Giant hydronephrosis (GH) is defined as a dilated collecting system containing more than one liter of fluid. In this case we reported a 22-year-old man who presented acute onset abdominal pain, so an extension study: Computed tomography (CT) is performed finding a giant hydronephrosis (9037 cc).
We present this case in which percutaneous nephrostomy with slow decompression was done as initial treatment to relieve symptoms and prevent complications, later an open left nephrectomy was completed, without difficulties. The histopathology report showed obstruction of the pyeloureteral junction, which was not detected at birth. Therefore, we could not determine its congenital or postnatal origin.
Giant hydronephrosis, Nephrectomy, Abdominal distention
Giant hydronephrosis, characterized by the presence of more than 1 L of fluid in the renal collecting system, is a rare urological condition, particularly in adults [1]. Epidemiologically, the left kidney is commonly affected, the most common underlying causes include ureteropelvic junction (UPJ) obstruction and renal stone disease, and is often detected and treated in early childhood. It is a spectrum of pathophysiological processes of congenital (intrinsic stenosis, adynamic segment, mucosal valves and high insertion of the ureter) and acquired (scarring, reflux, malignant or benign tumors) etiologies [2].
The dilation of the renal pelvis and collecting system is a response to obstruction or urinary reflux; it reflects smooth muscle hypertrophy and accumulation of urine above the level of the obstruction. The pressure is transmitted to the delicate tubular system and leads to tubulointerstitial nephritis because of deposition of excessive amounts of extracellular matrix. The result is decreased glomerular filtration rate, decreased renal blood flow and nephron loss [3].
GH is a slowly progressive disease that may present as asymptomatic abdominal distension until the late phase or with vague symptoms, such as nausea, constipation, dyspepsia, fever, asthenia, mild diffuse abdominal pain or flank discomfort, chronic low back pain, recurrent urinary tract infections, and hematuria [4]. The majority of this condition will be diagnosed during childhood and infancy. If it is not treated early, it may cause progressive and gradual complications like hypertension, kidney rupture, renal failure, and malignant transformation because of prolonged irritation [5].
The differential diagnosis includes massive ascites, cysts (hepatobiliary, mesenteric, pancreatic, adrenal, echinococcal liver, and ovarian), splenomegaly, pseudomyxoma, and tumors [6]. Diagnostic tools include anterograde or retrograde urography and ultrasonography, but CT with contrast remains the gold standard for diagnosing hydronephrosis [7].
GH is managed surgically. Either nephrectomy or renal sparing therapy is performed based on residual renal function and the severity of symptoms. In the majority of cases, renal function is poor or absent, and nephrectomy is the usual method of definitive treatment. In our patient, the kidney did not produce urine after complete drainage of the hydronephrosis [8].
Nephrostomy drainage can be performed on patients who cannot undergo other treatments. If nephrectomy is feasible, progressive preoperative decompression is recommended to relieve symptoms, avoid hemodynamic disorders due to abdominal decompression, improve cardiopulmonary function, evaluate the function of the affected kidney, and perform preoperative anatomical analysis using CT to evaluate vascular features, such as polar vessels, that could explain the hydronephrosis [9]. Also, when there is a large staghorn calculus causing hydronephrosis, a nephrostomy decompresses the upper urinary tract initially and then provides access for percutaneous nephrolithotomy to allow definite fragmentation of the stone. Pelviureteric junction obstruction may be treated with pyeloplasty either by a laparoscopic or open approach [10]. Our objective is to report a case of an infrequent entity as the giant hydronephrosis.
A 22-year-old man was admitted to the Hospital General de Zona 1A (Mexico City, México) in October 2022 with a abdominal pain predominantly in the mesogastrium, abdominal distension, no alterations in bowel habits were reported, with evacuations present.
So an extension study: Computed tomography is performed, finding an oval lesion with regular and well-defined borders in the left hemiabdomen with general measurements of 358 × 174 × 279 mm and a volume of 9037 cc. After contrast administration it does not show abnormal enhancements with attenuation units of -2 HU (Figure 1).
