We present the case of a 48-year-old female with a history of symptoms including exertional dyspnea, fatigue, chest pain, and cough with clear sputum for three months. She had a previous history of a car accident two years prior. Upon evaluation, vital signs and physical examination findings were normal. Imaging revealed a giant diaphragmatic hernia with intestinal loops and a transverse colon hernia in both lung fields, displacing the heart to the left. Surgical repair was performed, revealing a large diaphragmatic defect with herniated abdominal organs. The patient recovered well postoperatively with resolution of symptoms and was discharged after eight days with rehabilitation therapy. The case underscores the importance of considering late-onset diaphragmatic hernias in patients with a history of trauma and nonspecific symptoms, emphasizing the need for early identification and intervention to improve outcomes and reduce the risk of recurrence.
Giant diaphragmatic hernia, Diaphragmatic plasty, Abdominal trauma
The diaphragm is a muscular and tendinous dome-shaped partition originating from the sternum, ribs, twelfth thoracic vertebra, and the first, second, and third lumbar vertebrae. It is the most important inspiratory muscle and, unlike skeletal muscles, is constantly active. The inferior surface of the diaphragm covers the liver, the intra-abdominal portion of the esophagus, the stomach, the spleen, the adrenal glands, and the kidneys and, to some extent, the pancreas and the transverse colon. This muscle has four serous membranes: Three covering its upper or thoracic surface, and one covering its abdominal surface. The three serous membranes of its upper surface are the pleura on each side and the serous layer of the pericardium, covering the middle portion of the central tendon. The serous membrane covering the abdominal surface is a section of the general peritoneal membrane of the abdominal cavity.
A diaphragmatic hernia is defined as the passage of abdominal contents into the thoracic cavity through a defect in the diaphragm. Diaphragmatic rupture is an important indicator of the severity of trauma. Traumatic diaphragmatic hernias are very uncommon. Events triggering these injuries usually involve a sudden increase in abdominal pressure. The severity of symptoms varies depending on the degree of abdominal protrusion into the pulmonary space.
We present a 48-year-old female patient who suffered from exertional dyspnea, fatigue, asthenia, adynamia, chest pain, and cough with hyaline sputum for three months. She had a history of a car accident two years ago.
