Background: Laparoscopic sleeve gastrectomy (LSG) is a common bariatric surgery and has its discrete advantages or disadvantages as compared to more complex bariatric procedures. Several studies have reported increased incidence of de novo gastroesophageal reflux (GERD) or its aggravation following LSG. Since GERD causation is multifactorial, no ideal method or technique exists to overcome this challenging complication especially associated with LSG. GERD affects quality of life and is a risk factor for pathological progression to Barret’s esophagus and its sequelae. Our goal was to analyze whether the adding omentopexy (OP) to LSG impacts GERD symptomatology in the long term follow up.
Methods: This is a single institution case control study including two groups of morbidly obese patients who underwent LSG in a university hospital. Patients were grouped under omentopexy (OP) or no omentopexy (NP) categories. Patient characteristics such as age, sex, ASA (American Society of Anesthesiologists) risk, body mass index (BMI), nutritional status and co morbidities were comparable. Postoperative follow up was scheduled at one week, one, three, six and twelve months and yearly thereafter. All received standard post-operative clinical, nutritional evaluation and PPI therapy for at least the first 3 months.
Results: A total of 107 patients underwent LSG from January 2012 to December 2014. Out of these, 71 had OP while 36 had NP were considered for analysis. These patients had at least 5 years of post-operative follow-up with our institution. LSGs in both groups were performed by our experienced surgeons using bioabsorbable staple line reinforcement (BSLR) groups. Preoperative and post-operative presence or absence of GERD symptoms were recorded using simple questionnaire at the follow up visit or over the phone. Post-operative symptoms of GERD were subcategorized as either no change, worsening or improvement in symptoms. In NP group, 26 out of 36 patients (72%) had unchanged symptoms, 9 out of 36 patients (25%) had worsening and 1 out of 36 patients (2.7%) had improvement in GERD symptoms. While 58 out of 71 patients (81%) in OP group had unchanged symptoms, 6 out of 71 (8.4%) had worsening and 7 out of 71 (9.8%) had improvement in symptoms 5 years after surgery. The above difference reached statistical significance between OP and NP groups with P value of 0.03 (< 0.05). While OP group had on average 15-20 minutes longer operative time, but no significant difference was seen in the of length of stay.
Conclusions: Our study indicates that adding OP to LSG may have some desirable effects on GERD symptomatology. However, larger, and controlled clinical trials are called for to uphold its validity in bariatric patients.
LSG: Laparoscopic Sleeve Gastrectomy; OP: Omentopexy; NP: No omentopexy; HH: Hiatal Hernia; BMI: Body Mass Index; GERD: Gastroesophageal Reflux Disease; DM: Diabetes Mellitus; OA: Osteo Arthritis; CI: Confidence Interval; SD: Standard Deviation; ASA: American Society of Anesthesiologists; Mg: milligrams
Bariatric surgery is the most effective resolution to morbid obesity. With the current ASMBS estimates 60-65% of bariatric surgeries are LSGs (Laparoscopic sleeve gastrectomies). LSG is the preferred procedure due to its decreased technical complexity and comparable results [1]. Obesity is a significant risk factor for development of GERD, with over half of these patients suffering from symptomatic GERD [2]. There are multiple mechanisms involved in the pathogenesis of GERD ranging from gastro esophageal motility disorders, impaired lower esophageal sphincter (LES) resting tone, transient LES relaxations (TLESR), impaired esophageal acid clearance and delayed gastric emptying. Many patients with GERD have associated hiatal hernia along with morbid obesity [3-5]. Obesity is independently responsible for GERD through its effect on anatomical alterations to the esophago-gastric junction (EGJ), negative impact on transient relaxation of the lower esophageal sphincter (LES) and/or increasing risk for development of a hiatal hernia (HH), further exacerbating GERD [6]. In obese individuals, visceral fat, organomegaly, and elasticity of support core muscles and ligaments are important in generating an elevated IGP during inspiration and expiration, which is responsible, in turn, for increasing the gastroesophageal pressure-gradient during inspiration. While HH impairs the EGJ flap, changes intragastric pressure (IGP) relative to the LES thus affecting its competence [7]. Therefore, gastric contents may easily reflux into the esophagus. LSG may inherently predispose to GERD or its worsening due to its iatrogenic creation of an anatomical configuration ultimately affecting the integrity of cardia and incisura angularis. Which we believe affects intragastric pressure and competence of both gastroesophageal and pyloric sphincter resulting in symptomatic or asymptomatic GERD [8]. Addition of omentopexy improves the abnormal anatomical configuration at the level of incisura angularis, lowers intragastric pressure and possible GERD improvement in some patients.
This is a single institution case control study performed at our university hospital. Data was collected using the hospital and MBSAQIP database. The study was exempt from Institutional Review Board (IRB) due to the retrospective nature of the study. All patients who underwent LSG from January 2012 to December 2014 were included. Patients are referred to our center from several sources such as our weight management program, primary care physicians and other specialties were included. All patients undergo a selection process that includes nutritional, psychological, medical, and GI assessment. Bariatric procedures are discussed with all patients prior to surgery. And written informed consents are obtained. Risks, benefits, and complications of all bariatric procedures are discussed. Our patients undergo upper endoscopy as part of preoperative evaluation and placed on a pre-operative ‘liver shrinking’ diet (600-800 Cal/day) for at least two weeks. We used size 40 or 44 Fr bougies for calibrating the sleeve sizes in both groups.
