Mesenteric cysts are rare benign lesions occurring in the abdomen. The cystic lesions can be asymptomatic or present with a specific symptoms. When discovered, treatment is either open or Laparoscopic surgery. We present a case of 29-years-old woman with one year history of progressive increasing abdominal swelling after her first delivery via caesarean section. It was initially painless however occasional pain was noticed some months prior to presentation at the out-patient department.
Examination revealed a palpable mass occupying the whole abdomen. Ultrasound scan of the abdomen suggest the 30 cm × 20 cm cystic lesion, which was reported as right ovarian cyst and computed tomography scan could not be done due to financial constraint. Exploratory laparotomy revealed a huge cyst protruding out of mesentery of the transverse colon displacing the small bowels sideways and downward. The excised cyst found to have a thick wall and unilocular measured 35 cm × 20 cm in diameter. It was internally lined with fibrinous exudate and contained dark brown fluid. The patient had an uneventful postoperative recovery. Histopathology of the cyst showed a benign haemorrhagic cyst of the mesentery.
Mesenteric cyst, Transverse colon, Unilocular cyst
Mesenteric cysts are rare cyst located in the mesentery of the small bowel or colon [1,2]. They are uncommon benign intra-abdominal tumours that occur across the life course, with a reported incidence of 1/100,000 in adult and 1/20,000 in children and a female to male ratio of 2: 1 [3]. Depending on their size and location, these cysts are often