She was referred to our unit and evaluated. She presented with vital signs within normal parameters and no compromise of neurological status, adequate skin and mucous membrane coloration. On thoracic examination, rhythmic heart sounds, right lung base peristaltic sounds. Abdomen was globular due to abundant adipose tissue. No other alterations were noted.
Laboratory tests were within normal ranges. Chest X-ray showed characteristic radiolucency of intestine in the right hemithorax, with displacement of thoracic structures to the contralateral side (Figure 1 and Figure 2). It was decided to perform a thoraco-abdominal computed tomography which showed a giant diaphragmatic hernia of 8.8 cm with mesenteric fat, intestinal loops, transverse colon spanning both lung fields, and displacing the heart posteriorly to the left (Figure 3 and Figure 4).
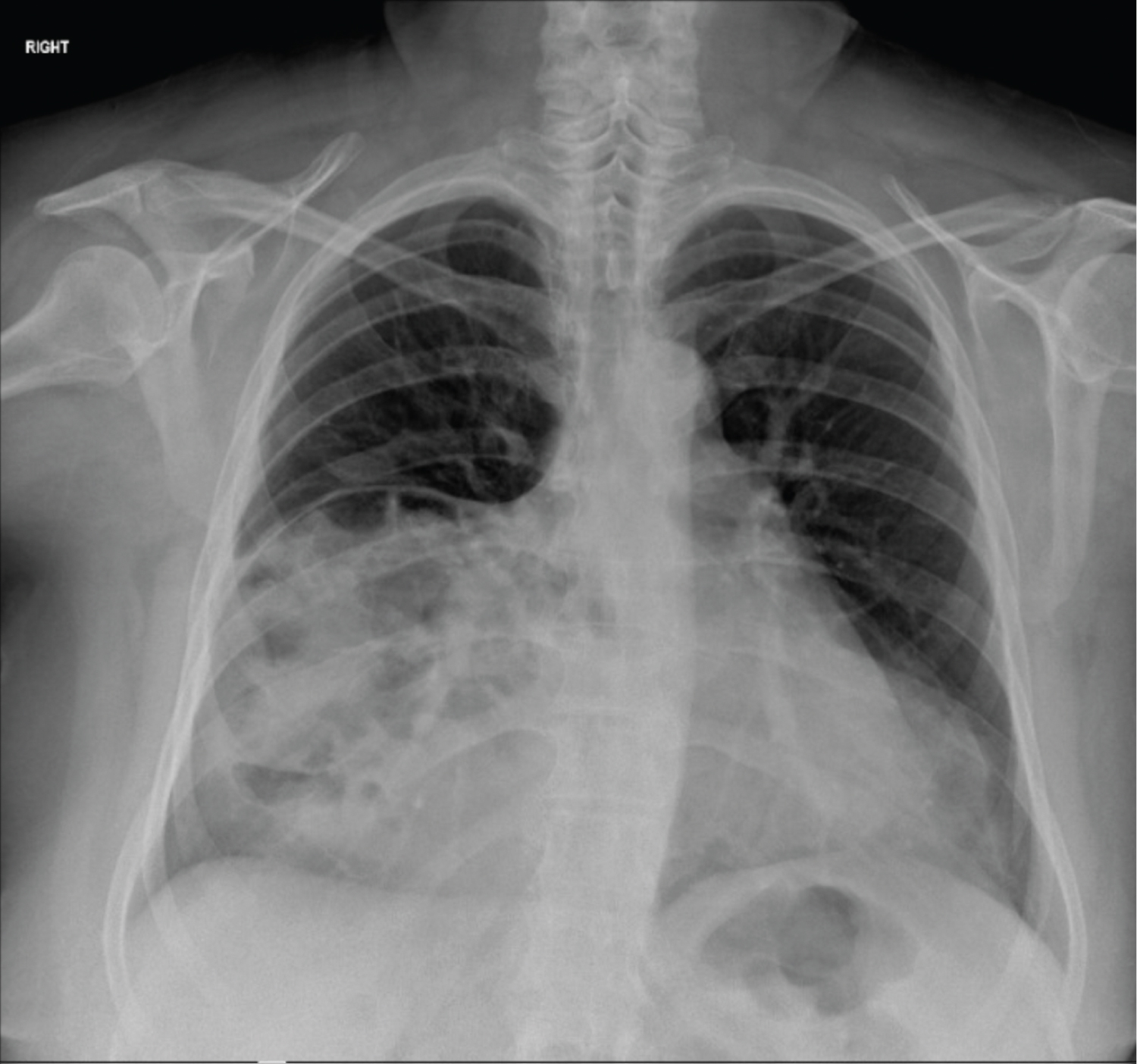 Figure 1: Chest X-ray before hernia repair.
View Figure 1
Figure 1: Chest X-ray before hernia repair.
View Figure 1
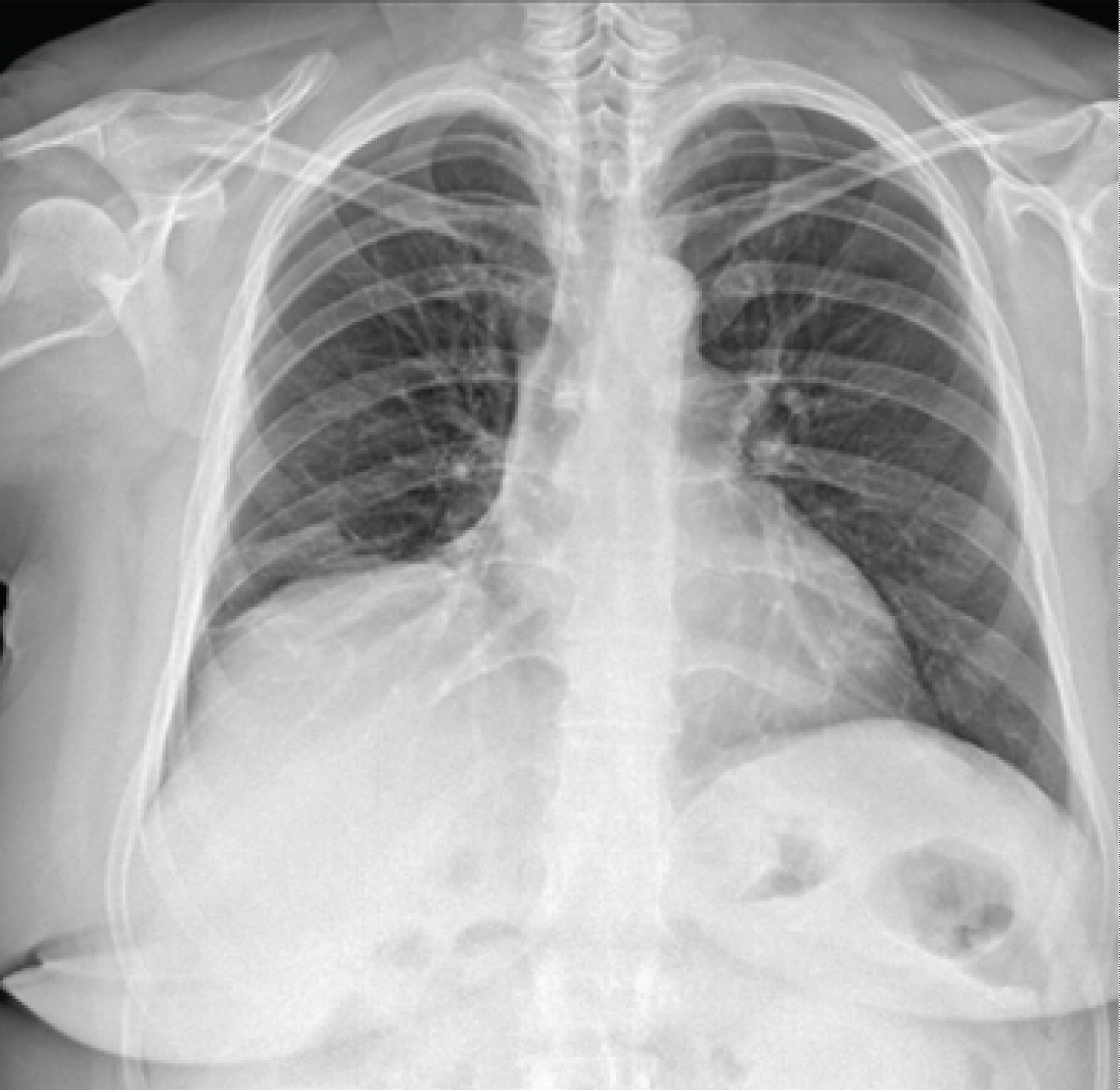 Figure 2: Chest X-ray after hernia repair.
View Figure 2
Figure 2: Chest X-ray after hernia repair.
View Figure 2
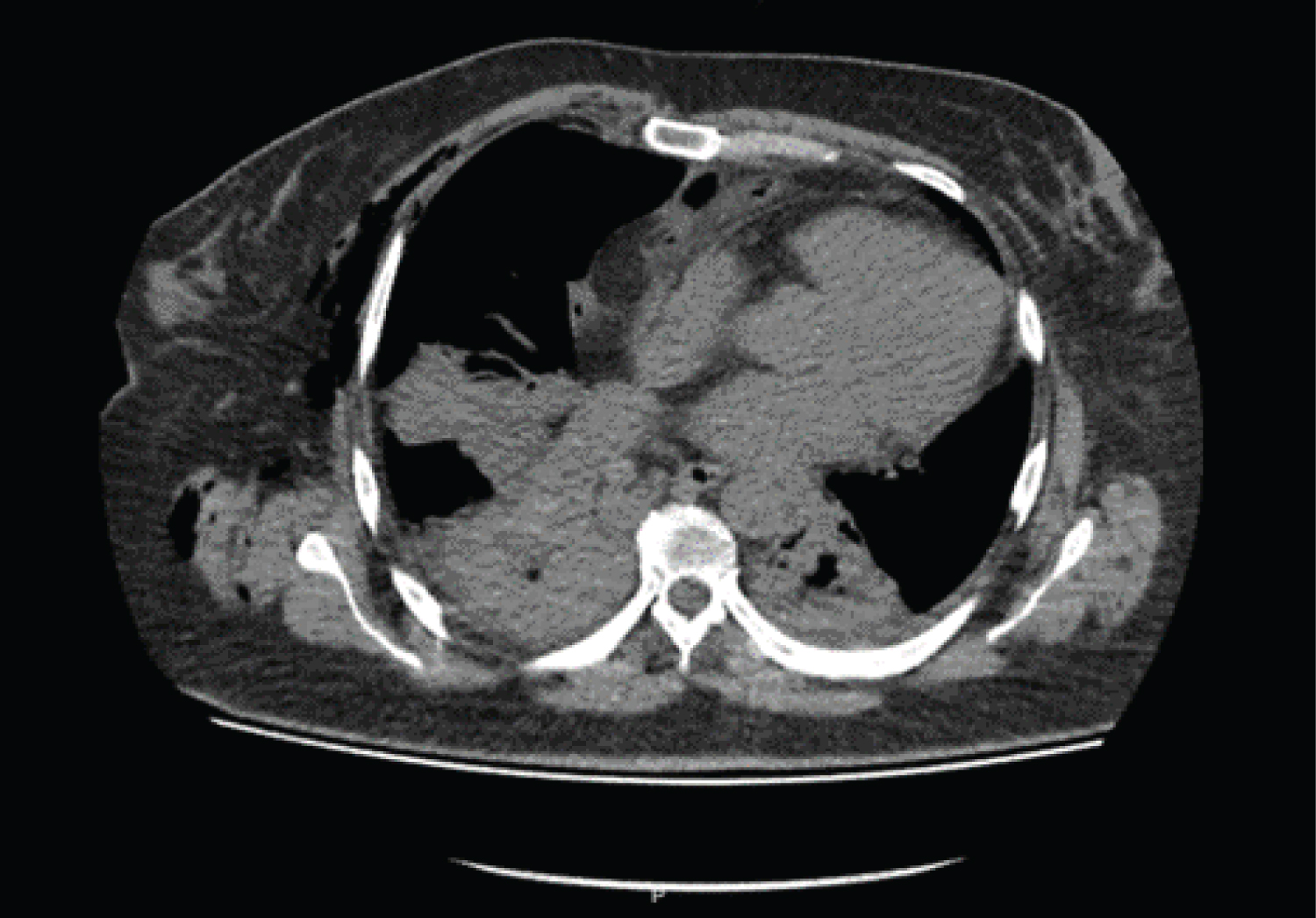 Figure 3: Simple tomography, transverse section at the level of the mediastinum, occupation of abdominal organs is observed in the right hemidiaphragm.