Proton pump inhibitor (PPI) therapy is routinely given postoperatively for the first ninety days. This treatment is based on additional clinical indications of either symptomatic reflux esophagitis or history of peptic ulcer disease.
Two surgeons A, B performed LSG at our institution during the year 2012 to 2014. Their techniques are at par with current standards of performing LSG in United states. We use 40-44 Fr Size boogies for gastric sleeve calibration. Surgeon A performs OP, while surgeon B does not perform OP. Both Surgeons A and B perform LSG using BSLR. Surgeon A believes in selectively performing hiatal herniorrhaphy and LSG, if HH is present. While surgeon B routinely performed laparoscopic gastric bypass as standard operative procedure in those with severe preoperative GERD.
In the OP group, the pexy was performed using braided non-absorbable interrupted sutures. Three sutures were placed to tack the posterior wall of the sleeved stomach to the remnant greater omentum, as shown in Figure 1 and Figure 2.
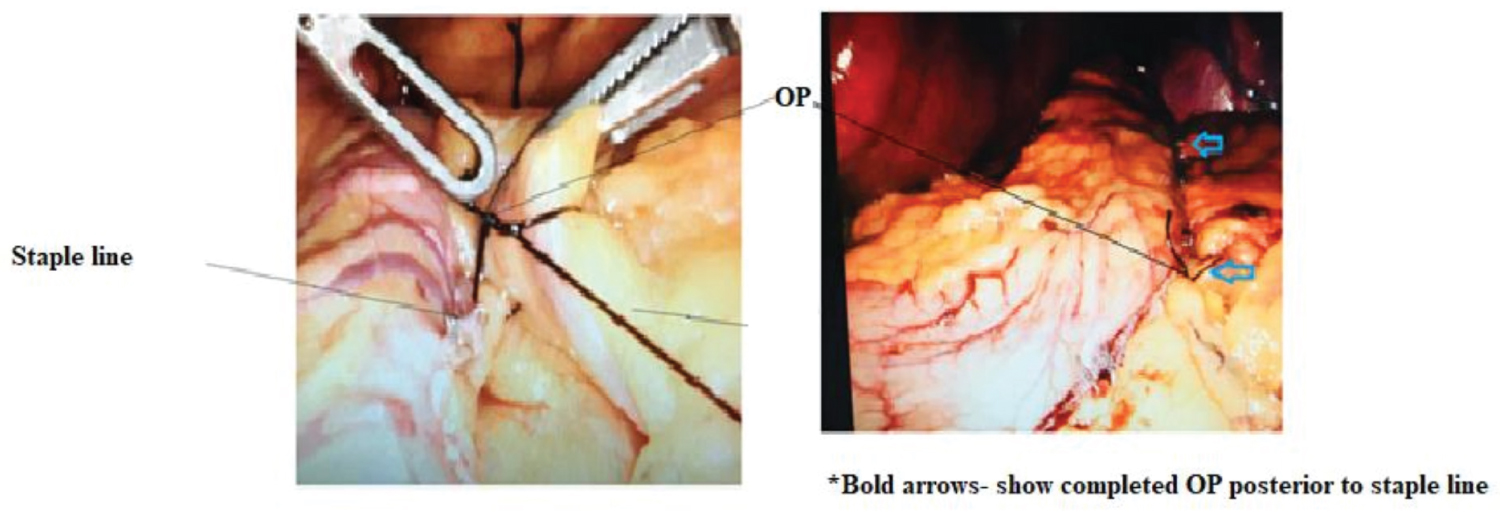 Figure 1: Method of performing omentopexy (OP).
View Figure 1
Figure 1: Method of performing omentopexy (OP).
