Introduction: Prevalence of GSD has been 10-20% in developed countries, 2.5-10% in African populations, and 3.1-6.1% in Asians. Approximately 3-8% of GSD patients experience complications, including cholecystitis, gallstone ileus, pancreatitis, empyema, and gallbladder perforation. Therefore, GSD care could be expensive and place a considerable burden on the budget of health systems.
Case report: A 57-year-old female admitted to the emergency room due to oral intolerance and abdominal pain. In the ER, she presented abdominal distension, inability to pass bowel motions or gas, with the requirement of nasogastric tube placement, and discharge with intestinal characteristics was obtained, upon admission leukocytosis of 20,000 with neutrophilia. CT scan showed a stone of probable biliary origin impacted in the terminal ileum, pneumobilia, and uncomplicated diverticular disease. She was evaluated by general surgery, performing exploratory laparotomy with the following findings: Impacted gallstone at 20 cm from the ileocecal valve, distended small bowel loops, no evidence of ischemia, and scant peritoneal reaction fluid. Enterolithotomy was performed 30 cm from the ileocecal valve plus primary closure with Heineke-Mikulicz technique.
Discussion: Gallstone ileus is a mechanical small bowel obstruction induced by an impacted ectopic gallstone. The terminal ileum and ileocecal valve are the most common sites of gallstone impaction. Generally, gallstones < 2-2.5 cm have a high probability of spontaneous transit. Gallstone ileus is a rare long-term complication of cholelithiasis. Risk factors include female gender, age > 65 years, history of episodes of untreated cholecystitis, and larger stones (> 2.5 cm).
Gallstone ileus, Bowel obstruction, Surgery, Enterolithotomy
Gallstone disease (GSD) is a common gastrointestinal disease of the digestive tract and one of the leading causes of hospital admissions for gastrointestinal problems. The prevalence of GSD varies between different countries and with ethnicity. GSD is more common in developed countries than in low-income and middle-income countries. The prevalence of GSD has been 10-20% in developed countries, 2.5-10% in African populations, and 3.1-6.1% in Asians. Approximately 3 to 8% of GSD patients experience complications, including cholecystitis, gallstone ileus, pancreatitis, empyema, and gallbladder perforation. Therefore, GSD care could be expensive and place a considerable burden on the budget of health systems [1].
A gallstone ileus is usually a late complication of gallbladder disease, accounting for 1 to 4% of all mechanical bowel obstructions, especially in the elderly. It usually occurs in women and patients with a history of Choledocholithiasis. Intestinal impaction is due to a gallstone that enters the intestine through a cholecystoenteric fistula. The mortality rate is considerable, ranging from 12 to 27%. Clinically, it presents the usual signs and symptoms of intestinal obstruction, and abdominal CT is the best diagnostic method. Treatment in most cases is surgical, focused on resolving the intestinal obstruction. The most effective treatment is the mechanical removal of the cause of the obstruction, usually by surgical intervention, involving an enterolithotomy [2].
Laparotomy enterolithotomy is the most reported surgical procedure [3] and is currently considered a promising approach for patients with significant comorbidities, hemodynamic instability, or high-risk surgical dissection. Reisner and Cohen compared mortality in patients who underwent enterotomy alone and patients who underwent one-stage surgery and found a mortality rate of 12% for patients who underwent enterotomy alone versus 17% for patients who underwent surgery at one time. In this case, given the patient's age and her comorbidities, this was also the technique of choice [4].