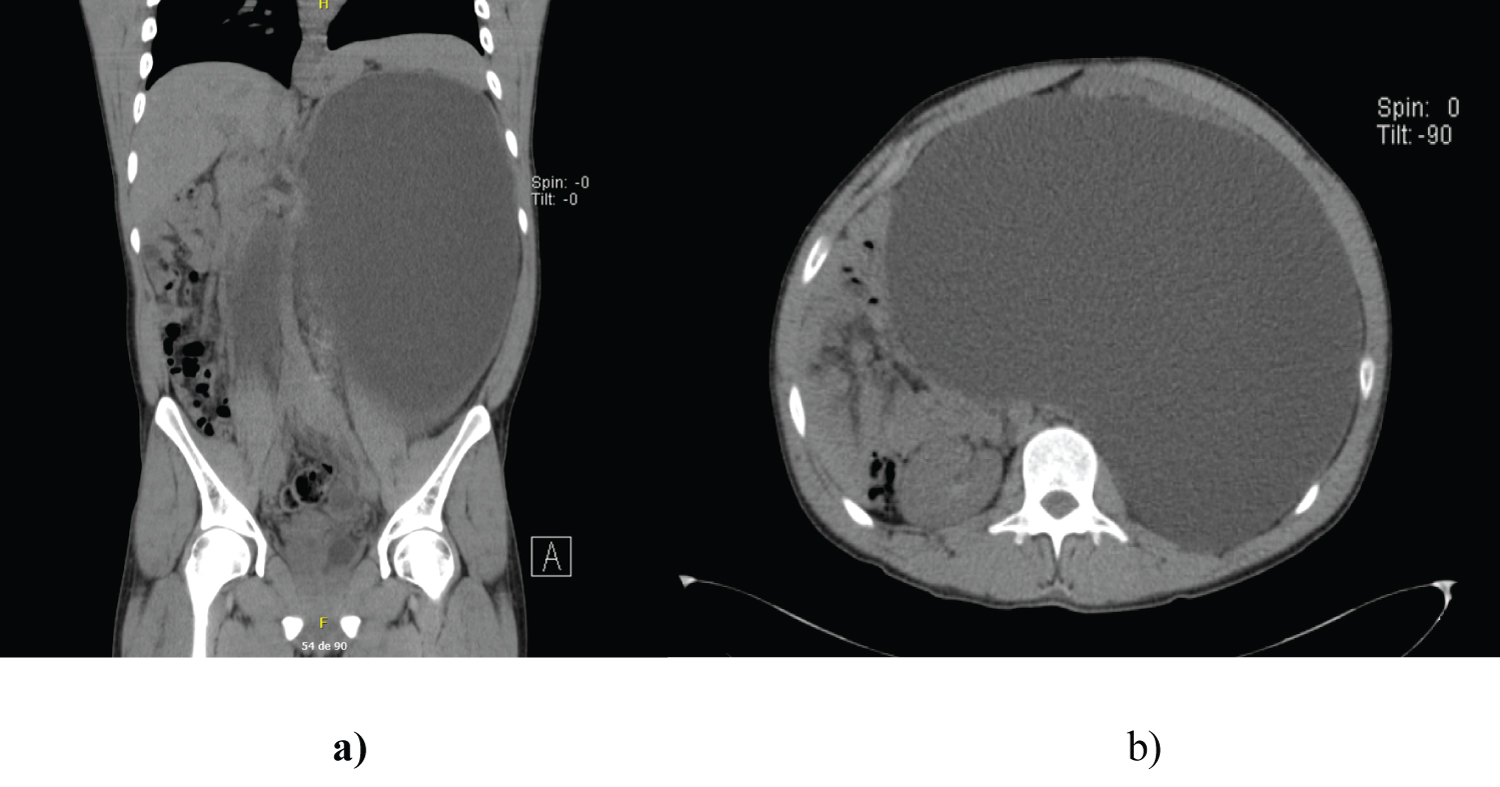 Figure 1: Computed tomography at admission. An oval lesion with regular and well-defined borders was observed in the left hemiabdomen of 358 × 174 × 279 mm and a volume of 9,037 cc. a) Coronal section b) Axial section.