View Figure 1
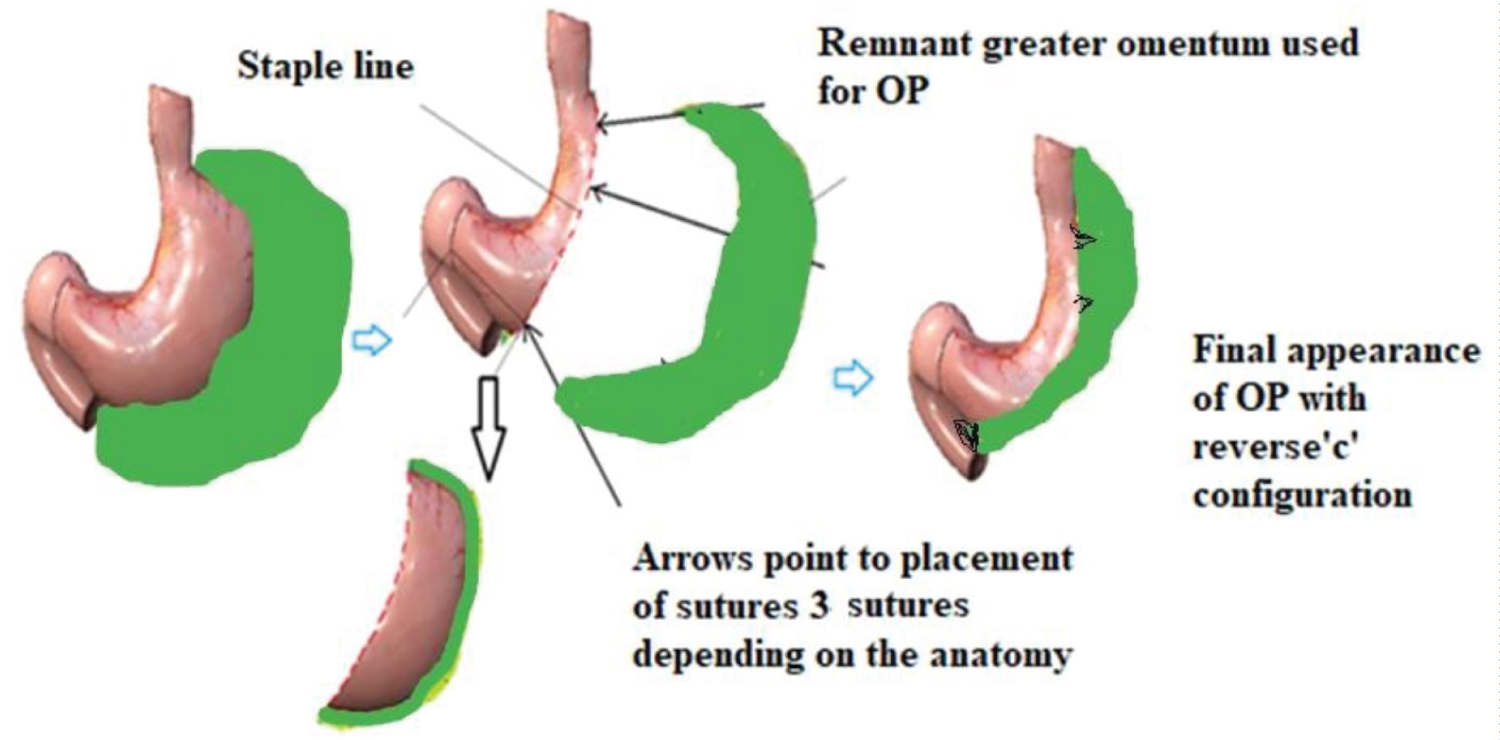 Figure 2: OP Step by Step approach (Note: no suture at the level of incisura angularis).
Figure 2: OP Step by Step approach (Note: no suture at the level of incisura angularis).
OP: Omentopexy.
View Figure 2
With this technique it is ensured that the staple line remains accessible, should there be any bleeders to be dealt with at the end of the case. The layout of the sutures is assessed based on the tension needed to achieve a smooth contour at the staple line interface and therefore specific fixation sites are chosen (described in detail below). The result is a smooth anatomical configuration with reverse-C shaped configuration to prevent any wind-sock deformities or twisting of the gastric sleeve.
Our goal when performing LSG is to keep the angle at incisura angularis more obtuse. Figure 3 demonstrates upper GI studies done during follow up in some symptomatic patients in the two groups for comparison per se.
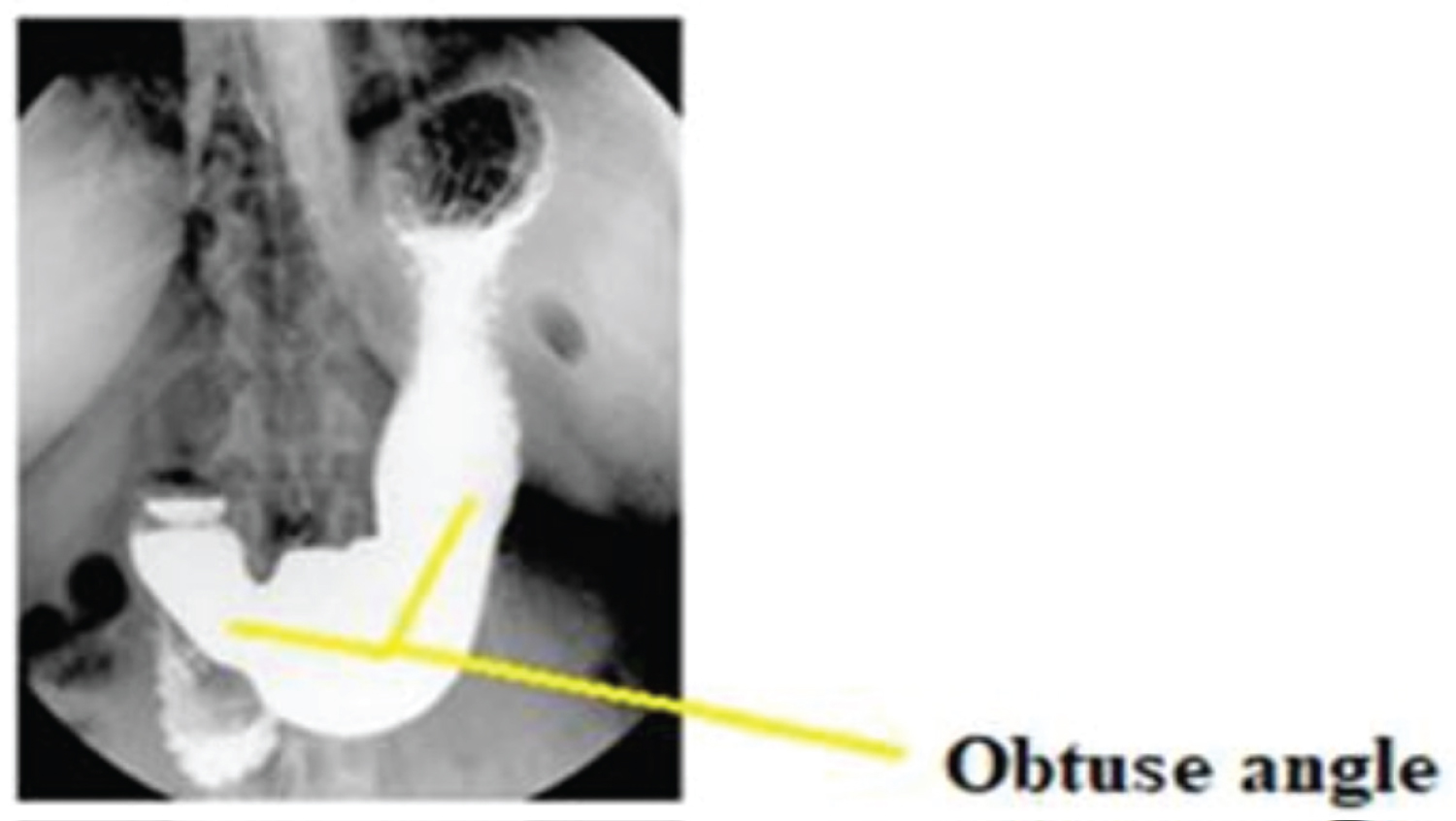 Figure 3: UGI study in a patient with OP, demonstrates "obtuse" angle at incisura angularis.
Figure 3: UGI study in a patient with OP, demonstrates "obtuse" angle at incisura angularis.
UGI: Upper Gastrointestinal
View Figure 3
As seen in Figure 4, the lateral traction from the previously attached greater omentum is lost after LSG. This causes an imbalance in the forces on the sleeved stomach making the anatomical configuration in NP group as “L-shaped” as opposed to a “reverse C-shaped” in OP group.
 Figure 4: Compromised gastric outlet due to acute angle at incisura in a patient without OP.
Figure 4: Compromised gastric outlet due to acute angle at incisura in a patient without OP.
OP: Omentopexy
View Figure 4
Enhanced recovery after surgery protocol (ERAS) was followed except for preoperative carbohydrate treatment. The postoperative orders, pain management, and discharge protocol are standard for our LSG patients. Patients are kept NPO (Nil per os) during the day of surgery and following clinical evaluation bariatric clear liquids commence on first post-operative day. Intravenous acetaminophen starts on the day of surgery for adjunctive pain management. We usually do not start post-operative NSAIDs or enoxaparin if there is any clinical indication of bleeding. Patients are discharged after overnight observation and are sent home with three months of prescription PPIs. Post-operatively they are followed up at one week, one, three, six and twelve months and then once a year. Comorbidity assessment and nutritional status are evaluated routinely at each visit. Starting at third month follow up routine and anemia labs are obtained, which includes complete blood count and measuring serum iron concentration, total iron binding capacity (TIBC), transferrin saturation. Patients are treated with iron supplements, multivitamins, and vitamin B12.