Admitted a 57-year-old female to the emergency room due to intolerance to the oral route and abdominal pain. No significant background to the case. His condition began a week before his admission with colicky abdominal pain in the epigastrium and hypochondria, accompanied by evacuations that decreased consistency, nausea, and vomiting of "countless" gastro biliary content. Management began before admission with spasmolytics, antiemetics, analgesics, and temporary improvement and he came for evaluation at this hospital due to the persistence of symptoms. In the emergency area, he presented with abdominal distension and absence of evacuations and gas channeling, for which was placed a nasogastric tube, and discharge with intestinal characteristics was obtained, upon admission with laboratories in which leukocytosis of 20,000 stood out, at the expense of neutrophilia, without hydroelectrolyte imbalance, liver function tests without alterations, and slight elevation of nitrogen dioxide. A CT scan showed a stone of probable biliary origin impacted in the terminal ileum, pneumonia, and uncomplicated diverticular disease (Figure 1 and Figure 2). She was evaluated by general surgery, performing exploratory laparotomy. The following findings were obtained: Impacted gallstone 20 cm from the ileocecal valve, distended small bowel loops, no evidence of ischemia, and scant peritoneal reaction fluid. Enterolithotomy was performed 30 cm from the ileocecal valve (Figure 3) plus primary closure with the Heineke-Mikulicz technique in two planes (Figure 4 and Figure 5). During the postoperative period, the patient had an adequate evolution; the flow through the nasogastric tube ceased, and she started the oral route with adequate tolerance; she presented evacuations with typical characteristics 48 hours after surgery, and the drainage was maintained without flow until, after her withdrawal, she was discharged 72 hours later due to improvement. Follow-up continued via outpatient clinic with an elective cholecystectomy plan.
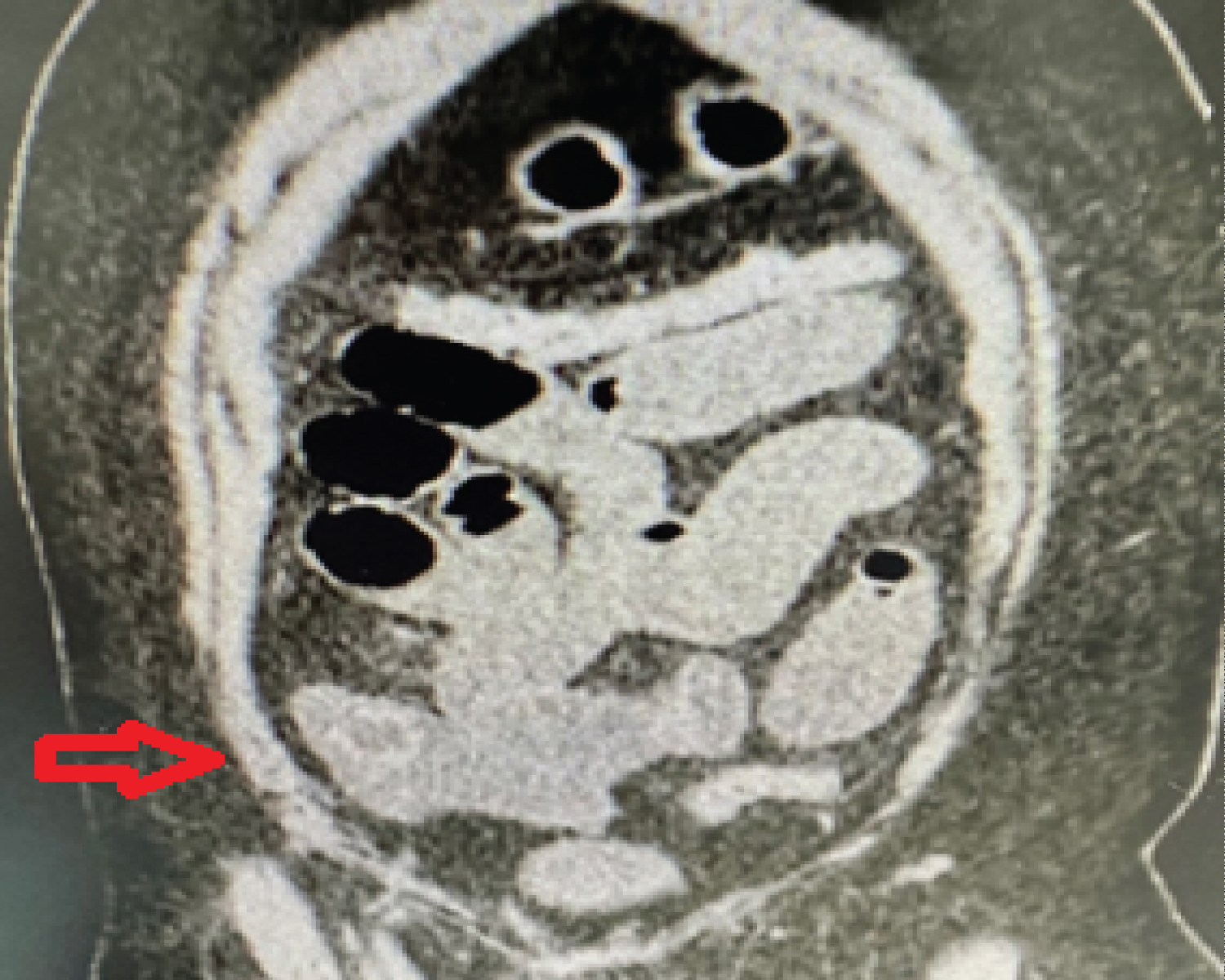 Figure 1: CT scan is axial and coronal cut showing impacted stone in the terminal ileum.
View Figure 1