View Figure 3
Figure 3: Simple tomography, transverse section at the level of the mediastinum, occupation of abdominal organs is observed in the right hemidiaphragm.
View Figure 3
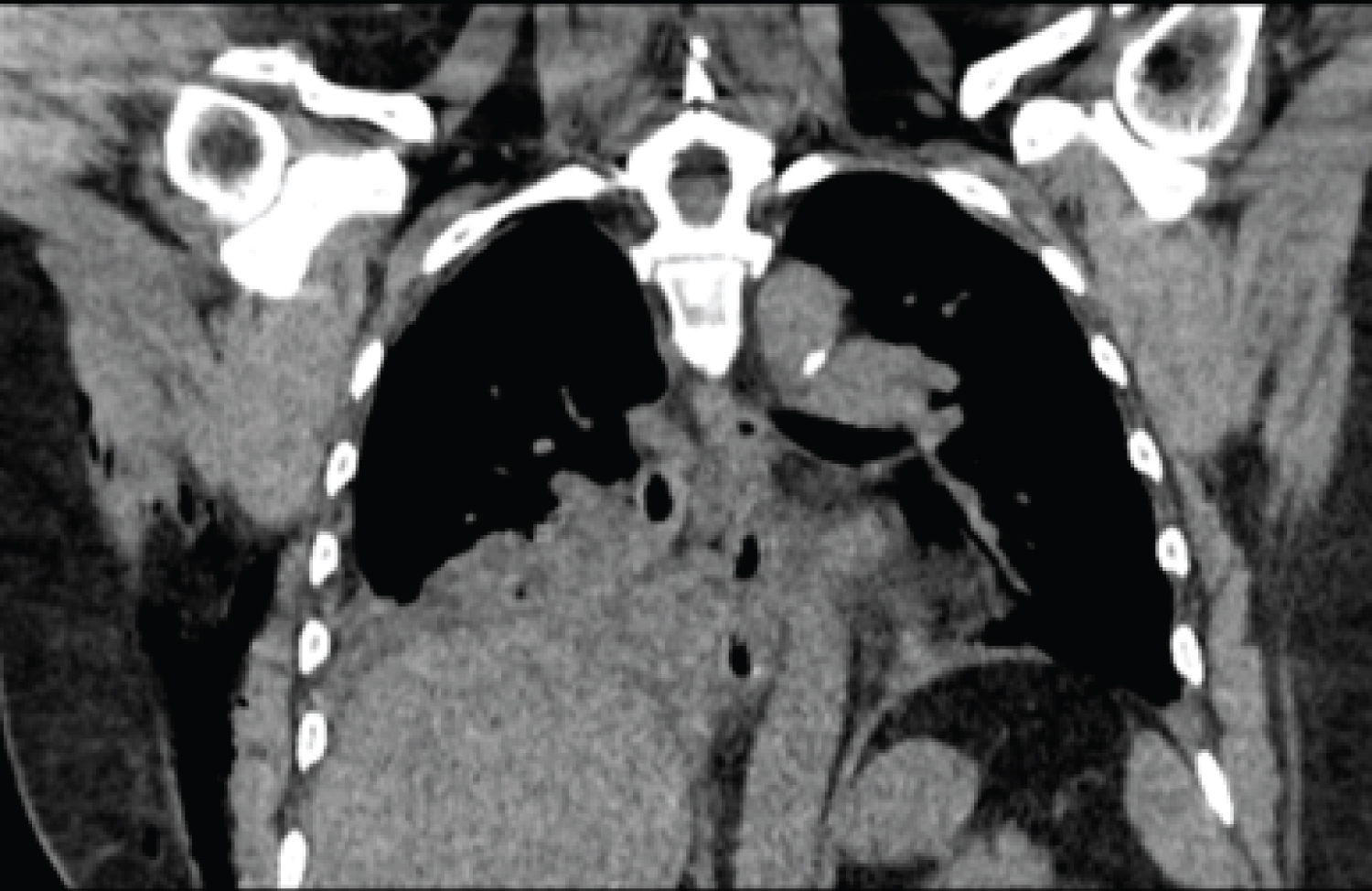 Figure 4: Coronal reconstruction showing rise of intestinal contents in the right hemidiaphragm, which causes partial pulmonary collapse.