View Figure 1
Figure 1: Computed tomography at admission. An oval lesion with regular and well-defined borders was observed in the left hemiabdomen of 358 × 174 × 279 mm and a volume of 9,037 cc. a) Coronal section b) Axial section.
View Figure 1
The patient had no significant family history. The vital signs of the patient were stable. Abdominal examination revealed non-define abdominal tumor, predominantly in the left hemiabdomen. Other physical examinations were unremarkable.
Blood tests revealed that the patient's white blood count was 5.4 × 109 cells/l, Albumin 3.8 gr/dl, Hemoglobin 14.5 gr/dl, Creatinine 1.2 gr/dl, Urea 31.4 gr/dl Other laboratory examinations were all negative, including those for blood chemistry, blood tumor markers, and liver function.
Cultures were negative, and no atypia was detected in the urine cytology. The nephrostomy was kept open until surgery.
A preoperative CT scan with arterial and late phase showed almost complete regression of the hydronephrosis without any vascular anatomical anomalies (Figure 2). After 4 weeks of complete drainage, the patient underwent a left nephrectomy. Intraoperative findings revealed a giant hydronephrotic left kidney with a 20 × 25 cm hydronephrotic sac, Bleeding: 300 ml (Figure 3). The nephrectomy was performed without complications. Pathological analysis of the nephrectomy specimen showed obstruction of the pyeloureteral junction.
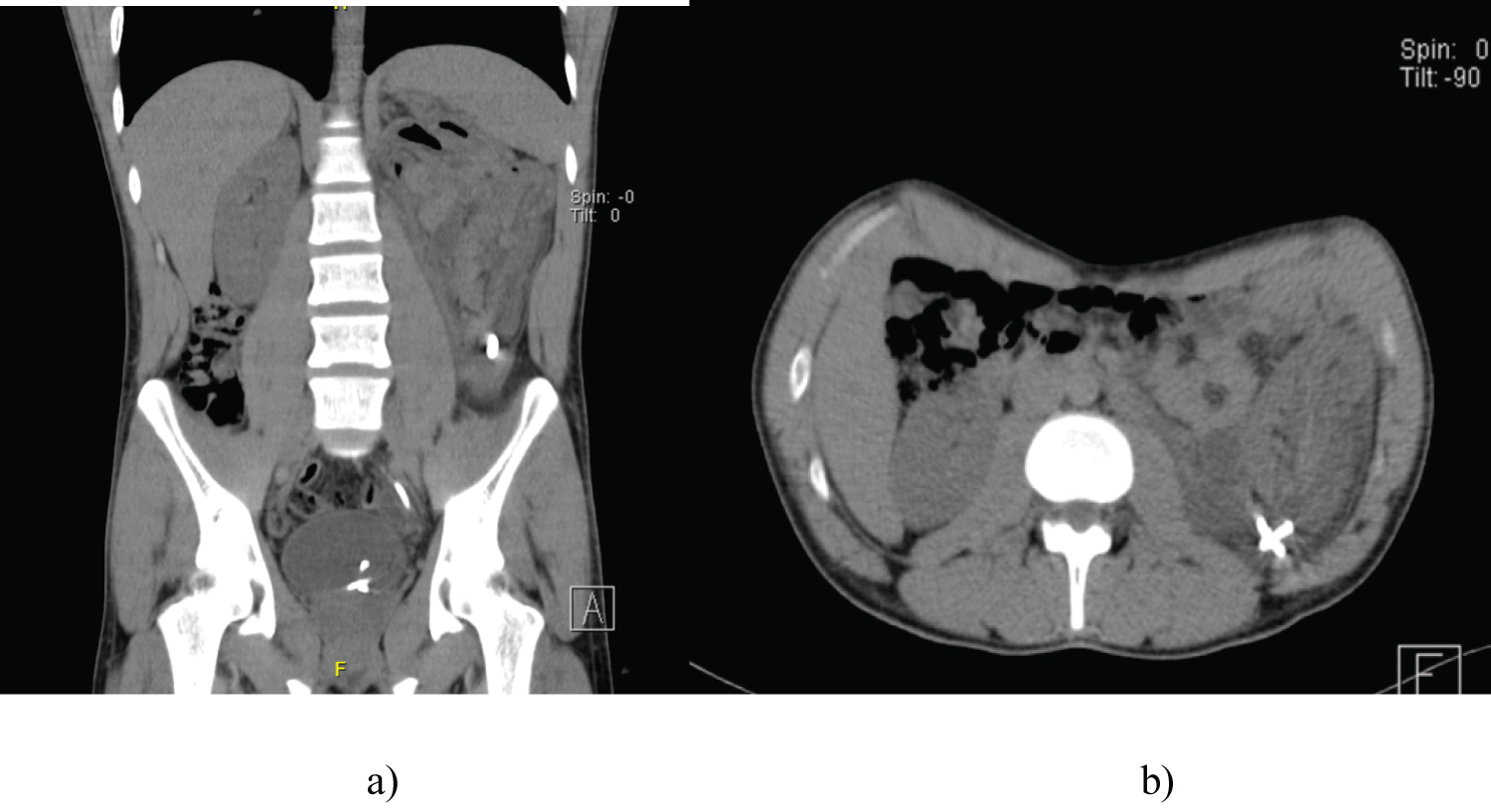 Figure 2: Abdominal computed tomography after nephrostomy placement. a) Coronal section b) Axial section.
