Background: Necrotizing fasciitis (NF) is a rare life-threatening soft tissue infection. The development of NF of the lower extremity secondary to a perforated colorectal tumor has been reported only in a few cases.
Case report: We report a case of 65-year-old female with abdominal and thigh pain was diagnosed with NF based on clinical and radiological findings. Urgent surgical debridement and exploratory laparotomy revealed a perforated colon cancer mass with retroperitoneal abscess. The patient underwent left hemicolectomy, subsequent debridements, followed by left lower limb disarticulation. Histopathological examination confirmed adenocarcinoma.
Conclusion: Early diagnosis and aggressive surgical intervention are crucial in NF management. Awareness of the development of NF secondary to perforated colon cancer is essential to prompt diagnosis and to prevent delays in proper management.
Necrotizing fasciitis, Cancer colon, Lower extremity
Necrotizing fasciitis (NF) is an uncommon yet life-threatening soft-tissue infection characterized by rapid progression and necrosis of the muscle, fascia, and subcutaneous tissue [1]. Early diagnosis and aggressive surgical intervention are crucial to mitigate the high mortality rates associated with this condition [1,2]. While NF is commonly caused by trauma or surgical wounds, it can also arise secondary to various underlying conditions, such as intra-abdominal infections, inflammatory bowel diseases perforated or penetrated diverticulitis [3].
The occurrence of necrotizing fasciitis (NF) associated with cancer colon is infrequently documented in the literature. In this report, we present a unique and rare case of NF affecting the iliopsoas and thigh muscles, which developed as a consequence of a recently diagnosed perforated left sided colon cancer.
A 65-year-old Sudanese female with a past medical history of diabetes mellitus and hypertension presented to the emergency room with complaints of left upper abdominal pain for 2 weeks and left thigh pain and swelling for one week. On examination, she was elder woman, obese and in discomfort. Vital signs were notable for a heart rate of 117 beats per minute, blood pressure of 153/67 mmHg, temperature of 36.6 °C, and oxygen saturation of 97% on room air. Abdominal examination revealed tenderness in the left upper quadrant without signs of peritonitis. Examination of the left leg demonstrated tenseness and tenderness without swelling or redness.
Initial labs showed elevated white blood cell count of 24.69 × 109/L, elevated creatine kinase (899 U/L), alkaline phosphatase (365 IU/L) and lactic acid levels (7.9 mmol/L). The tumor marker profile exhibited a notable increase in Carcino Embryonic Antigen (CEA) levels (24.15 ng/ml), while other markers, including CA 19-9 and CA 125, were found to be negative. Computed tomography (CT) of the abdomen, pelvis and upper lower limb showed focal mural thickening and irregularity of the descending colon with surrounding multiloculated intra and retro peritoneal collection, with down word extension of fluid and air to the left iliac fossa. Also the CT showed diffuse air foci at left thigh in the facial plane which extend to left psoas and iliacus muscle. Those findings are suggestive of a ruptured tumor or inflammatory process with extension of fluid and air into the left lower quadrant and left thigh consistent with necrotizing fasciitis (Figure 1).