View Figure 4
Figure 4: Coronal reconstruction showing rise of intestinal contents in the right hemidiaphragm, which causes partial pulmonary collapse.
View Figure 4
Surgical repair was decided due to clinical deterioration and patient's desire. Exploratory laparotomy was performed, revealing an anterior right diaphragmatic defect of 10 × 9 cm, loops of small intestine, omentum, mesentery, and transverse colon in the right hemithorax, with collapsed right lung which recovered after Valsalva maneuver (Figure 5). Diaphragmatic plasty with mesh was performed and fixed with separate polypropylene sutures on the abdominal side of the diaphragm (Figure 6).
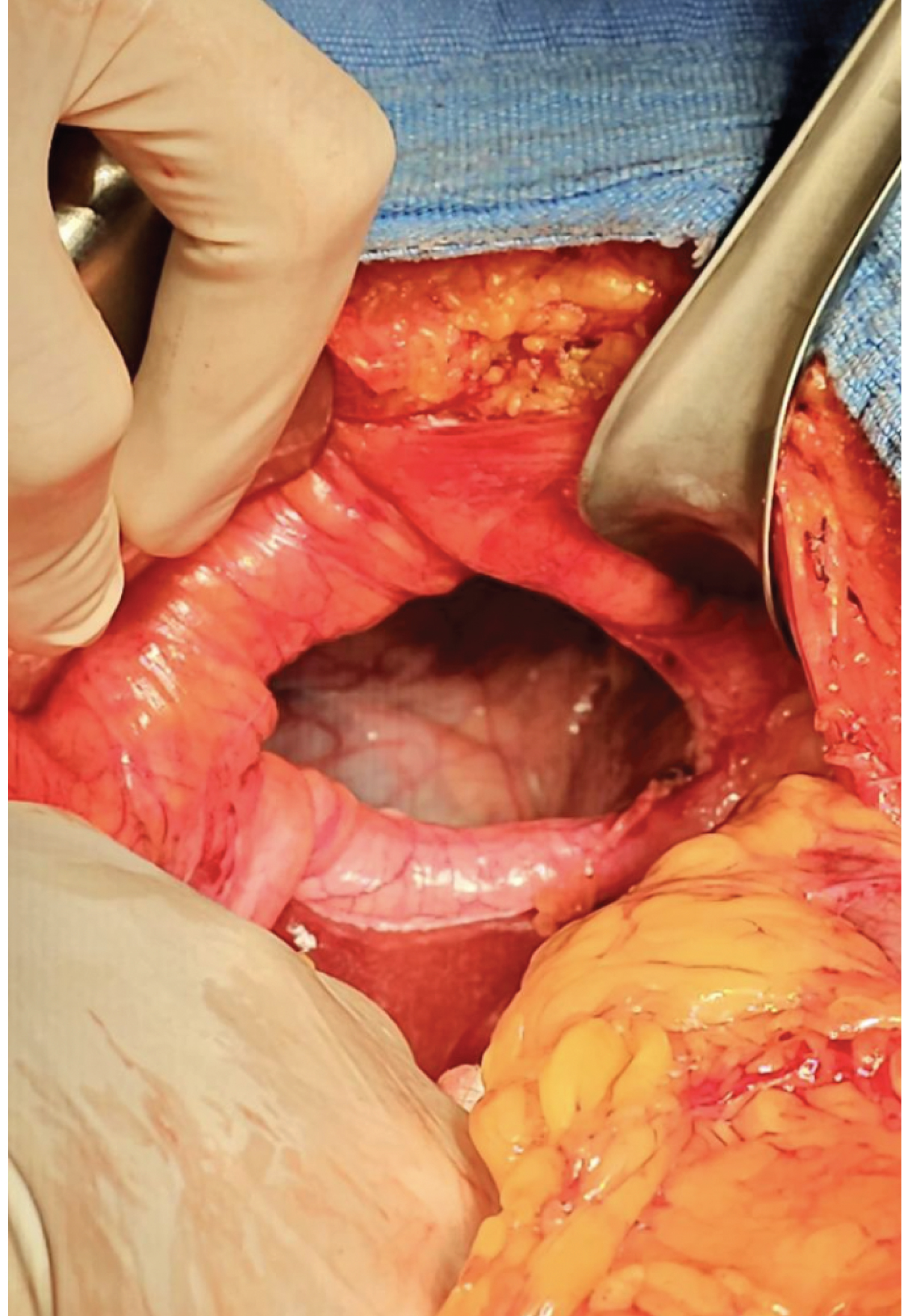 Figure 5: Image showing hernial ring.