Routine post-operative upper GI study or endoscopy was not performed, unless clinically indicated. Patients with HH were excluded from the study, while those with GERD or using antacids for reflux were included in the study. These patients were followed surgery to assess any improvement, worsening or change in their reflux symptoms at their follow up visits. The GERD symptomatology was assessed using a simple questionnaire that included questions specific to GERD and use of Antacids or PPIs. Some patients who failed to follow up were interviewed over the phone for presence of GERD and use of PPIs. The symptoms were then classified as unchanged, worsened, or improved. Of note those patients who reported switching the antacids from H2 blockers to proton pump inhibitors or using more than one antacid were categorized under worsening of GERD symptoms. Patients who discontinued use of antacids were classified to have improved symptoms.
Statistical analysis and Power analysis were performed to check for adequacy of the sample size. Standard univariate methods were used to express continuous variables with respect to mean, standard deviation and 95% confidence intervals. Discrete variables were expressed as proportions. Comparison was performed by using Chi square test. A two-sided p value of 0.05 was considered significant. The study was conducted with the understanding that there are multiple factors causing GERD, including but not limited to patient factors and operative technique. Regression analysis was performed for all these factors. Regression analysis was also performed to evaluate for factors that would affect postoperative outcomes such as age, ASA class, BMI, co morbidities, gender, and anemia.
A total of 107 patients were included in our study, that underwent LSG from January 2012 to December 2014. Those with Barrett’s esophagus and hiatal hernias were excluded. The technique and selection criteria are similar for both surgeons. Preoperative endoscopy and if necessary UGI study were performed for all patients. Those who had hiatal hernia were completely excluded from this study. Out of 107 patients, 71 had OP while 36 had NP were included for analysis. Patients with at least 5 years of post-operative follow up were included in the study. LSGs in both groups were performed by our experienced surgeons using bioabsorbable staple line reinforcement (BSLR) groups. Preoperative and post-operative presence or absence of GERD symptoms was documented based on use of antacids and using simple questionnaire either at follow up or over the phone to assess for presence of GERD symptoms. Post-operative symptoms of GERD were subcategorized as either no change, worsening or improvement in symptoms of GERD. In NP group, 26 out of 36 patients (72%) had unchanged symptoms, 9 out of 36 patients (25%) had worsening and 1 out of 36 patients (2.7%) had improvement in GERD symptoms. While 58 out of 71 patients (81%) in OP group had unchanged symptoms, 6 out of 71 (8.4%) had worsening and 7 out of 71 (9.8%) had improvement in symptoms 5 years after surgery. The above difference reached statistically significance between OP and NP groups with P value of 0.03 (< 0.05). While OP group had on average 15-20 minutes longer operative time, no significant difference was seen in the of length of stay. This is shown in Table 1.