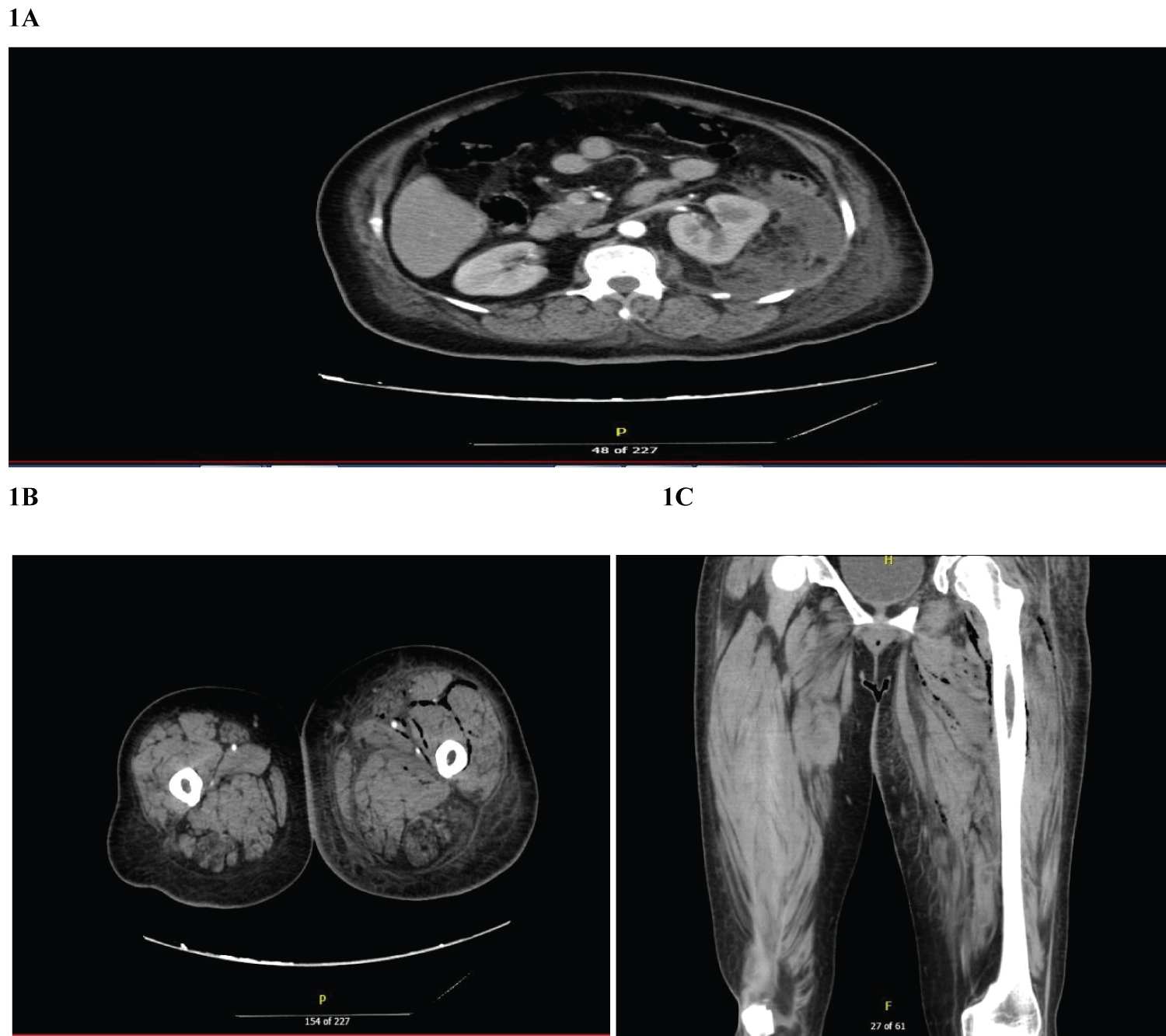 Figure 1: (A) Axial Computed tomography (CT) image demonstrated a thickened mural wall of the descending colon and abscess formation around this area; (B,C) Axial and coronal CT image showed a diffuse air foci at left thigh in the facial plane which extend to left psoas and iliacus muscle.
View Figure 1
Figure 1: (A) Axial Computed tomography (CT) image demonstrated a thickened mural wall of the descending colon and abscess formation around this area; (B,C) Axial and coronal CT image showed a diffuse air foci at left thigh in the facial plane which extend to left psoas and iliacus muscle.
View Figure 1
She was admitted to the intensive care unit for management of necrotizing fasciitis with septic shock and immediately transferred for an urgent debridement of the left thigh with copious wound irrigation and placement of serial wound dressings (Figure 2). Post-operatively, her clinical status deteriorated with progressive renal failure and requirement for hemodynamic support. Intra-abdominal cultures grew [organism], sensitive to Meropenem, which was started already since admission.
