adhesions and cholecystoenteric fistula [1,2,5].
This entity is seen in 0.3-0.5% of patients with a long history of cholelithiasis, other authors cite an incidence of 1-3% [2,4,5]. It accounts for 1 to 5% of non-strangulating mechanical small bowel obstruction cases in general population, and 25% in elderly patients [2,3,5,8,9]. It is more common in the older age group (> 60 years), average age of presentation is 74 years. These patients are usually frail, and with multiple comorbidities [10]. Female gender is more frequently affected with a rate of (3.5:1) [1,9], others authors cite as high as (6:1) [2].
The known risk factors are a long history of cholelithiasis, advanced age, repeated episodes of acute cholecystitis, stones > 2 cm [2,4], Ozer & Morosin, et al. reported up to 40-50% of patients diagnosed with gallstone ileus have antecedents of recent biliary colic bouts, jaundice and acute cholecystitis (30%) [2,5].
It is associated to a relatively high rate of morbidity and mortality (12-27%) due to a delayed presentation and diagnosis, secondary to non-specific symptoms [1,2,5]. Chang, et al. reported a mortality of (7-30%), average 18%, attributed to factors such as elderly or frail population, multiple comorbidities; cardiovascular, respiratory, and endocrine (diabetes and obesity), as well as late presentation from the onset of symptoms or delayed diagnosis [10].
Clinical presentation is usually non-specific and intermittently. The average duration of onset of symptoms preceding hospital admission is ± 5 days [6]. Physical examination may also be non-specific, with intermittent nature of symptoms [1,5].
Imaging studies such as X-ray and CT-scan can present characteristic radiological signs. CT-Scan sensitivity, specificity and accuracy is reported as 93%, 100% and 99% respectively specially when oral contrast is applied [2,5,6,11,12].
Since natural stone exclusion occurs infrequently (approximately 1.3%), surgery is indicated for cases of gallstone ileus involving stone extraction and closure of the fistula [13].
A 56-year-old woman with a long history of gallstones presented to the emergency department with constipation for the past 72 hours and colicky intermittent abdominal pain that partially improved with vomiting. In her past medical history there is reference to arterial hypertension, obesity, type 2 diabetes and hypercholesterolemia. She had experienced in the last year multiple episodes of biliary colic, treated with medical management. No surgeries and important family background of diseases are reported.
The patient's vital signs were stable at the time of admission. Abdominal examination demonstrated a generalized tenderness to palpation, without peritoneal irritation signs, and empty rectal ampulla at the digital rectal examination. Laboratory findings were within normal parameters.
She was initially treated with intravenous fluids, antibiotics and a NG tube with no improvement in her clinical status.
Radiological examinations were performed, the CT scan demonstrated an ectopic, obstructing, partially calcified jejunal intraluminal stone, with approximate dimensions of 4 × 4 cm, signs of small bowel obstruction with dilated jejunal loops above the obstruction, and signs of incipient pneumobilia "Rigle's triad" (Figure 1).