Table 1: 5-year outcomes of LSG with and without omentopexy. View Table 1
As discussed, the technique of performing LSG per se was similar in the two groups, including the choice of stapler device. Their demographics, BMI, ASA class and co morbidities were also comparable as shown in Table 2.
Table 2: Demographics of patients undergoing LGS with or without OP. View Table 2
All patients were explained the risks, benefits, and complications of doing standard laparoscopic sleeve gastrectomy. Alternative bariatric operations were discussed, and informed consents were obtained. Choice of OP or NP was operating surgeon’s preference which was separately discussed during preoperative sessions. It was noted that intraoperative time was 15-30 minutes longer in the OP group as compared to NP group. Postoperatively, all patients were followed at 1 week, 1, 3, 6 and 12 months intervals and once a year for five years.
The finding of reflux was based on preoperative diagnosis of GERD based on endoscopic findings or clinical findings. This further dictated the need for acid reducing therapy in the two groups beyond three months after LSG.
As shown in Table 2 a total of 7 out of 71 patients had improvement in GERD in the OP group as compared to 1 out of 36 patients had improvement in GERD in the NP group. Symptoms of GERD remained same or unchanged in 58 out of 71 patients in OP group, versus 26 out of 36 patients in NP group. While 6 out of 71 patients reported worsening of GERD symptoms in OP group. And 9 out of 36 patients reported worsening of GERD symptoms in the NP group. Upon performing statistical analysis between three groups and two surgical options above, using chi square test the p value reached statistical significance of 0.03 (< 0.05). Other complications were comparable between the two groups where most of the GERD in the OP patients were managed conservatively using proton pump inhibitor therapy. The remaining Four patients in the NOP group were treated using revision or conversion to Roux-en-Y procedure, due to worsening of GERD despite maximum medical therapy. There was no mortality rate in any of the two groups. GI obstructions or leaks were not seen in any of the groups.