Figure 1: CT scan is axial and coronal cut showing impacted stone in the terminal ileum.
View Figure 1
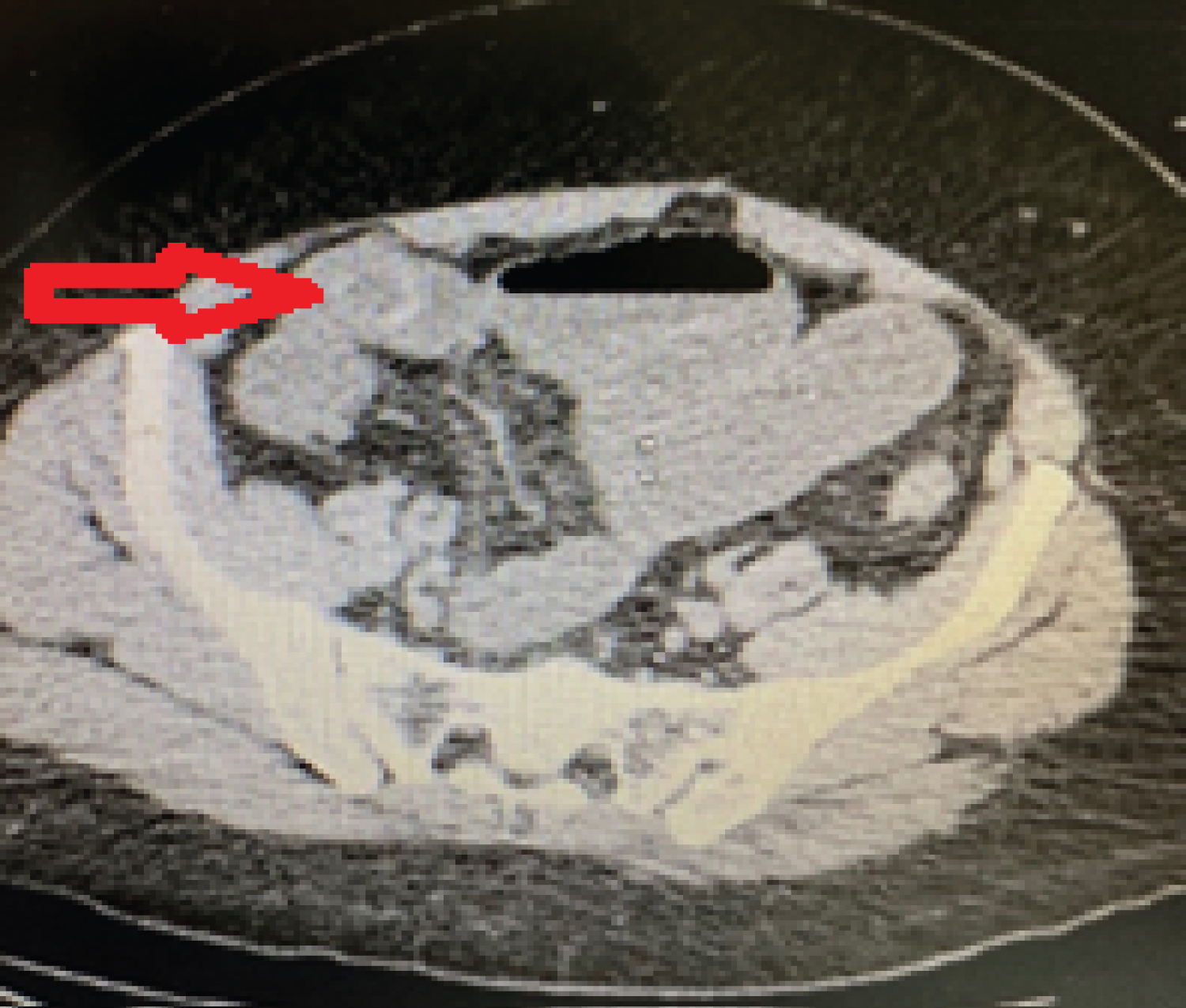 Figure 2: CT scan is axial and coronal cut showing impacted stone in the terminal ileum.
View Figure 2
Figure 2: CT scan is axial and coronal cut showing impacted stone in the terminal ileum.
View Figure 2
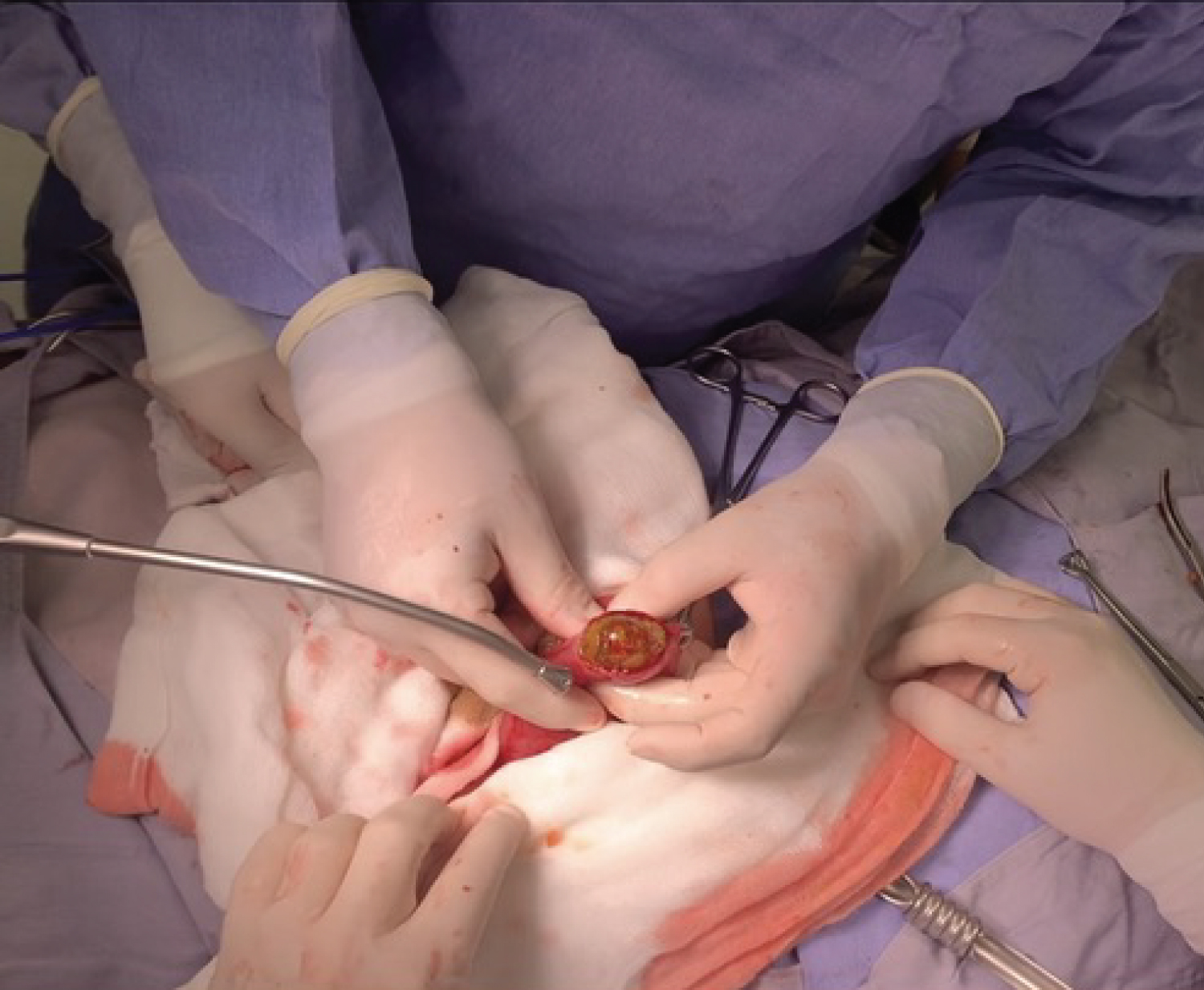 Figure 3: Biliary stone 3 cm in diameter, extracted 30 cm from the ileocecal valve through enterotomy.
View Figure 3
Figure 3: Biliary stone 3 cm in diameter, extracted 30 cm from the ileocecal valve through enterotomy.
View Figure 3
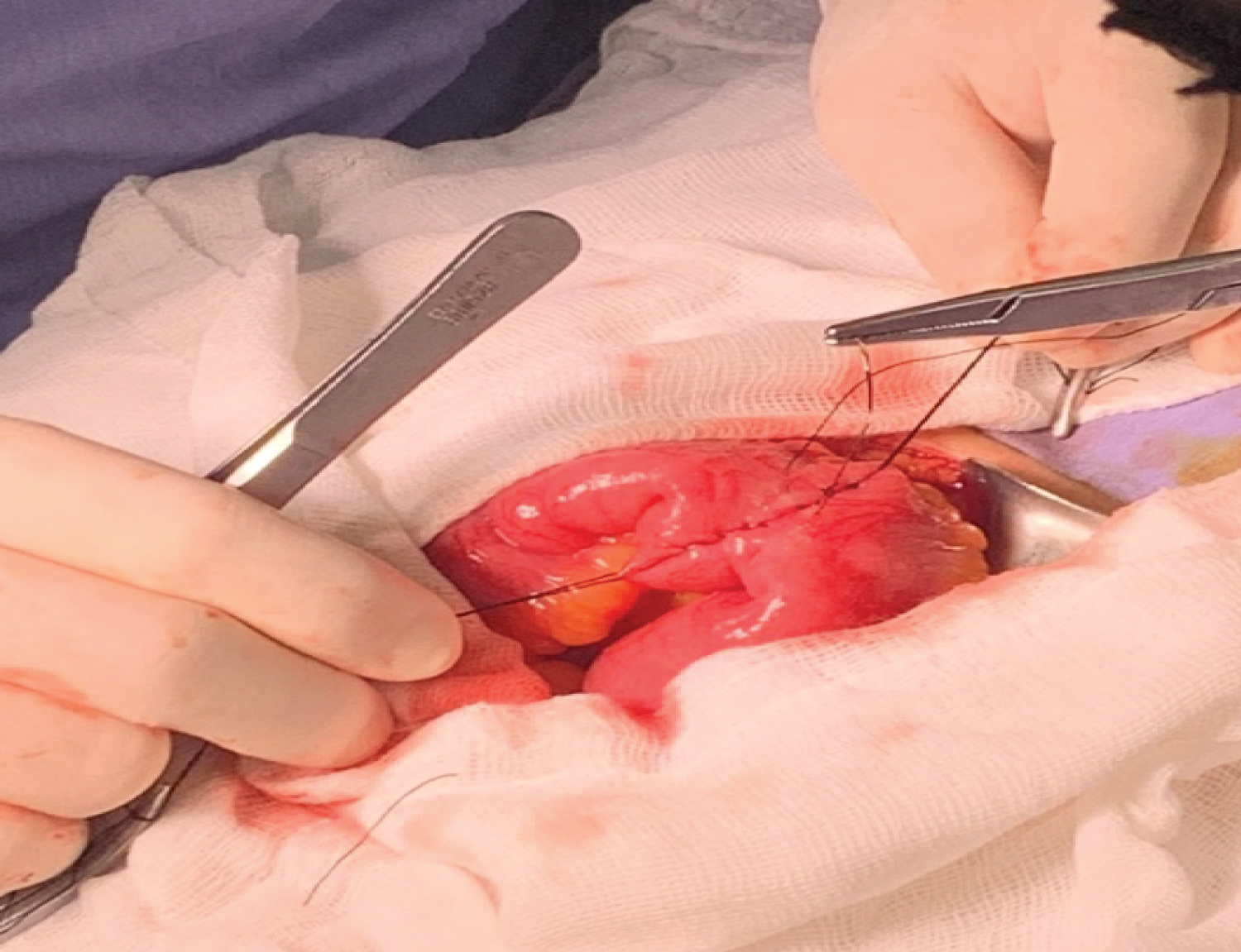 Figure 4: Primary closure of the terminal ileum with the Heineke-Mikulicz technique.
View Figure 4
Figure 4: Primary closure of the terminal ileum with the Heineke-Mikulicz technique.
View Figure 4
 Figure 5: Biliary stone 3 cm in diameter.
View Figure 5
Figure 5: Biliary stone 3 cm in diameter.
View Figure 5