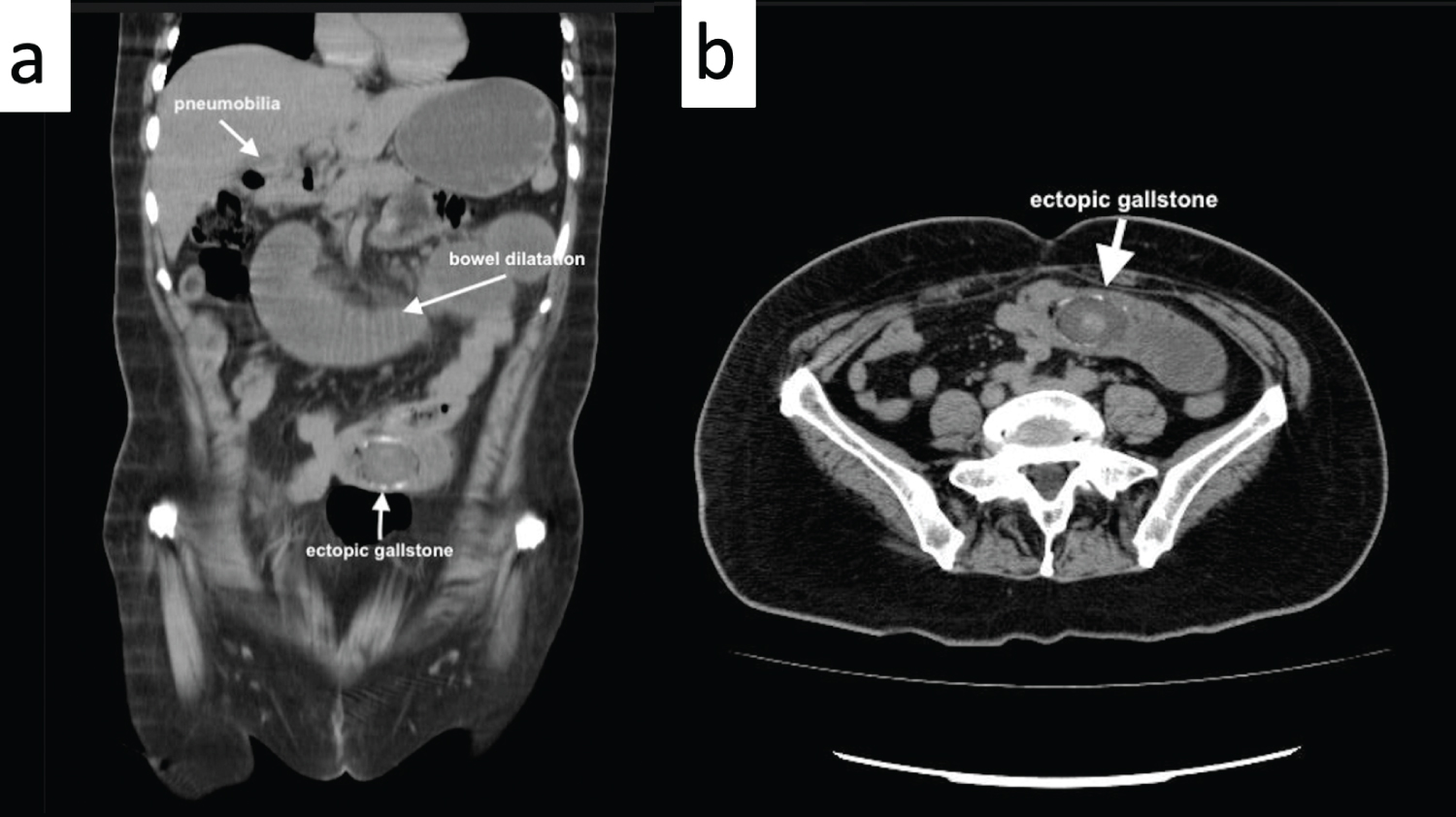 Figure 1: a) Ectopic gallstone; b) Rigler's triad; ectopic gallstone, bowel dilatation, pneumobilia.
View Figure 1
Figure 1: a) Ectopic gallstone; b) Rigler's triad; ectopic gallstone, bowel dilatation, pneumobilia.
View Figure 1
Patient underwent laparotomy. We identified a gallstone about 100 cm distant from the Treitz ligament, which caused total obstruction. Consequently, a transverse enterotomy was done, obtaining a 4 × 3 cm large gallstone, and the bowel was then closed transversally in two layers (Figure 2). Gallbladder and biliary tract exploration as well as surgical management were left for the second session. Operation concluded without complications.