Details of medical management including but not limited to proton pump inhibitors or H2-blockers prescribed are as shown in Table 3 and Table 4.
Table 3: Preoperative and post-operative GERD symptomatology management for OP. View Table 3
Table 4: Preoperative and postoperative GERD symptomatology management for NOP. View Table 4
As noted, most of the patients did not have GERD before undergoing surgery. However, postoperatively greater number of patients had relief of GERD after OP as compared to NOP group. The actual distribution of medical therapy is demonstrated in Figure 5 and Figure 6. Regression analysis was carried out for possible factors affecting leaks, reflux, or bleeding. These were surgical approach, staple line reinforcement, use of fibrin glue, co morbidities, size of boogies (40 versus 44 Fr), omentopexy and BMI. None of these, except the omentopexy (OP) or NP showed some correlation. All patients were followed postoperatively at one week, 1, 3, 6 and 12 months and had nutritional evaluation with micronutrient supplementation as necessary.
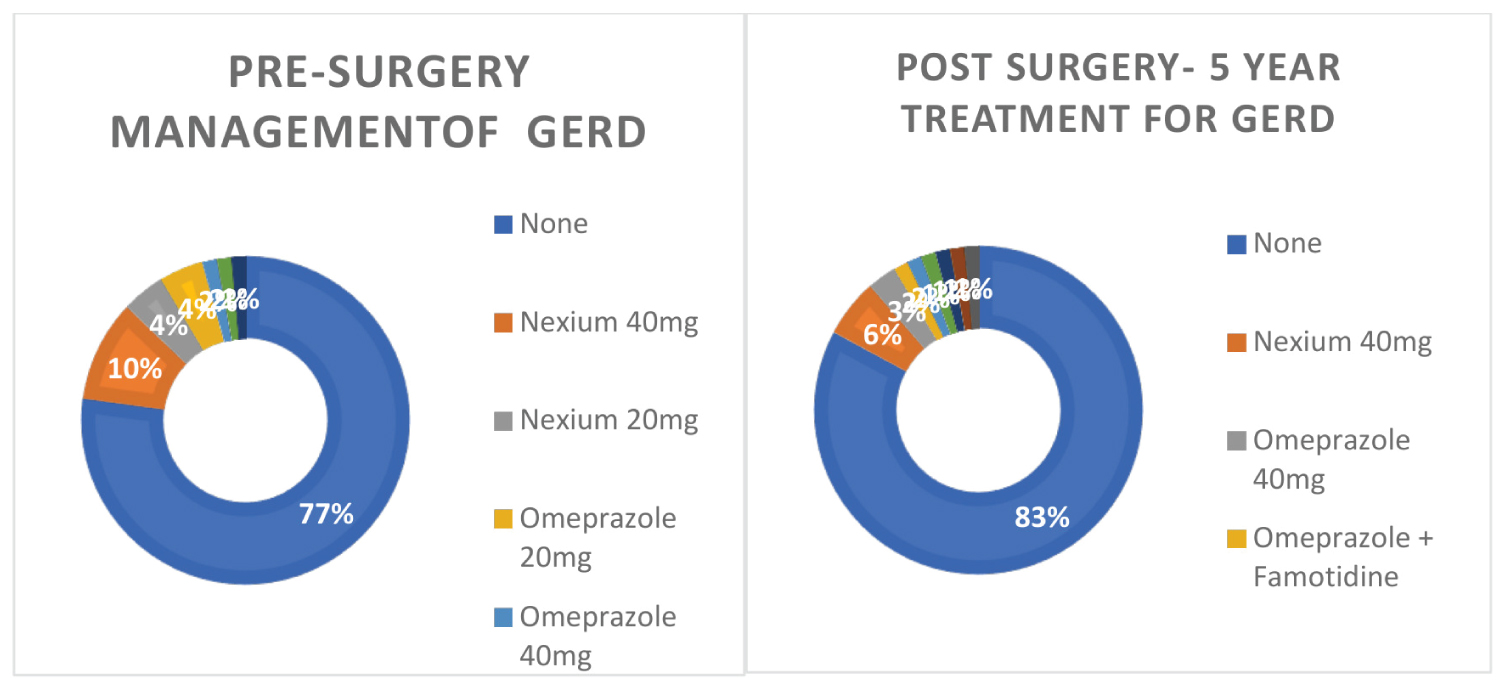 Figure 5: Change in reflux symptoms and medical management seen after LSG with OP.
Figure 5: Change in reflux symptoms and medical management seen after LSG with OP.
mg: milligrams; GERD: Gastrointestinal Reflux Disease; Pre: Preoperative; Post: Postoperative.
View Figure 5
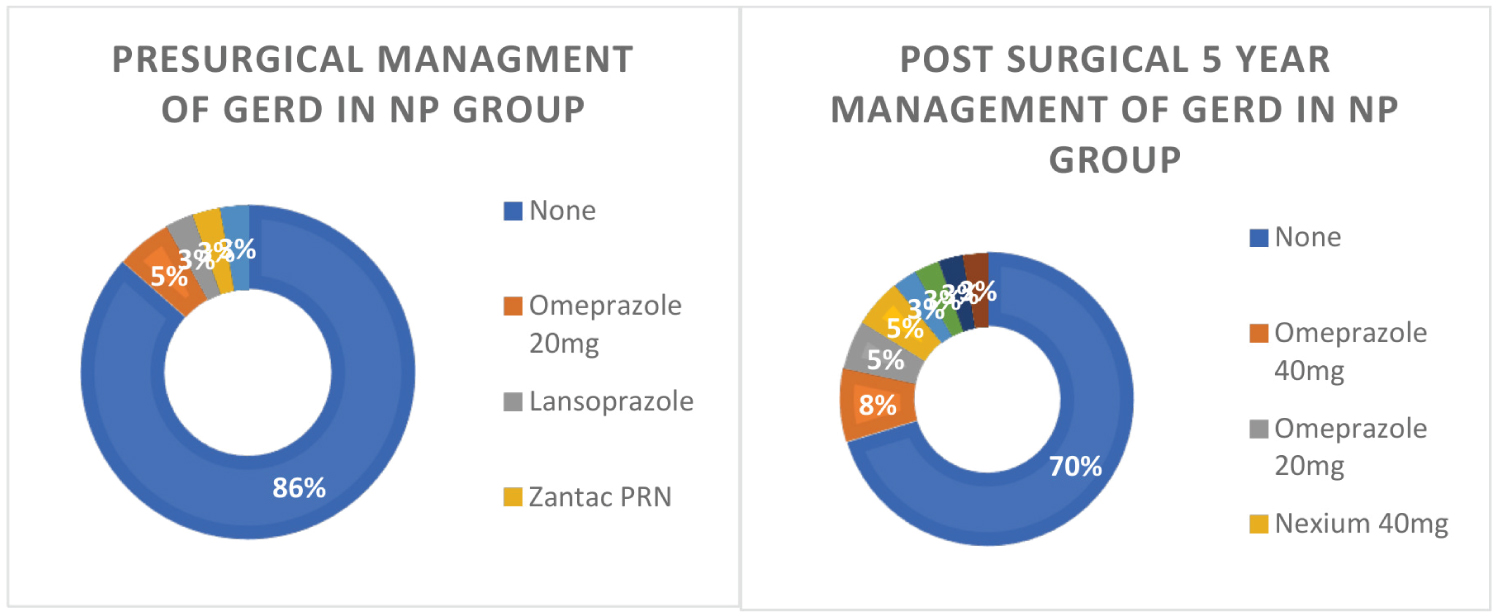 Figure 6: Change in reflux symptoms and medical management seen after LSG with OP.
Figure 6: Change in reflux symptoms and medical management seen after LSG with OP.
mg: milligrams; GERD: Gastrointestinal Reflux Disease; Pre: Preoperative; Post: Postoperative; OP: Omentopexy; NP: No Omentopexy
View Figure 6
Regression analysis was carried out for possible factors affecting leaks, reflux, or bleeding. These were surgical approach, staple line reinforcement, use of fibrin glue, co morbidities, size of boogies (40 versus 44 Fr), omentopexy and BMI. None of these, except the omentopexy (OP) or NP showed some correlation. All patients were followed postoperatively at one week, 1, 3, 6 and 12 months and had nutritional evaluation with micronutrient supplementation as necessary.
