Adult intussusception is a rare condition, and idiopathic cases are even much more uncommon. We report a case of a 38-year-old female patient who presented with severe abdominal pain, vomiting, and a paraumblical palpable mass. Initial investigations revealed elevated white blood cell count, and low hemoglobin level. Computed tomography (CT) scan confirmed the presence of an intussuscepted jejunal loop with obstructive changes. Surgical exploration was performed, and a resection of the intussuscepted jejunal loop and an end-to-end anastomosis were carried out. Histopathological examination showed necrotic and ischemic changes without malignancy. The patient had a favourable postoperative recovery and was discharged in stable condition.
This case emphasizes the diagnostic challenges and surgical management considerations in adult intussusception, especially when the etiology is idiopathic. Clinical presentations are often nonspecific, and imaging, particularly CT scan, is crucial for accurate diagnosis. Individualized surgical approaches should be based on factors such as the location of intussusception and the presence of underlying pathology or malignancy.
Intussuscption, Idiopathic, Jejuno-jejunal
Intussusception in adults is a rare occurrence, typically associated with the presence of a pathological lead point. However, it is very uncommon for the etiology to be identified as idiopathic [1]. In this case study, we present a case of an adult female who experienced jejuno-jejunal intussusception without any identifiable organic cause. The patient presented with worsening abdominal pain and a paraumblical palpable mass.
A 38-year-old female patient was referred from a rural area hospital to our facility, she presented with severe abdominal pain and vomiting, that had worsened over the last two days. She had a long history of abdominal pain over the last two years and intermittent periods of constipation, additionally; she had experienced weight loss of approximately 14 kg over the same period. At the time of presentation, the patient appeared ill and was oriented. She had a nasogastric tube in place from the referred hospital, from which greenish-colored fluid was observed. Upon examination, the patient had a distended abdomen without tenderness or guarding, a palpable well-defined mass was identified in the abdomen around the umbilicus. The previous hospital examination had revealed massive rectal bleeding. Vital status at time of admission revealed that blood pressure of 114/69 mmHg, temperature of 36.7 °C, and