View Figure 5
Figure 5: Image showing hernial ring.
View Figure 5
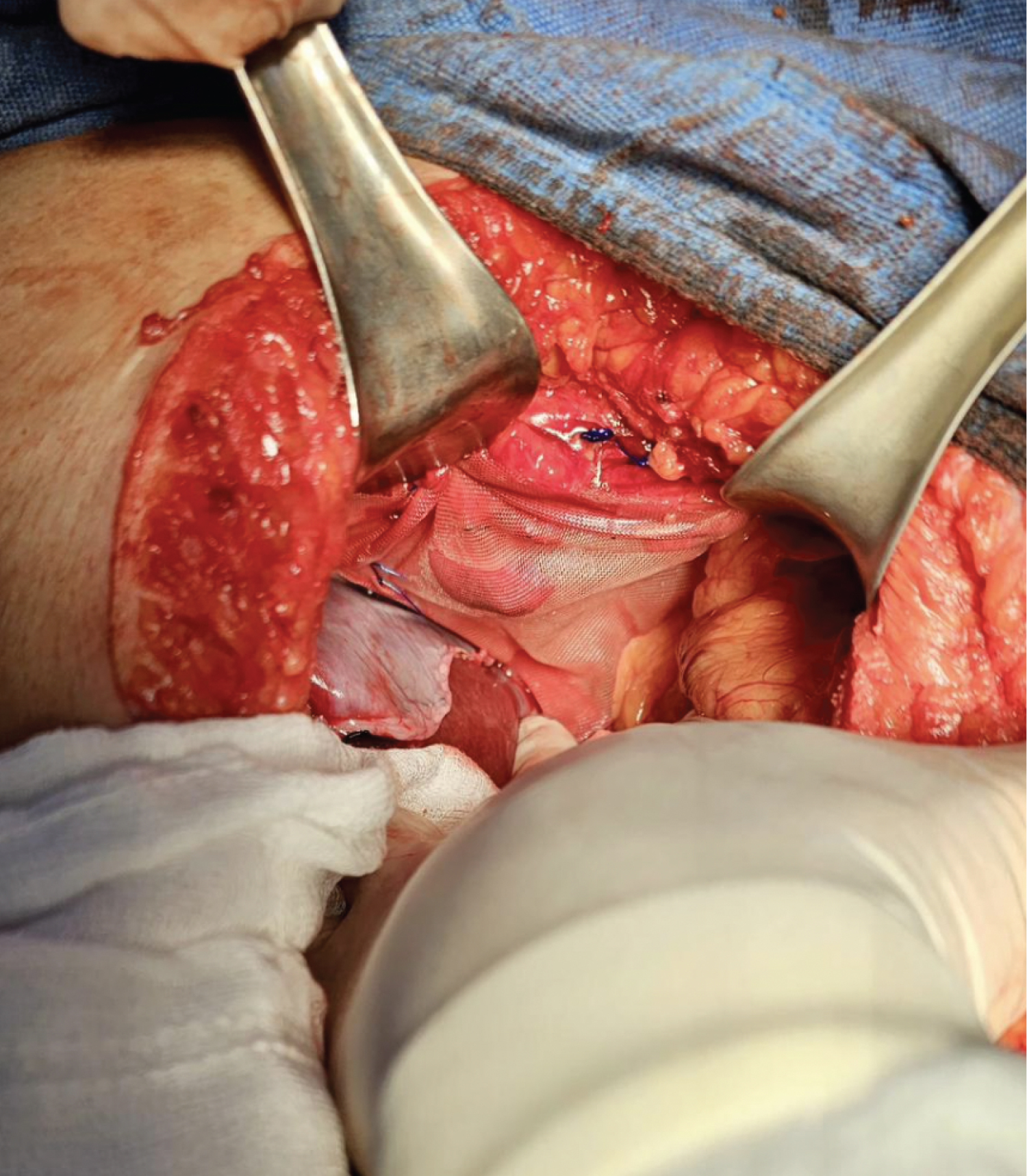 Figure 6: Image showing repaired herniated defect.
View Figure 6
Figure 6: Image showing repaired herniated defect.
View Figure 6
The patient had a favorable postoperative course, with notable clinical improvement, resolution of exertional dyspnea and adynamia, and improvement of cough. She was discharged after eight days with pulmonary and cardiac rehabilitation therapy [1-4].