GERD is a multifactorial condition commonly seen in both obese and non-obese individuals. It typically manifests with GI symptoms of heartburn, regurgitation and or dysphagia. Its atypical manifestation includes extra-esophageal symptoms such as chest pain, dental erosions, chronic cough, laryngitis, or asthma [9-11].
A barrier valve mechanism exists between the esophagus and the stomach, in the form of LES (Lower esophageal sphincter) which is influenced by adjacent anatomical structures [12]. The LES consists of intrinsic and extrinsic components. The intrinsic component of the LES consists of esophageal muscle fibers and is under neurohormonal control. The extrinsic component consists of the diaphragmatic crurae and the phreno-esophageal ligament, which provide adjunct anatomical support to the LES and further protect against gastric reflux [13].
Transient lower esophageal sphincter relaxation (TLESR) is a phenomenon responsible for acid reflux in normal subjects and those with GERD. TLESRs are spontaneous LES relaxations of 10-60s duration, which are unrelated to swallowing [14,15]. A higher percentage of TLESRs is associated with reflux in GERD patients as compared to normal individuals [3,16-19]. An important trigger for TLESR appears to be post prandial gastric distension, via stimulation of proximal gastric tension and stretch receptors. In addition to LES resting pressure, its frequency is also influenced by endogenous hormones such as cholecystokinin, medications, specific foods, and dietary habits [20].
GERD is associated in up to 50% of morbidly obese patients [2,13]. Clinical experience suggests that GERD is positively affected by weight loss [21]. A substantial proportion of weight loss achieved with bariatric surgery helps nullify the clinical course of GERD seen in many patients. LREYGBP may be the primary consideration in morbidly obese patients with GERD. Studies have shown benefits of LREYGBP in decreasing acid exposure at lower esophagus [22,23]. However, not every patient is a candidate for LREYGBP. LSG in recent times has gained popularity due to its technical feasibility and comparable satisfactory weight loss results. Unfortunately, the same is not applicable to its complications such as leaks, bleeding, gastric strictures, gastric twist, and GERD. These complications are at times more morbid than the complications associated with gastric bypass; and the only alternative remains its conversion to gastric bypass due to comparatively lower incidence of GERD [24]. LSG can cause worsening, improvement or de novo GERD depending upon several factors. The incidence of de novo GERD following LSG could range up to 35% with new-onset esophagitis ranging from 6.3% to 63.3% [25,26]. There are several anatomical alterations causing reflux after LSG. Such factors are related to removal of gastric fundus, concurrent presence of hiatal hernia, anatomical or physiological changes in LES pressures, reduced gastric compliance and narrowing at the level of angle of his between vertical and horizontal portions of the sleeve [7]. Other factors such as disruption of the angle of His and division of sling fibers also play significant role in causing post-operative GERD after LSG [27]. Likewise factors contributing to improvement of GERD after LSG result from decreased intra-abdominal pressure due to weight loss, reduced acid production from resection of the acid-producing gastric fundus and accelerated gastric emptying with reduced gastric volume [28,29].
Various surgical solutions to prevent GERD after LSG are available, but not widely accepted such as sleeve with fundoplication, GE junction plication using falciform ligament, amongst a few [30,31]. No literature is available to gauge the effectiveness or beneficial evidence of these preliminary procedures. As we discussed, a few small studies have reasonable success with LSG and fundoplication. However, long term impact of keeping portions of gastric fundus in these studies on weight loss remains to be seen [32]. Likewise, the results of magnetic sphincter augmentation after sleeve gastrectomy, based on small studies and case reports are limited and met with potential complications at this time [33,34]. Therefore, to date there is no definitive resolution to medically refractory GERD after LSG, except conversion to REY gastric bypass anatomy. There are no better alternatives to medical management than sphincter augmentation or conversion to gastric bypass.
Omentopexy also has been studied to some extent with differences of opinion amongst surgeons regarding its benefits. Proponents of OP suggest that this technique can decrease the important complications of LSG such as gastric leaks, bleeding, and GERD without changing the weight loss outcomes [35-37]. While the proponents of LSG without pexy (NP) believe that adding OP is of no value in reducing any of these complications and that OP only increases operative time [38-40].
The technique of performing LSG is fundamentally standardized across the United States with minor variations or modifications. Surgeon preferences are seen in the use of variable size bougies, staple line reinforcements and/or omentopexy (OP) may influence the outcomes after LSG. Although many bariatric surgeons use 36-40 Fr bougies for calibrating gastric sleeves. There is no discrete evidence regarding this choice.
We use 40 and 44 Fr bougies for females and males respectively. This choice also depends on the fact that we are a center training bariatric fellows. Given the circumstances a larger bougie size would avoid dreadful complications such as gastric leak. This has been shown in a few studies. We believe the size of bougie may not affect GERD. No data is available to prove or disapprove this belief. The impact of OP on gastric reflux has been the least studied and remains controversial. Larger, controlled trials are unavailable to objectively assess its role in patients with GERD. In this small study we have attempted to subjectively evaluate the utility of adding OP to LSG in improving or worsening GERD symptoms.