Gallstone ileus is a mechanical small bowel obstruction induced by an impacted ectopic gallstone. The terminal ileum and ileocecal valve are the most common sites of gallstone impaction. Generally, gallstones < 2-2.5 cm have a high probability of spontaneous transit. Gallstone ileus is a rare long-term complication of cholelithiasis. Risk factors include female gender, age greater than 65 years, a history of episodes of untreated cholecystitis, and larger stones (> 2.5 cm). Inflammatory changes, pressure erosion, and ischemia of the gallbladder wall could lead to fistula in patients with a long history of gallstone disease. The most common fistula is cholecystoduodenal fistula (33-97%), followed by stomach, small intestine, and colon involvement [5].
Strong clinical suspicion is necessary for early diagnosis of this condition. Nonspecific and intermittent symptoms, misdiagnosis, or late diagnosis cause high morbidity (20-57%) and mortality rates (7-18%) in this condition compared to other causes of small bowel obstruction. The median duration of symptom onset and delay in diagnosis is six days. A delay in diagnosis leads to complications, including dehydration, shock, sepsis, or peritonitis [6].
Radiological images are the cornerstone of early diagnosis of gallstone ileus. Rigler's triad, including pneumonia, small bowel obstruction, and ectopic gallstones, represent the pathognomonic findings. Treatment options include surgery (closure of the fistula in one or two stages) or conservative (natural closure of the fistula) [7].
Souiki T, et al. [3] report a case where computed tomography of the abdomen showed dilated small bowel loops upstream of a large gallstone with a calcified rim. These findings are consistent with gallstone ileus. After adequate resuscitation with intravenous fluids, the patient underwent an emergency midline mini-laparotomy. Surgical exploration revealed the presence of a gallstone in the ileus causing intestinal obstruction. Was removed the gallstone by longitudinal enterotomy, and the defect was closed transversely. Given the high anesthetic risk for the patient and the need for a shorter laparotomy, it has been decided not to treat cholecystitis and entero biliary fistula. The patient had an uneventful recovery and was symptom-free within six months of follow-up.