asymptomatic and are thus discovered incidentally during routine imaging. Symptomatic cases may present with acute or chronic vague abdominal pain (55%-81%), a palpable mass (44%-61%) abdominal distension (17%-61%), nausea and vomiting (45%), constipation (27%) or diarrhoea (6%).
Mesenteric cysts are classified as chylolymphatic, simple (mesothelial), enterogenous, urogenital remnant and dermoid (teratomatous cyst) [4]. Completion surgical excisions, by either open or laparoscopic approach ensures the lowest risk of recurrence. This report highlights the case of a 29-years-old who presented symptomatically and was successfully managed by open surgery as laparoscopic technique was not available in our centre.
A 29-years-old woman presented at the surgical outpatient department of the hospital with a year history of progressive abdominal swelling that was initially painless and few month prior to presentation developed occasional abdominal pain. The abdominal swelling was noticed few months after a caesarean section. However there was no history of vomiting, constipation or anorexia. Physical examination revealed the patient to be in fair general condition with no wasting. Abdominal examination revealed uniform distension with no clear delineation of any abdominal masses. Other systemic examinations were unremarkable. The initial blood workup included complete blood count, serum electrolyte and renal function all which were within normal range. The patient was hepatitis-B surface antigen negative and sero-negative for human immunodeficiency virus. Imaging investigation included an