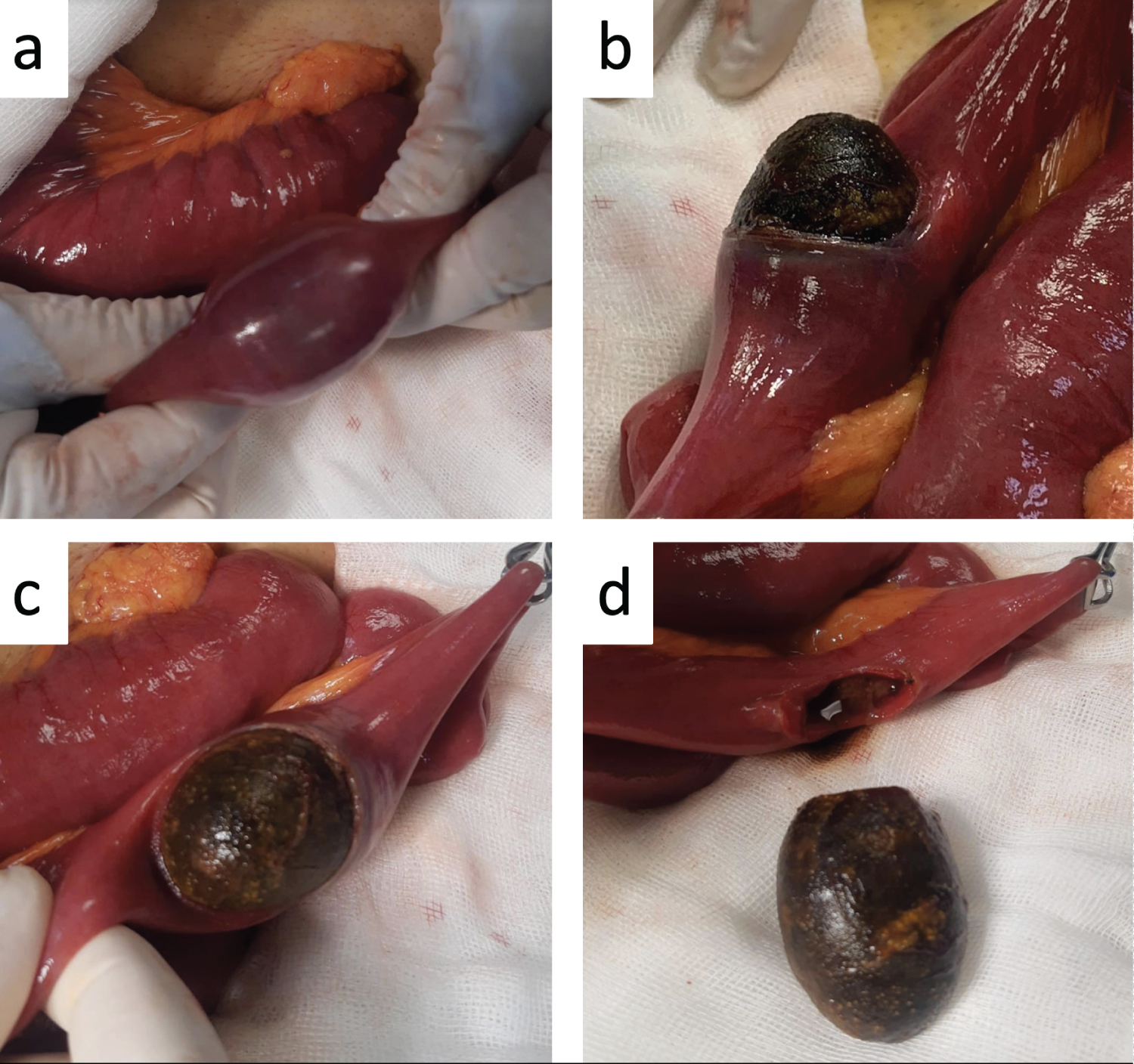 Figure 2: a) Jejunum occluded by a mass; b) Transverse enterotomy; c) Enterolithotomy; d) 4 × 3 cm large gallstone.
View Figure 2
Figure 2: a) Jejunum occluded by a mass; b) Transverse enterotomy; c) Enterolithotomy; d) 4 × 3 cm large gallstone.
View Figure 2
Antibiotic, postoperative pain control, and fluid therapy with nasogastric catheter continued. Patient presented gas outlet and adequate peristaltic movement in the following postoperative 48 hours, after that nasogastric catheter was withdrawn and diet was initiated. The patient was discharged with full recovery on the 5th post-operative day.