oxygen saturation of 96%. Initial investigations showed that arterial blood gas analysis revealed a pH of 7.43, PCO 2 of 29.2 mmHg, and HCO 3 of 20.8 mEq/L. The white blood cell count was elevated at 25.77 × 10^9/L, and the hemoglobin level was markedly declined at 6.3 g/dL. Following resuscitation measures, the patient received transfusion of packed red blood cells after cross-matching and blood grouping.
A computed tomography (CT) scan with intravenous contrast was performed (Figure 1A and Figure 1B), which revealed long segment bowel-within-bowel appearance involving a jejunal loop, along with obstructive jejunal bowel changes and the presence of omental fat and mesenteric vessels within the intussuscepted bowel. The CT scan also showed mild to moderate free fluid and a filling defect thrombus in the distal portion of the superior mesenteric vein. No abnormalities were observed in the liver, portal vein, or biliary system.
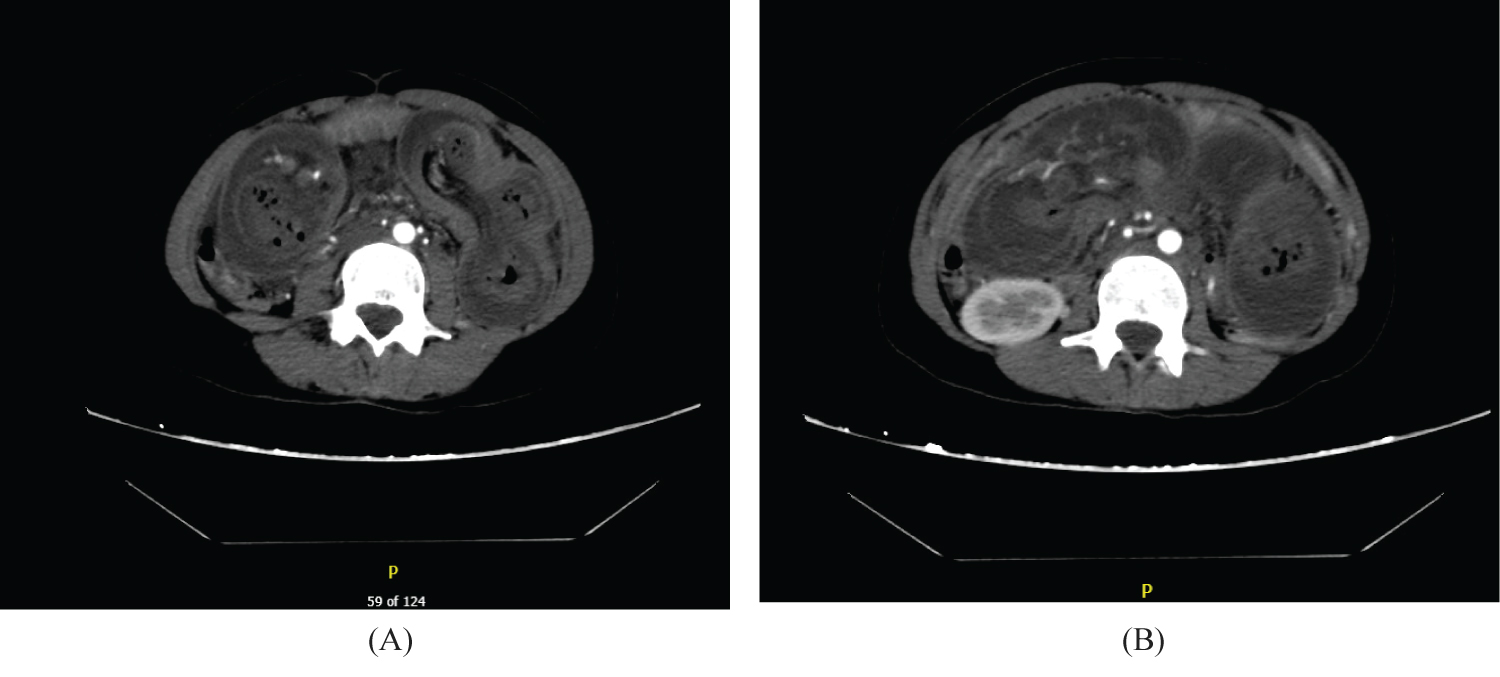 Figure 1: Axial CT scans of intussuscepted long segment of a jejuno-jejunal small intestinal loop.
View Figure 1
Figure 1: Axial CT scans of intussuscepted long segment of a jejuno-jejunal small intestinal loop.
View Figure 1
A consultation was conducted with the general surgery team regarding the CT findings. The plan included nothing per mouth (NPO) status, intravenous fluids, keeping the nasogastric tube inserted, urinary catheterization with output monitoring and ongoing blood transfusion. After admission, the initial output from the nasogastric tube was 700 mL of greenish fluid. The patient showed partial improvement and was scheduled for exploratory laparotomy after receiving the third unit of blood.
The surgical procedure, performed involved resection of the intussuscepted jejunal loop and end-to-end anastomosis. During the operation, a midline laparotomy was done, and the intussuscepted loop, located 5 cm from the duodenojejunal flexure, was identified. Resection of the involved jejunal loop (Figure 2 and Figure 3), approximately 2 meters in length, was carried out, along with an end-to-end anastomosis. A small perforation in the distal segment was repaired. After ensuring hemostasis and performing a saline wash, the abdominal wall was closed, and a drain was placed in the pelvis. The resected segment was sent for histopathological examination which showed extensive necrotic and ischemic changes in the small bowel, with marked neutrophilic infiltration, congestion, and edema. The surgical margins appeared normal, and no malignancy was detected.