Diaphragmatic hernias can arise from closed injuries, such as traffic accidents, which account for approximately 75% of cases, or penetrating injuries, such as stab or gunshot wounds, which represent the remaining 25% [5]. In cases of closed traumas, sudden changes in intra-abdominal pressure can cause significant tears in the diaphragm, requiring considerable impact to provoke such an injury. The severity of the injury and the subsequent surgical challenges for treating the diaphragmatic injury dramatically increase depending on associated intra-abdominal injuries [6], especially those associated with closed traumas that often pose a life-threatening risk to the patient. Penetrating injuries tend to cause only minor lacerations. In comparison, closed traumas are more likely to result in herniation of abdominal contents into the thorax because the defect is usually more extensive. The right hemidiaphragm has some partial protection provided by the liver in closed trauma. As a result, in a series of cases, approximately 68% of diaphragmatic injuries secondary to closed traumas affected the left side, 24% the right side, 1.5% both sides, 1% were pericardial, and 5% could not be classified [5].
The incidence of post-traumatic diaphragmatic hernias is still not precisely known. However, diaphragmatic injuries affect approximately 5% of patients with multiple traumatic injuries who have undergone laparotomy and were found in approximately 1% of patients in a wide trauma database [7,8].
Diaphragmatic hernias occurring after trauma can cause both respiratory and abdominal symptoms. Diaphragm rupture often goes unnoticed due to other serious injuries that may occur in the context of severe trauma [9]. Diaphragmatic injuries may not result in immediate herniation, but over time, normal negative intrathoracic pressure can cause a gradual increase in the size of a small diaphragmatic defect and, as a result, protrusion of abdominal contents through it. This phenomenon explains the delay in diagnosis, which occurs in approximately 15% of cases [10]. A variety of organs may be involved, including the stomach, omentum, colon, small intestine, spleen, liver, and even the kidney. The stomach, colon, small intestine, spleen, and omentum are more commonly found in left-sided hernias. The liver and colon are more common on the right side [11].
Diagnosis can be established in one of three distinct phases: The acute phase, which manifests immediately after trauma; the interval or latency phase, occurring between trauma and the presentation of complications, characterized by transient and occasional symptoms due to herniation of abdominal organs and spontaneous reduction of viscera; and the complication phase, when the hernia is complicated by obstruction or strangulation of organs contained within the hernial sac [12]. In cases of penetrating injuries affecting the area between the fourth intercostal space and the umbilicus, a high level of suspicion for possible diaphragmatic injury should be maintained. The onset of respiratory or abdominal symptoms several days or weeks after the injury may indicate an undiagnosed diaphragmatic injury.
Chronic post-traumatic diaphragmatic hernias are distinguished by the lack of peritoneal lining or a hernial sac. This characteristic is mainly related to extensive adhesions to the surrounding lung, reduction of which can cause significant bleeding. In these cases, repair is preferably done through a thoracic approach or by a combined thoracoscopic-abdominal approach, although cases of laparoscopic or thoracoscopic repair have also been described [13]. The combined approach reduces the risk of lung injury in case of adhesions and the absence of a peritoneal hernial sac complicating the abdominal approach. In our patient, contrary to what is generally observed, the hernia originated from the right side. She had a delayed presentation of diaphragmatic hernia, and the diagnosis was established during the interval phase, prior to severe complications. The latency period extended for 2 years; during this stage, patients often experience nonspecific symptoms, such as mild abdominal discomfort and occasionally respiratory symptoms.
In closed traumas, the left thoracoabdominal region is affected three times more than the opposite side. This is primarily attributed to the protective role of the liver, which cushions the sudden increase in the right hemidiaphragm [14-16]. The left hemidiaphragm has weak points related to the fusion sites of embryological outlines [17,18], and ultimately, the right hemidiaphragm is considered to have greater resistance to tension compared to the left side [15,17].
Although chest X-rays or computed tomography (CT) scans can be useful, their diagnostic capacity varies between 40% and 80% depending on the type of test performed [19]. Images are obtained through CT scans of the chest and abdomen, with reported sensitivities of 78% for left-sided hernias and 50% for right-sided hernias [20]. Various studies have shown that CT scans have a sensitivity and specificity ranging from 61% to 87% and 72% to 100%, respectively, for diagnosing diaphragmatic rupture [10,21]. After closed trauma, CT scans may reveal three characteristic changes:
1. The "collar sign" (also known as the hourglass sign) consists of a waist-like constriction of herniated viscera at the edges of the defect.
2. The "dependent viscera sign" is observed when the upper third of the liver is adjacent to the posterior ribs, either on the right or left, indicating that the stomach or intestine is in contact with the posterior ribs. This finding is uncommon as an intact diaphragm maintains a significant costophrenic angle posteriorly.