An important anatomic factor in GSI physiopathology is the proximity between the gallbladder and the duodenum, the most common of which is a fistulous connection between them (60-68%), "cholecystocolonic" transverse colon (5-25%), "Cholecysto-duodeno-colic (2.5%), "cholecysto-gastric or cholecysto-duodenal (1-3%) as a Bouveret's syndrome, and less frequently "cholecysto-jejunal" [1-4,14]. Another way that gallstone may enter the duodenum is through the common bile duct (dilated papilla of Vater, or after endoscopic sphincterotomy) [1,2]. In 85% of cases, gallstones are eliminated through feces or vomitus, the other 15% become entrapped in the gastrointestinal tract [4].
Stone size must be at least 2 cm in diameter to obstruct GI lumen (most frequently a big one > 2.5 cm). Sites affected usually have important narrowing in the bowel lumen and less peristalsis activity; terminal ileum and ileocecal valve (60-75%), proximal ileum and jejunum (20-40%), stomach (14%), sigmoid colon (4%) and duodenum (3-10%), the so-called Bouveret syndrome [1,5,6,15].
Some clinical features include signs of digestive tract obstruction; nausea, vomit, abdominal distension, constipation, and crampy or colicky generalized abdominal pain. Vomitus can be bilious due a small bowel obstruction, feculent when large bowel obstruction is present, or may appear coffee-ground [6,10]. Physical examination demonstration specific signs, including jaundice, abdominal distension and tenderness, with high pitched intestinal sounds [1,5]. Intermittent nature of constipation and other symptoms may be presenting in part due to the "tumbling phenomenon", secondary to temporary gallstone impaction followed by symptoms relief when the stones dislodges, travels distally and impacts again [5,6,10]. Sepsis presents either for cholecystitis or peritonitis due to impaction of the gallstone, causing pressure to the bowel wall with secondary necrosis and perforation [5,10]. In some other cases, as a Bouveret syndrome causing distal gastric or proximal duodenum impaction of the stone [2,3]. Clinically it can be divided in 3 major groups; "I: Acute classic gallstone ileus; II: Gallstone ileus with subacute recurrent attacks; III: Chronic gallstone ileus known as Kawersky syndrome" [2].
Radiological signs associated to GSI are Rigler's triad; pneumobillia or contrast material in the biliary tree, small bowel partial or complete obstruction signs (air-fluid levels, dilated small bowel loops), ectopic gallstone (usually right iliac fossa). The presence of two of the three signs is considered pathognomonic and it presents in 20%-50% of cases [2,5,12]. Petren sign described as the presence of air or oral contrast in gallbladder or biliary tree secondary to the transfection of the contrast agent from the fistula tract can also be identified. Another radiologic pattern is the Forchet sign (after oral contrast enhancement), which is the "snake head like" shape of the bowel lumen due to the obstruction, being unable of the contrast agent to pass the stone, and accumulate [2]. Endoscopy can be a useful adjunct to imaging studies for diagnosis and management of this condition [2,5,6].
Generally, GSI is managed by laparotomy, but with high morbidity (20-57%) and mortality (7-18%) associated. Laparoscopy has been evaluated and seems successful [15]. The current procedures are enterolithotomy alone, one-stage procedure of enterolithotomy, cholecystectomy and fistula closure and two-stage procedure of enterolithotomy with an interval cholecystectomy and fistula closure [14]. One stage surgery is excessively invasive, and associated postoperative complications are habitual. Regarding two-stage surgery has a disadvantage of associated risk of recurrence, retrograde cholecystitis, and cancer development due to remaining fistula [13]. Unfortunately, the question of whether interval biliary surgery should be performed remains unanswered.
The importance of a timely diagnosis of this entity falls in its marked morbidity and mortality given that delayed identification is associated with major bowel surgery, more often in the settings of emergency in elderly patients with multiple comorbidities, and the necessity of special postoperative care including intensive care unit (ICU) [11]. Clinical with a complementary radiological approach are needed for conclusive analysis. Surgery is required in the great majority of cases.