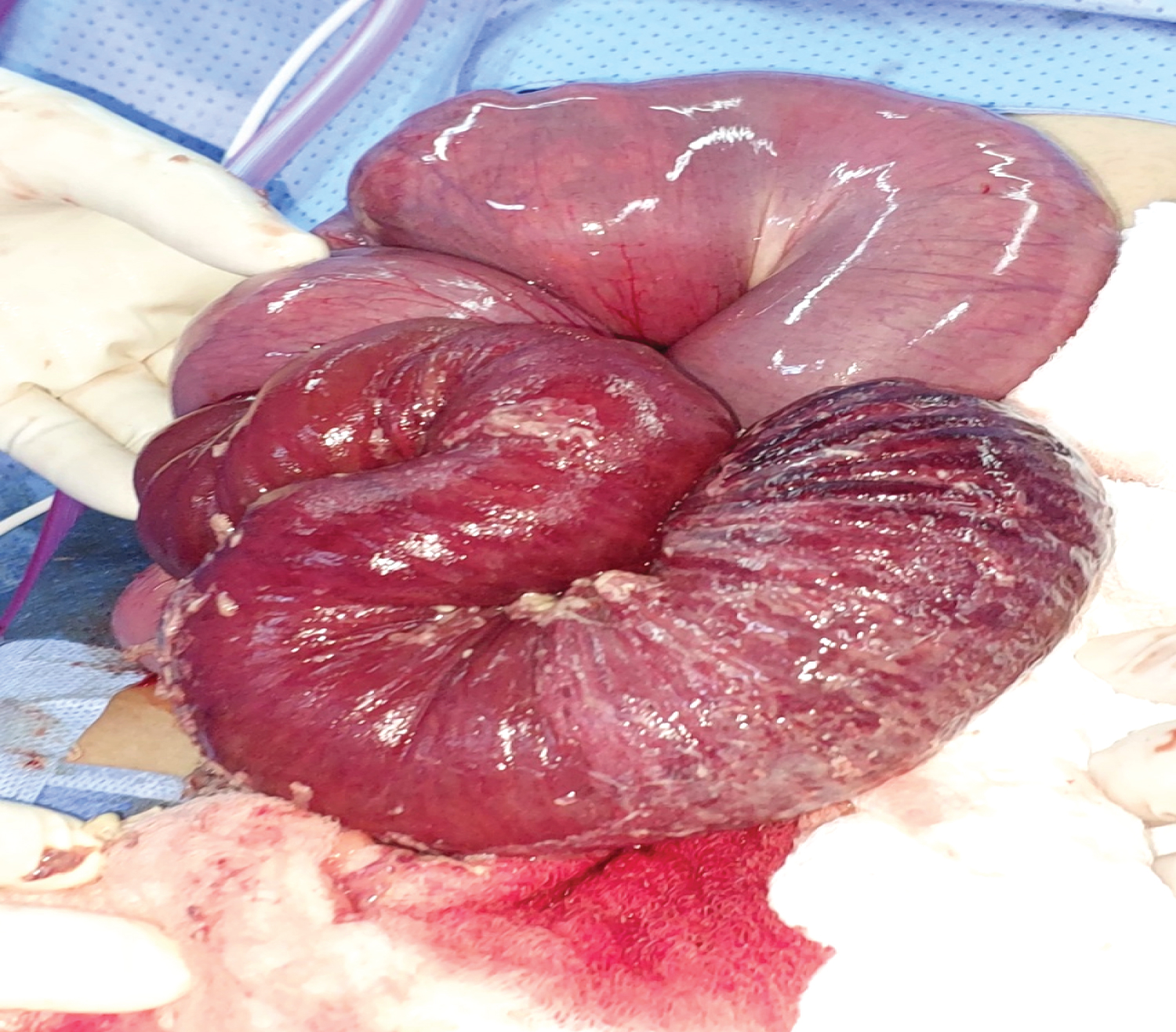 Figure 2: Visual inspection of the intussuscepted jejuno-jejunal loop revealed evident ischemic changes within the affected loop, while the surrounding jejunal loops appeared grossly normal.
View Figure 2
Figure 2: Visual inspection of the intussuscepted jejuno-jejunal loop revealed evident ischemic changes within the affected loop, while the surrounding jejunal loops appeared grossly normal.
View Figure 2
 Figure 3: Resected jujenal specimen shows ischemic changes.
View Figure 3
Figure 3: Resected jujenal specimen shows ischemic changes.
View Figure 3
Following the surgical procedure with no significant complications observed, the patient was transferred to an inpatient unit. Throughout the subsequent four days, her vital signs were consistently monitored and remained stable. She was kept on a nothing per mouth (NPO) status, received intravenous fluids, antibiotics, and human albumin. The output from her hemovac drain was diligently monitored and exhibited a gradual decrease until it ceased entirely.