abdominopelvic ultrasound scan, which revealed a cystic mass occupying much of the abdominal cavity, with no clear site of origin. It measured approximately 30 cm × 20 cm and for a better localization and delineation of the cystic mass, computed tomogram was requested but could not be done due to financial constraint. On the basis of the presentation and imaging findings on ultrasonography, the patient was prepared for exploratory laparotomy. At surgery, the cyst was observed to occupy almost the whole abdominal cavity [5] (Figure 1 and Figure 2).
 Figure 1: Intraoperative encysted mass.
View Figure 1
Figure 1: Intraoperative encysted mass.
View Figure 1
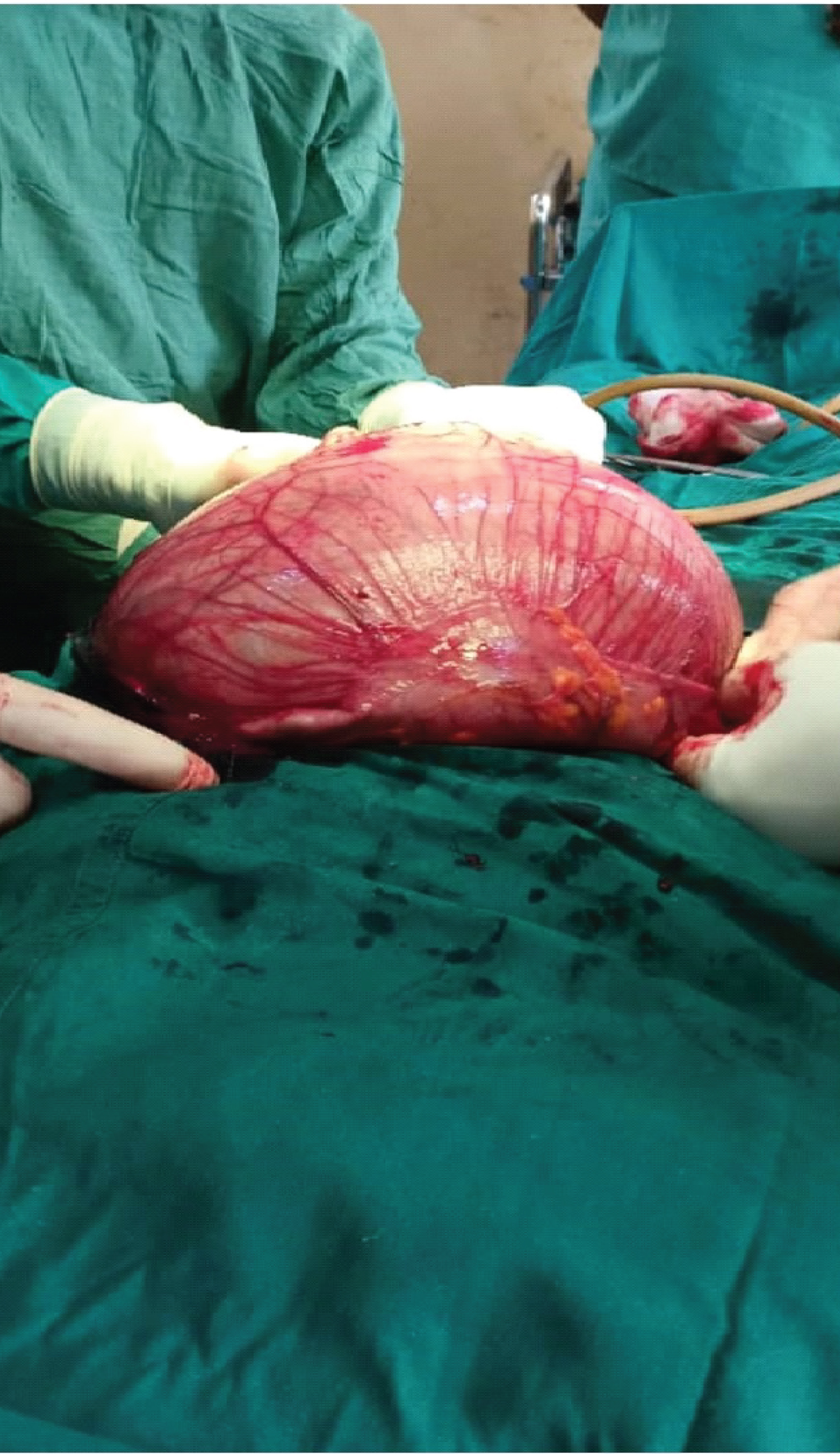 Figure 2: Encysted mass arising from the mesentery of the transverse colon.
View Figure 2
Figure 2: Encysted mass arising from the mesentery of the transverse colon.
View Figure 2
The encysted mass was partially drained to facilitate dissection, close inspection revealed involvement of the mesentery of the transverse colon. No adhesions were found between the cyst wall and the other intraabdominal structures. The cyst was carefully dissected from the mesentery of the transverse colon sparing the blood supply. Complete enucleation of the cyst was accomplished without the need for bowel resection (Figure 3 and Figure 4).
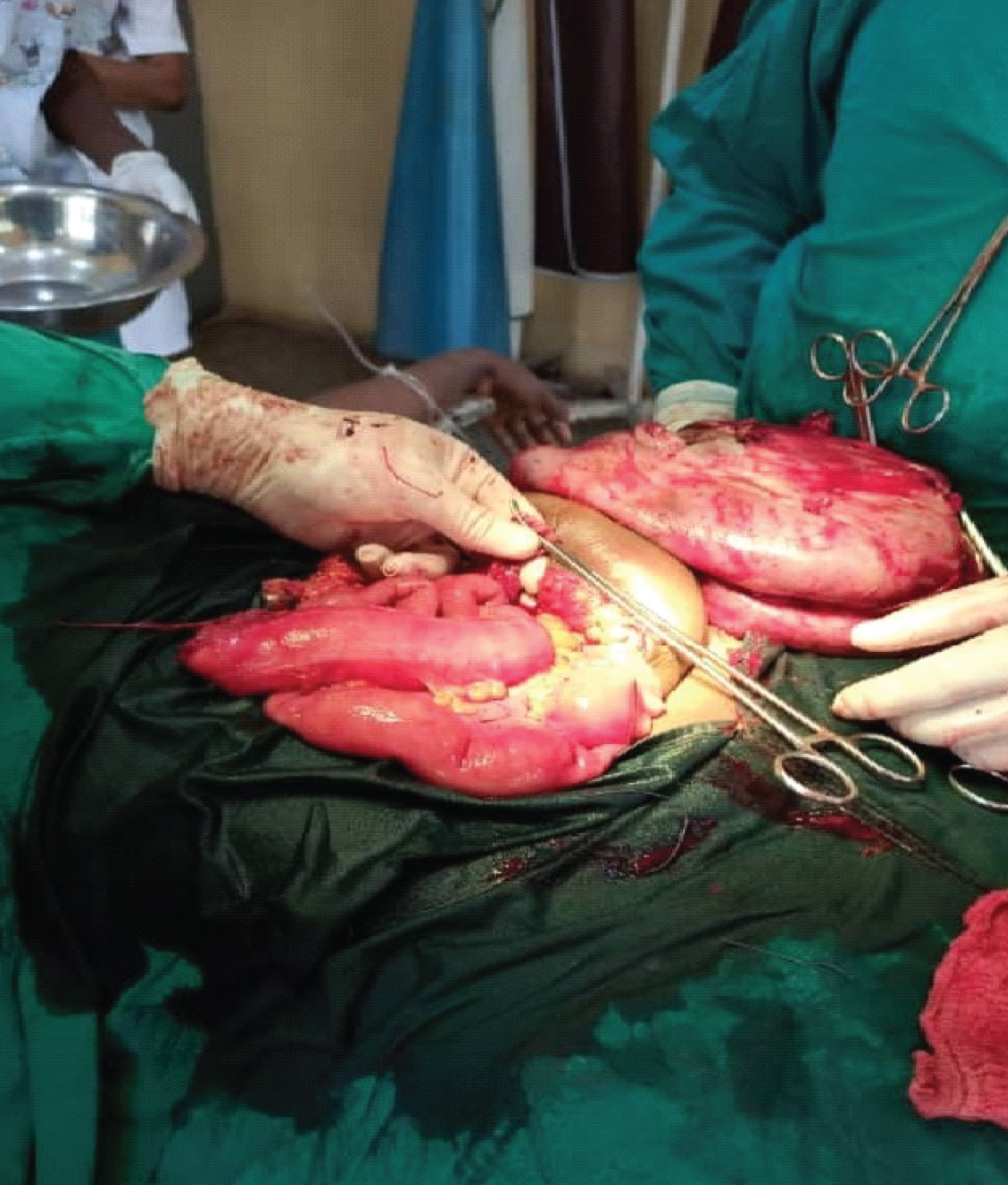 Figure 3: excised specimen containing dark green fluid.
View Figure 3
Figure 3: excised specimen containing dark green fluid.
View Figure 3
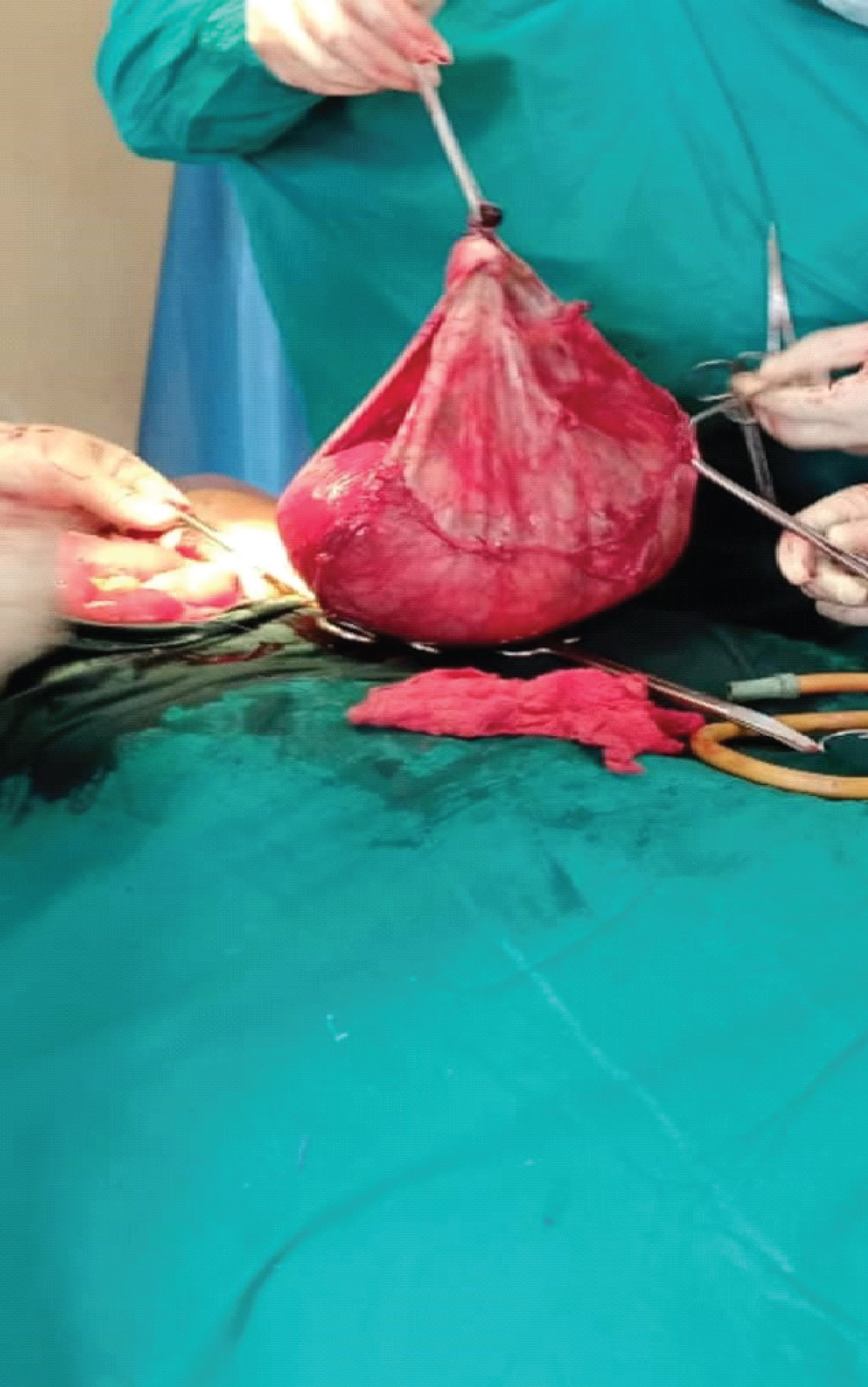 Figure 4: Completely excised cyst without bowel resection.