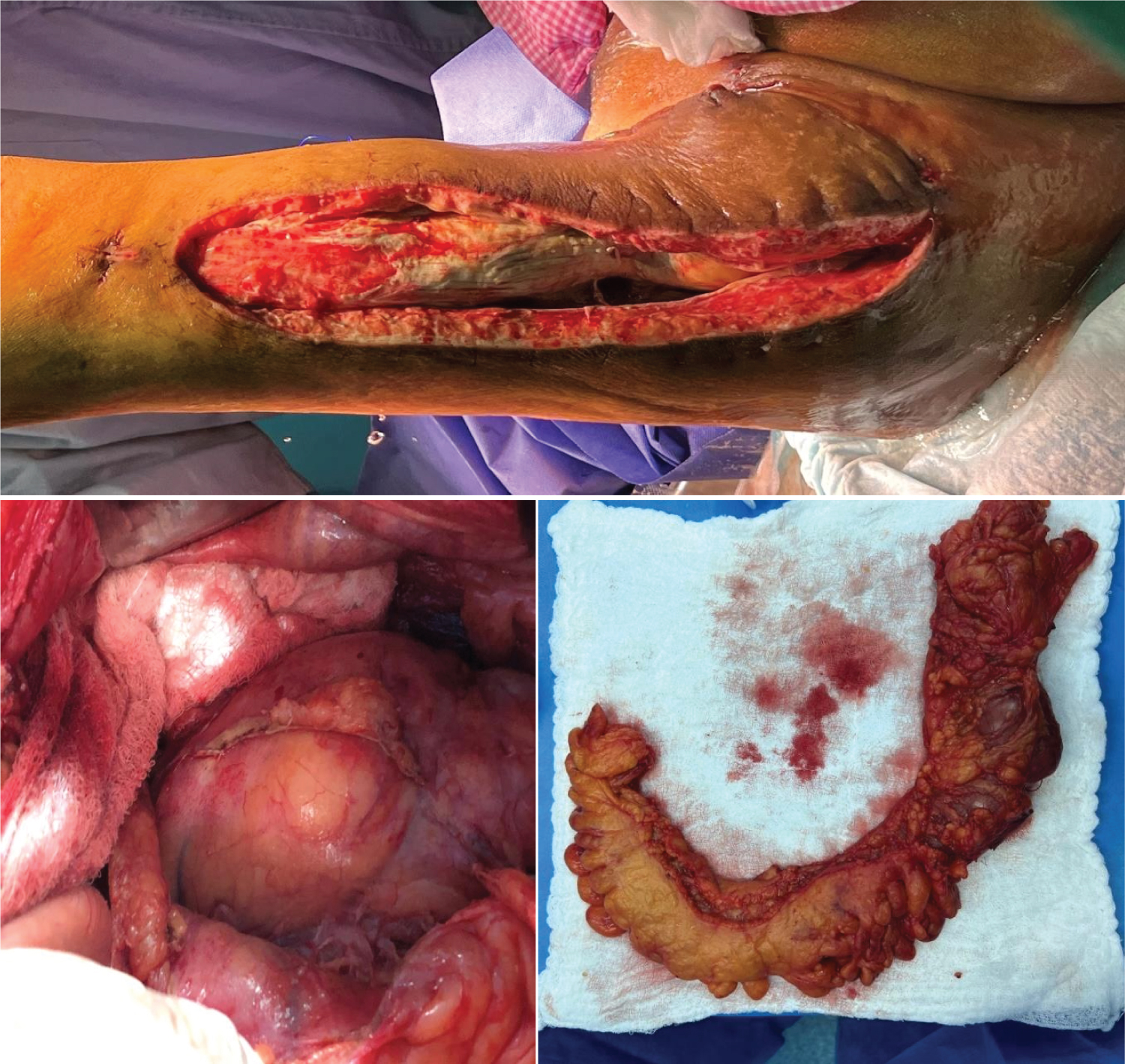 Figure 2: (A) Additional extensive open wound for drainage from the initial drainage site of the left thigh; (B) Intraabdominal image demonstrating the left colon; (C) Surgical specimen of the left hemicolectomy.
View Figure 2
Figure 2: (A) Additional extensive open wound for drainage from the initial drainage site of the left thigh; (B) Intraabdominal image demonstrating the left colon; (C) Surgical specimen of the left hemicolectomy.