CT scans are a reliable tool and often the first imaging modality in these patients. However, in some instances, they may not visualize the gallstone. Magnetic resonance imaging is the gold standard imaging modality for radiolucent gallstones; however, in Asia-Pacific, it is infrequently used as a first-line investigation, especially in intra-abdominal surgical conditions, due to study scarcity and cost. Magnetic resonance imaging (MRI) is well regarded as the gold standard for detecting radiolucent and attenuating stones that would otherwise go undetected on radiographs and CT scans. However, it does not usually play a role in the acute setting for intra-abdominal surgical presentations, especially in Asia Pacific. Moreover, while gallstone ileus has been described in the literature, no reports of MRI in the acute setting being used for diagnostic purposes have been reported. Therefore, if there is a high index of suspicion for gallstone ileus, gallstone ileus warrants expedited MRI to confirm the diagnosis due to the urgency of management [8].
Although more extensive comparative studies are required, preliminary analyzes suggest that intraoperative indocyanine green fluorescence cholangiography markedly reduces the rate of common bile duct injury. A lower rate of common bile duct injury and conversion to open surgery with fluorescence cholangiography was found in six and 16/10,000 vs. 25 and 271/10,000 cholangiography with and without fluorescence. Considering the risk of common bile duct injury and the risk of recurrence in a patient without comorbidities can be performed open cholecystectomy using fluorescence cholangiography. They can correctly identify the common and cystic bile ducts to generate an adequate critical view of safety and prevent injuries to the common bile duct despite the severe inflammatory process [9-11].
Fluorescence with indocyanine green. Since its clearance is hepatic, it allows effective visualization, using fluorescence systems, of the entire biliary anatomy and reduces complications. To minimize common bile duct lesions, there are multiple strategies to perform a safe cholecystectomy: the critical view of safety, intraoperative cholangiography, steps proposed for a safe cholecystectomy by different societies, and, recently, the use of intraoperative cholangiography.
In a recent meta-analysis, including 481 patients, it was compared to the ability to visualize the extra-hepatic biliary tree structures of routine intraoperative cholangiography with indocyanine green fluorescence cholangiography. They found that fluorescence provided the exact visualization of the cystic duct and the junction of the cystic duct with the common hepatic duct compared with routine intraoperative cholangiography. However, better visualization of the common hepatic duct was obtained with fluorescence and bypassed cystic duct canalization [9].
They have reported Spontaneous resolution in only 1.3% of gallstones > 2-2.5 cm cases. The literature reports that, in cases of spontaneous resolution, the dimensions of gallstones vary from 2 to 6 cm. Brogna B, et al. [12,13] found 13 previously published cases of biliary ilio (BI) with spontaneous resolution; in most cases, the patients were women. The time for spontaneous resolution varies from 16 hours to 7 days, and the impaction site was, in most cases, the right iliac fossa. In two cases, the gallstone in the rectosigmoid area was found. In three cases, gallstones were visualized on imaging, but in two cases, multiple gallstones were visualized on spontaneous evacuation. In one case, multiple gallstones were described on CT. The CT was the most widely used imaging tool to diagnose IB. In six cases were found Cholecystoduodenal adhesions fistulas were on CT. In one case, was found a cholecystocolonic fistula on CT and MRI. In one case, a cholecystoduodenal fistula. In this case, the suspected progression of the gallstones in the intestinal tract was followed by imaging and evacuated spontaneously in about seven days. Therefore, in elderly patients and comorbidities, initial conservative management could be considered, especially in the presence of high-risk factors for surgery. On the other hand, spontaneous fistula closure can occur in 50% of cases. However, in this case, there was a potential 5 to 33% risk of the repeated impact of more stones. In this case, the clinicians opted for conservative management due to the high risk of surgical complications from the patient's older age and comorbidities [12,13].
No funding was received.
Not applicable.
Ethics approval waived.
Consent to publish obtained.
The authors declare that they have no competing interests.