3. The "discontinuity of the diaphragm sign" occurs if a direct discontinuity in the diaphragm is observed along with a lack of visualization of a segment of it. In penetrating diaphragmatic traumas, the diagnosis can be made by following the trajectory of the weapon and looking for contiguous injuries in structures on both sides of the diaphragm, such as a liver injury on the right side or a splenic or gastric injury on the left side, commonly associated with hemothorax or pulmonary injuries [21,22]. Findings on CT scans that are evident after closed trauma are often not observed after penetrating injuries. The "dependent viscera sign" is rare in patients with penetrating injuries, which is attributed to the small size and variable location of the defect. Similarly, the "collar sign," which is related to the presence of intrathoracic hernia, is generally not present in penetrating traumas. Thickening of the diaphragm is a nonspecific sign but should raise suspicion of diaphragmatic injury, even if it is the only anomaly present.
In polytraumatized patients receiving ventilatory support, positive intrathoracic pressure may prevent herniation through a diaphragmatic rupture. However, upon discontinuation of mechanical ventilation, herniation may occur, potentially affecting breathing. Symptoms can arise long after the injury, and they have even been observed after a period of more than 10 years [10]. In such situations, the patient may not link the acute illness to a previous trauma. The attending physician should consider a traumatic cause when the defect in the diaphragm is not hiatal and is not found in typical locations of congenital defects. Surgical repair is necessary once a diaphragmatic rupture has been identified [23,24]. In most cases, repair in acute situations is performed through an abdominal approach.
The surgical approach to diaphragmatic injuries is based on the timing of diagnosis (early or late) and its clinical presentation. Patients with a missed diagnosis of diaphragmatic injury are likely to experience a prolonged clinical course (from months to years), characterized by a gradual increase in visceral herniation and the appearance of symptoms and signs of cardiorespiratory compromise, obstruction, and occasionally, strangulation with perforation of the herniated segment of the gastrointestinal tract into the affected hemithorax. The diaphragm, as a muscle, tends to retract rapidly and undergoes significant atrophy over time. Therefore, although primary repair of a diaphragmatic injury, by approximating the edges of the defect, may be feasible on the day of trauma, repairing an undiagnosed diaphragmatic injury is much more difficult due to the presence of herniated viscera, as well as retraction and atrophy resulting from delayed diagnosis. Since the characteristics of the diaphragm change over time in patients with undiagnosed diaphragmatic injuries, primary repair is associated with a high rate of suture line failure; therefore, alternative techniques for repairing chronic diaphragmatic hernias, such as the use of prosthetic material to correct the defect, are preferable.
The use of prosthetic materials is recommended in defects of considerable size, usually exceeding 20 to 30 cm. However, it is crucial to evaluate the anatomy of the defect, especially in chronic cases, where retracted edges are unlikely to be primarily sutured, even in smaller defects [25].
In this particular case, repair was performed through an abdominal incision, carrying out correction of the defect by herniorrhaphy. Despite being a chronic condition, the edges and size of the ring allowed for adequate repair.
In most cases, acute diaphragmatic ruptures are addressed through an exploratory laparotomy or abdominal laparoscopy. This allows for the exclusion of associated intra-abdominal injuries that may be potentially life-threatening. Although less common, a thoracic approach can also be chosen. Diagnostic laparoscopy is used in patients at high risk of diaphragmatic injury, especially if another visceral injury is not suspected (e.g., in the case of a stab wound in the lower thorax) [13].
During exploratory laparotomy or laparoscopy, the diaphragm should be thoroughly examined for possible injuries, as these can easily go unnoticed. According to a study, approximately 14% of injuries are missed during the initial laparotomy [26]. This situation may result, in part, from the difficulty in visualizing the hemidiaphragms and smaller injuries often present in penetrating traumas. Small defects are usually closed primarily using non-absorbable sutures [27]. For larger diaphragmatic defects, it may be necessary to use a prosthetic mesh to ensure tension-free closure. In case the surgical field is contaminated, alternative methods such as using biological mesh, vascularized tissue flaps, or a temporary absorbable mesh may be considered, with planning for subsequent reconstruction. Placing an intercostal drainage above the repair is advised to prevent the development of reactive pleural effusion. Patients with smaller tears may experience a delayed presentation and develop subsequent herniation of abdominal contents, often manifesting with gastrointestinal discomfort related to volvulus or incarceration of abdominal viscera.
The rarity of post-traumatic diaphragmatic hernias warrants meticulous evaluation in a patient with respiratory, cardiovascular, or digestive symptoms and a history of abdominal or thoracic trauma. Early identification facilitates therapy, increases the patient's years of quality life, and decreases the risk of recurrence.
It can be concluded that late diaphragmatic rupture is a condition often linked to previous thoracoabdominal trauma and presents with nonspecific symptoms that can worsen and endanger life. Therefore, it is crucial for the surgeon to be familiar with this condition to ensure appropriate treatment.