View Figure 2
She subsequently underwent an exploratory laparotomy in which we found an obstructing mass adherent to the splenic flexure of the colon with extension into the retroperitoneum associated with retropretonial abscess and necrotic tissue formation (Figure 2). A left hemicolectomy was performed with drainage of 200 millimetres puss from the large retroperitoneal abscess. End colostomy was created at the left side. Post-operatively she required continued critical care support and monitoring to compensate the systematic septic status. The colonic mass was sent as a biopsy for histopathological examination and revealed a moderately differentiated adenocarcinoma and her postoperative tumor marker profile follow up yielded negative results. She had a prolonged and complicated postoperative course requiring multiple subsequent debridements of her left thigh wound, finally a left lower limb disarticulation from hip joint and closure done via posterior flap was made. Her respiratory status declined briefly requiring intubation but ultimately improved. Her renal function recovered with supportive care. Oncological evaluation found stage III colorectal adenocarcinoma. After decannulation and gradual improvement, she was deemed stable for transfer to a higher center for adjuvant management.
The presented case highlights an exceptionally uncommon occurrence of perforation in the left colon due to colorectal cancer, as colonic perforation is a rare complication in this context [4], with the presentation by a reteroperitonial perforation that develops to a necrotizing fasciitis (NF) of the thigh muscles is even much more uncommon [5-7].
Necrotizing fasciitis (NF) is a severe suppurative infection affecting the soft tissues, leading to secondary necrosis of the subcutaneous tissues. While it can manifest in various anatomical sites, the abdominal wall, extremities, and perineum are frequently affected areas [1]. The incidence of necrotizing fasciitis (NF) in the United States alone is approximately 0.4 cases per 100,000 individuals annually [8]. Despite receiving appropriate management, the mortality rate remains high, ranging from 25% to 75% [2], and it is more likely to affect patients with immunocompromised status [9]. It typically manifests as a polymicrobial infection, with prevalent microorganisms comprising a mix of gram-positive cocci (such as Group A beta-hemolytic Streptococcus species), gram-negative rods, and anaerobes (such as Clostridium species). A significant proportion of these organisms are gas-forming which explains clinical surgical emphysema [10].
Early diagnosis and prober management is vital in the prognosis of necrotizing fasciitis. The diagnosis is suspected over a number of clinical manifestations, which encompass fever with associated rigors, localized tenderness, dermal discoloration, and palpable crepitus [1]. In cases of perforated colorectal cancer complicated by necrotizing fasciitis of the thigh and abdominal wall, as exemplified in the presented case, the affected individuals may initially manifest subtle and concealed clinical signs of a perforation. This can potentially result in delayed identification of an intraabdominal infection and NF [10].
Imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI) play a crucial role in discriminating necrotizing fasciitis (NF) from other superficial infections. The key imaging characteristics include fascial thickening exceeding 3 mm, fat infiltration, focal fluid collection, soft-tissue gas and up to intramuscular involvement [11,12]. However, these findings lack specificity as they can also be observed in non-necrotizing fasciitis and non-inflammatory conditions [12]. Therefore, a comprehensive assessment combining clinical and radiological features is essential for an accurate diagnosis.
The recommended approach for managing necrotizing fasciitis (NF) caused by colorectal cancer involves prompt early surgical intervention and intensive management for sepsis [6,7]. Emergent surgical debridement and open drainage of the affected tissues is the highest priority and the primary modality for managing NF [6,7,9]. Ishibashi, et al. have demonstrated that a time interval of less than 12 hours between diagnosis and surgery significantly improves survival rates [13]. Following the initial surgical debridement, a series of subsequent debridements should be performed to achieve thorough complete removal of necrotic tissue. In instances where there is a substantial tissue defect in the lower limb, the possibility of limb disarticulation and tissue flap reconstruction should be considered [14], as demonstrated in our case. The adoption of colostomy as a step with in the therapeutic approach remains a subject of debate, in cases of Fournier gangrene where the infection is localized near the primary tumor site, the implementation of a colostomy is considered essential to prevent contamination [7]. However, in instances where necrotizing fasciitis manifests at a distant location from the primary tumor, Sato, et al. concluded that the requirement for colostomy may be less pronounced, the decision was to proceed with colostomy in our specific case [7]. To optimize the oncological outcome, once the NF is under control, timely implementation of oncological interventions, including surgical resection and chemotherapy, is necessary [5].
Necrotizing fasciitis of the thigh may occur after an unanticipated retroperitoneal abscess, and necrotizing fasciitis should be taken into account when diagnosing colon cancer. The mortality rate related to necrotizing fasciitis can be decreased with early diagnosis and treatment.