View Figure 2
Figure 2: Abdominal computed tomography after nephrostomy placement. a) Coronal section b) Axial section.
View Figure 2
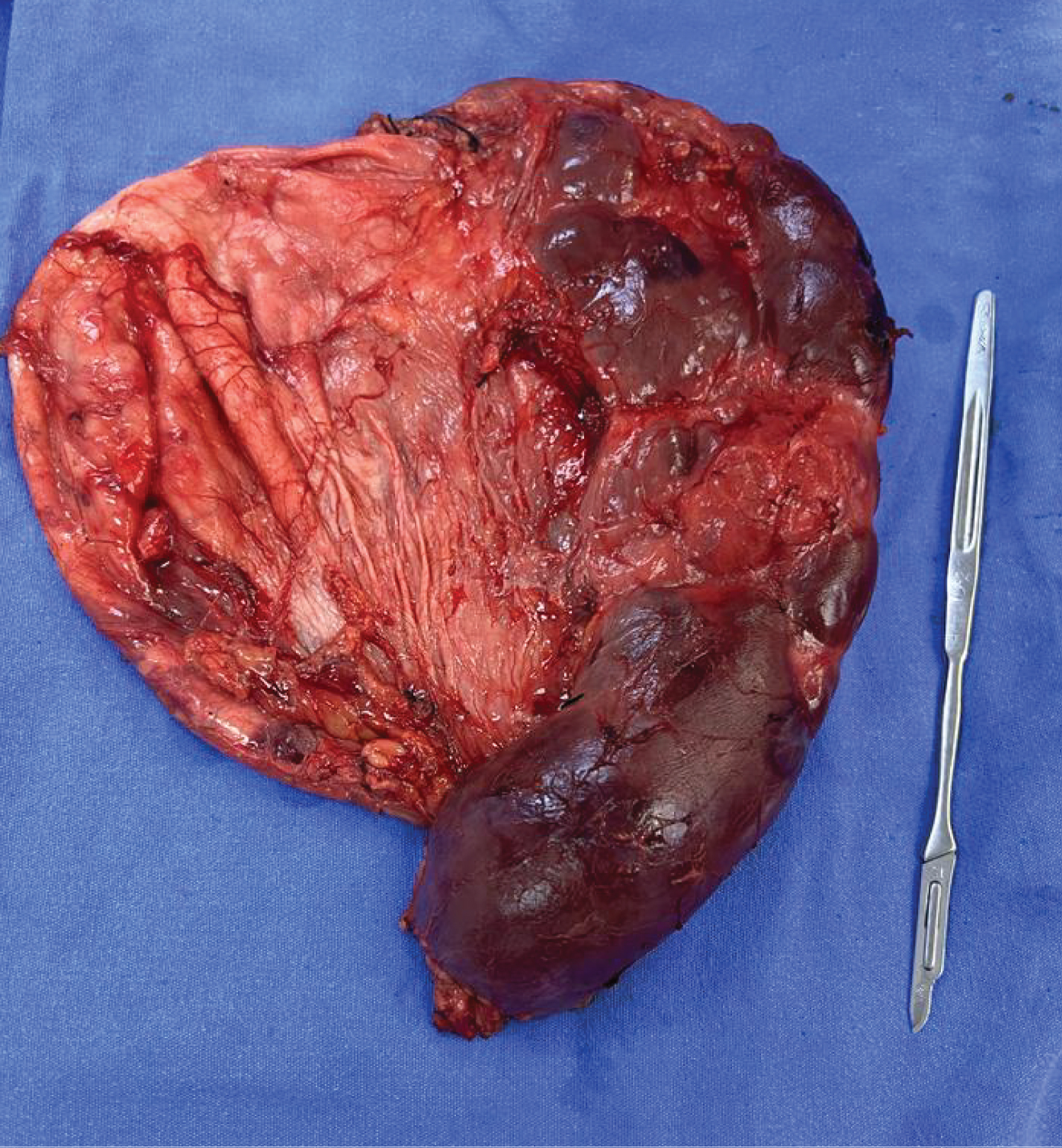 Figure 3: Surgical specimen.