Intussusception is defined as the protrusion of a proximal segment of the bowel into a distal segment. While intestinal intussusception is prevalent among children, it is infrequent in adults [1]. Many surgeons typically have limited exposure to adult cases throughout their career, as intussusception in this age group accounts for merely 5% of all intussusception cases and found to be a direct cause of intestinal obstructions in only 1-5% of adults [2]. The precise process of how this protrusion occurs in adults is uncertain, though it is thought that any intestinal wall or lumen lesion, known as lead point, that affects regular peristaltic action might cause this protrusion; hence the expansion of the protrusion to include larger segments of the intestine, mesentery and mesenteric blood arteries, this is promoted by more physiological peristalsis along the intestinal intussusceptions [3]. However, this hypothesis does not address how exactly intussusceptions in idiopathic instances develop same as in our case.
In adults, intussusception is often associated with an underlying aetiology in approximately 90-95% of cases, while in only 5-10 % the cause is set to be idiopathic [4]. Benign lesions, such as benign neoplasms, Meckel's diverticuli, appendix, and adhesions, are the primary lead points in the small intestine. Malignant lesions account for 25% of small bowel intussusceptions, while this percentage increases to around 50% in the large bowel [3]. A classification system has been developed based on the anatomical location of intussusceptions [5]. This classification categorizes intussusceptions into ileo-colic, ileo-ileo-colic, colo-colic, and small bowel intussusception involving the jejuno-jejunal and ileo-ileal regions [5].
Regarding the clinical presentation of intussusception in adults, while it is more apparent in pediatric cases, the literature describes it as primarily non-specific in adult patients, and its duration at time of presentation varies accordingly as it might appear as acute, intermittent, or chronic course [6]. Abdominal pain was identified as the predominant and most frequently observed presentation of intussusception in adults [7]. Less common presentations encompassed abdominal distension, palpable abdominal mass, nausea, vomiting, gastrointestinal hemorrhage, and alterations in stool patterns [7].
Imaging is the diagnostic modality of choice for identifying intussusception with high sensitivity; abdominal ultrasonography typically used for diagnosing intussusception in both pediatric and adult age groups [8,9]. It offers several advantages, including ease of execution and less invasiveness compared to alternative approaches. In the hands of a proficient radiologist, it enables a prompt and straightforward diagnosis, facilitating timely surgical intervention [8,9]. Noteworthy ultrasonographic indicators of intussusception encompass the distinctive 'target' and 'doughnut' signs observed in the transverse view, alongside the 'pseudo-kidney' sign evident in the longitudinal view [8]. A computed tomography (CT) examination commonly demonstrates a discernible three-layer structure consisting of the intestinal wall, its mesentery, and the enveloping intestine; also CT scans occasionally identify if there is a tumor serving as the provoking lead point [9]. Consequently, CT emerges as the foremost diagnostic modality for intussusception [10].
Considerable controversy surrounds the surgical management of adult intussusception, specifically pertaining to the optimal extent of surgical resection [5,7,11]. The debate focuses on whether en bloc resection without manipulating the mass or selective reduction prior to resection is more advantageous [7,11]. However, in cases of post-traumatic or postoperative intussusceptions, a simple reduction without resection is deemed acceptable [12]. Notably, in pediatric patients and instances where intussusception occurs in the small bowel, a simple reduction may be theoretically permissible if the affected bowel appears viable and lacks evidence of neoplastic lesions [12]. Conversely, operative reduction should be avoided when the bowel exhibits signs of inflammation or ischemia. In the case of colo-colic intussusception, en bloc resection without reduction is recommended due to the higher likelihood of underlying malignancy [5,7,11,12]. In our case, the initial preoperative CT scan revealed an intussuscepted jejunal loop (jejuno-jejunal) associated with obstructive jejunal bowel changes without any apparent evidence of a lead point. Intraoperatively, the same findings were observed as depicted in the CT scan. Consequently, the selected procedure involved resecting the intussuscepted jejunal loop, which measured 2 meters in length, followed by performing an end-to-end anastomosis. Considering the location of the intussusception, the lower incidence of malignancy in this area and the absence of any indicators of the presence of a lead point in both the CT and intraoperative examinations, the etiology was deemed idiopathic. Therefore, the advisable procedure was to proceed with the resection and anastomosis technique.
We have not any financial and personal relationships with other people or organizations that could inappropriately influence our work.