View Figure 4
Figure 4: Completely excised cyst without bowel resection.
View Figure 4
The final specimen sent for histopathology was a thick walled cystic mass measuring 34 cm × 20 cm. The immediate post-operative period was uneventful and the patient was discharged on the seventh postoperative day with complete healing of the surgical wound. Histopathology confirmed a benign haemorrhagic cyst of the mesentery.
Patient was seen at follow up clinic and doing fine.
Although mesenteric cysts are usually asymptomatic however they may give rise to symptoms due to compression of adjacent structure, stretching of the mesentery by rapid expansion, infection or rupture with haemorrhage. Their existence was first reported in 1507 by Benevieni, an Italian anatomist when he performed an autopsy on an 8 years old and the first effective surgical excision was performed in 1880 by Tillaux [6,7]. Mesenteric cysts are classified into i) Chylolymphatic; ii) Enterogenous; iii) Cyst of urogenital remnant; iv) Simple (mesothelial) and v) Teratomatous dermoid cysts [4].
Chylolymphatic cysts are the commonest and arise from congenitally misplaced lymphatic system, common in the ileum, thin walled, solitary and unilocular. It has got independent blood supply, so enucleation can be done without bowel resection. Enterogenous cyst arises as a diverticulum or duplication from the adjacent bowel. It is thick walled and received its blood supply from the adjacent bowel; consequently removal of the cyst always entails resection of the related portion of intestine. Clinical features include abdominal distension, vague abdominal pain, the presence of palpable mass, intestine obstruction and obstructive uropathy. Cases can also be found incidentally during other surgical procedure [8]. It has also been estimated that malignant transformation may occur in 3% of such cyst [9]. The specific diagnosis of this lesion is difficult prior to surgery as there are no pathognomonic symptoms or imaging finding as in the case. Ultrasound scan which often used in the initial evaluation, may show a well defined fluid filled cystic structure adjacent to bowel loops [8,9]. In the case reported abdominal ultrasound was reported as right ovarian cyst. Abdominal pelvic CT scan which is of great value in the localization of the mesenteric cyst could not be done in this case due to financial constraint. However, differential diagnosis may include lymphangioma, cystic teratoma, cystic lesions arising in the ovaries and cystic lesions of peritoneal origin and infectious cysts such as hydatid cysts.
In case of a large chylous cyst, especially in symptomatic cysts as in our case, surgical excision is advised to prevent a potential malignant transformation as well as development of other complications. The preferred technique entails open or laparoscopic enucleation of the mesenteric cyst, that is atraumatic separation of the cyst from the surrounding leaves of mesentery [8,10,11]. Whenever enucleation cannot be performed safely, due to adhesion of cyst wall to surrounding mesenteric tissue and/or other structures, a resection of adjacent organ may be necessary [12]. Potential treatment options have also been described such as drainage, deroofing and partial excision of cyst. These have been associated with a higher likelihood of recurrence and thus are best avoided. In our case, after initial exploration a cystic mass sized 35 cm × 20 cm arising from transverse colon mesentery was found and complete excision of the cyst with healthy borders was achieved. The postoperative period was uneventful. She was discharged home on the seventh postoperative day.
Mesenteric cysts represent a diagnostic challenge and they should be considered when a surgeon encounters an intraabdominal mass. Clinical examination and imaging do not always provide a diagnosis and surgical management should be advised due to the potential complications that may arise.
Nil.
There are no conflicts of interest.
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. The patient understands that her names will not be published and due efforts will be made to conceal her identity.