No data exists for duration of post bariatric antacid therapy. Clinically, different programs have variable post-operative protocols regarding the use of antacids. In general, we recommend 90 days of therapy. However, after 30 days we evaluated and tapered antacid therapy based on resolution of symptoms. We discontinue antacids for those who do not have any symptoms after 90 days. Hence this choice is arbitrary.
Clinically we believe that the factor of gastric distension as described above leading to TLESR is non-existent in a standard LSG primarily due to absent fundus. Influence of LSG on LES pressure could largely be due to distortion of extrinsic barrier components (crura and phreno-esophageal ligament) especially if HH dissection is concomitantly performed. Additionally, the role of pyloric sphincter both on acid and bile reflux is unknown as this could affect the clinical outcomes.
No studies are available to analyze the role of pyloric sphincter (PS) for GERD, as theoretically increased PS tone would increase intragastric pressure leading to higher incidence of GERD or bile reflux. While incompetent PS, along with diabetic gastroparesis could lead to increased risk of duodeno-gastric reflux/bile reflux [41]. LSG with comparatively reduced intraluminal radius, augments intraluminal/intragastric pressure, according to the principles of Hagen-Poiseuille Law [42,43]. This intraluminal pressure is further adversely affected by iatrogenic gastric narrowing, partial or complete closed loop gastric obstruction and narrow angle at incisura during gastric sleeve construction. It’s unclear how these changes would affect the pyloric and lower esophageal sphincters. With the addition of OP to LSG we propose that a wider angle at incisura angularis mitigates increased intragastric pressure to a certain extent. This phenomenon could be a favorable factor in reducing GERD although its impact. The complication of GERD after LSG is debilitating and significantly affects patient’s quality of life and its severity is proportional to use of antacids. The extrinsic component of LES consists of the diaphragmatic crura and the phrenoesophageal ligament, which provide anatomical support to the LES and further protection against gastric reflux [19]. Factors contributing to change in GERD symptoms after LGS could be weight loss, hormonal changes affecting LES and even change in frequency or intensity of TLERS. Preservation of anterior phrenoesophageal ligament during LSG is of benefit in causing favorable anatomical changes and possibly reduce GERD [44]. Increased angle at incisura angularis is probably associated with decreased intragastric pressure, with decreased incidence of GERD.
Patients who underwent gastropexy showed a significant reduction in antiemetic consumption, postoperative nausea, vomiting, GERD symptoms and gastric torsion than those who did not undergo gastropexy [45]. The current work hints omentopexy benefits in patients undergoing LSG, with overall better outcome as regards to the upper gastric upset and GERD compared to LSG alone [35]. LSG with omentopexy improved the clinical score of GERD in most cases and did not cause significant changes in the LES tone. The presence of reflux did not exacerbate the clinical score of GERD [38].
Another study demonstrated that, omentopexy decreased the incidence of acid reflux, gastric kink, volvulus, and intrathoracic migration. Moreover, food tolerance significantly improved in patients, which in turn led to higher compliance with the postoperative dietary plan and better outcome regarding weight loss. In addition, omentopexy showed lower incidence of postoperative leakage [39]. Other studies have shown that omentopexy does not have a significant effect on reducing the incidence of de novo GERD after LSG, even in those with higher BMI [40]. Its believed that omentopexy itself does not change the outcome for laparoscopic sleeve gastrectomy in terms of non-specific gastrointestinal symptoms or weight loss results [36].
Some studies have contradictory experiences with OP. These have shown that omentopexy did not have a significant impact on the prevention of post-LSG complications and is associated with longer operative time. Some studies have suggested that OP may serve as an extra guard against leakage, bleeding, vomiting, and GERD, manifested by the decreased incidence of these complications with that technique [38]. We have likewise seen some of these benefits in our prior research analysis that showed decreased leaks and bleeding complications [43].
We believe that the combined benefits of LSG and omentopexy in GERD may be- 1) Fundectomy with LSG decreases incidence of TLERs, 2) Increased IG pressure due to decreased volume of remnant sleeve gastrectomy, 3) Lower IG pressure due to the addition of OP, 4) Possibly favorable hormonal impact of LSG on gastric emptying, LES and PS. All these clinical findings or factors require research scrutiny using a larger randomized control trial to derive meaningful conclusions. Some of the important limitations of our study include- exclusion of patients with hiatal hernias and objective measurement of GERD is missing. Our study mainly focused on patient symptoms, making the subjective symptom analysis debatable. We know that it’s possible to have asymptomatic GERD further limits the study. Our study is also limited by its small sample size and has disadvantages inherent with case series. As with any retrospective study, analysis depends on the availability and accuracy of the medical record. The study is subject to selection bias and is uncontrolled due to limitations of any retrospective study. Therefore, a more controlled prospective analysis is called for to further understand the role of OP on postoperative GERD in patients with concomitant LSG and OP. Further studies involving large samples are still required to certify the above proposed relationship between GERD and Omentopexy in the setting of LSG.
Nitin Sharm, MD and Wai Yip Chau, MD have not received fees for serving as a speaker, such as consultant and/or an advisory board member] for Penn Medicine Princeton Medical Center, NJ.
Nitin Sharm, MD and Wai Yip Chau, MD have not received research funding from any entity/individual for this research project.