View Figure 3
Figure 3: Surgical specimen.
View Figure 3
Hydronephrosis is a persistent and progressively increasing expansion of the collecting system, accompanied by urine retention due to the outflow obstruction. The most frequent causes are congenital abnormalities. Acquired causes include urolithiasis, strictures due to postoperative or inflammatory changes, adhesions, polyps and malignant neoplasms. GH was defined by Stirling in 1939 as a kidney containing more than 1L of fluid in its collecting system or a kidney weighing more than 1.6% of body weight [11].
These patients clinical symptoms are not specific, but they commonly include increased abdominal girth and distended abdomen. Other manifestations include flank pain, hematuria, chronic abdominal pain, and repeated urinary tract infections. Even with its vague and general clinical manifestations, only 50% of giant hydronephrosis cases have been correctly diagnosed in the past [12]. In our case, the diagnosis was made based on clinical symptoms and a computerized tomography scan imaging study.
The treatment modality described includes percutaneous nephrostomy insertion, reconstructive surgery such as ureterocalicostomy, dismembered pyeloplasty, calycovesicostomy, and laparoscopic and open simple nephrectomy. The treatment option is deepened on patient condition, renal functional status, and surgeon experiences [13]. In a patient with loss of renal function, and thin cortical thickness, simple nephrectomy is the optimal choice because of the expected complications such as infections and tumor changes. A puncture/drain procedure such as nephrostomy insertion may be performed if the patients' condition precludes other treatments or if hemodynamic instability occurs due to a sudden abdominal rupture. Like in this case, and then giant hydronephrosis was effectively treated with simple nephrectomy [14].
Giant hydronephrosis as a result of ureteropelvic junction obstruction; is defined as a dilatation of the pelvicalyceal system comprising more than one liter of urine, causing swelling in the hemiabdomen, or crossing the midline with a cover of five vertebral lines. It is commonly represented on the left side and in men more than in women (male to female ratio: 2.4:1). Most ureteropelvic junction obstruction cases are discovered during early life or infancy.
Historically, only 50% of giant hydronephrosis cases are properly diagnosed because of its nonspecific clinical presentation. However, imaging techniques have been improved dramatically in recent years. Using ultrasonography, other useful diagnostic imaging techniques include abdominal radiography with observable radiopaque lithiasis, intravenous urography showing no excretion in the affected kidney, and CT.
GH is a rare urological entity that requires individualized management depending on the salvage capacity of the affected kidney and the accessibility of kidney sparing treatment. Renal drainage improves the patient’s condition and reduces the risk of postoperative complications.
To all staff in charge of patient care at the hospital.
This research has not received specific support from public sector agencies, commercial sector or non-profit entities.
The authors declare that they have no conflict of interest.
The authors declare that patient consent was obtained, which is in accordance with the policies and standards of our institutional ethics committee. No patient-identifying information is presented in this article, thus anonymity is preserved. No animal and/or human experiments were performed.