Objectives: The aim of the current study is to review patients underwent adrenalectomy either open or laparoscopic in our surgical department by the same surgical surgeon, focusing on the final diagnosis, type of operation and complications.
Methods: Retrospective review of patients who underwent adrenalectomy in our surgical department during the period from 2011 to 2021. Patient's data include age, sex, hospital stay, blood loss, operative time, tumor size, final diagnosis and complications.
Results: During the 10 years, 88 patients underwent adrenalectomy. The patient's mean age was 56.653 ± 14.28 years of age. 35 of patients were males (39.77%) and 53 were female (60.23%). Average blood loss was 49.5 ± 19.49 ml. The mean hospital stay was 4.15 ± 3.6 days.
Conclusion: Over 10 years, the increased level of experience was associated with reduced operative time, less blood loss and lower rate of complications. Laparoscopic adrenalectomy was associated with better clinical outcomes when compared with open surgery. Laparoscopic adrenalectomy can be performed safely even with tumors larger than 12 cm.
Adrenalectomy, Learning curve, Experience, Laparoscopic, Outcomes
Adrenal gland surgery represents one of the challenging operations because of the relatively inaccessible anatomical location of the adrenals and its proximity to vital structures. The prevalence of adrenal incidentaloma, which is an adrenal mass unexpectedly detected through an imaging procedure performed for reasons unrelated to adrenal dysfunction, at autopsy ranges from 1.4% to 2.9% [1]. Aging is associated with increased prevalence of incidentaloma, being < 1% among individuals younger than 30 years of age to about 7% in those over 70 years of age [2].
Indications for adrenalectomy include mainly functional adrenal tumors, malignancy and uncertainty regarding the clinical diagnosis. Surgery is indicated for functional tumors regardless of the size of tumors. It should be minded that the cortex and medulla of the adrenal gland have different embryonic origins and accordingly have different structures and functions and develop different tumors. Adrenalectomy can be performed by either laparoscopic or open techniques. Currently, laparoscopic surgery is considered the standard method for adrenalectomy. Approaches for laparoscopic adrenalectomy include trans-peritoneal or retro-peritoneal approaches. Most surgeons prefer laparoscopic trans-abdominal lateral adrenalectomy. However, open surgery is still indicated in cases of malignancy or suspected malignancy and when dealing with large tumors. Additionally, open adrenalectomy can be performed using a midline, bilateral or unilateral subcostal incision. As there is limited data on adrenal gland surgery, we aimed in this study to review our institutional experience in comparison to the existing literature. We primarily included the surgical indication, the management options and the final histopathological results for patients who had adrenalectomy by a single surgeon within 10 years of experience. Secondarily, we tried to evaluate the clinical outcomes between laparoscopic and open adrenalectomy.
We retrospectively analyzed all patients' data who underwent adrenalectomy at the General Surgery Department at James Cook University Hospital during the period from April 2011 to March 2021. All these patients underwent adrenalectomy by the same endocrine surgery consultant, Mr. Wael Elsaify. An informed consent has been obtained from all patients before the operating after thorough explanation of the purpose and possible complications of the procedures. All patients had pre-operative essential assessment including adequate history taking and clinical examination, hormonal work-up in addition to the appropriate imaging techniques by either CT or MRI. All cases have been discussed at an endocrine MDT to determine the most efficient treatment. Indications for adrenalectomy included: 1) Clinical functioning adrenal tumor; 2) Hyper-functioning adrenals secondary to pituitary tumors; 3) Significant increase in the size of the tumor regardless of the hormonal work-up result; 4) Clinical/radiological proven adrenal malignancy, and 5) Radiologically suspicious adrenal tumors.
The primary outcomes obtained in our results included age, sex, surgical approach, tumor size, laterality, follow-up, blood loss, hospital stay, morbidity and mortality and the final histopathology results. For all variables, data were collected retrospectively from our hospital recording system. The cut-off value for post-operative follow-up was 30 days for benign adrenal lesions. However, in cases of adrenocortical malignancy, prolonged follow-up was indicated. All data were collected in an Excel sheet (Microsoft Office 2010) and the required outcomes were obtained.
During the period from April 2011 to March 2021, 88 patients underwent adrenalectomy. The patients' mean age was 56.653 ± 14.28 years. 35 of patients were males (39.77%) and 53 were female (60.23%), (Table 1).
Table 1: Patient demographics. View Table 1
The most common approach in our study was laparoscopic lateral trans-peritoneal adrenalectomy. All patients had general anesthesia with endotracheal intubation in supine position, which then changed to the left lateral position or right lateral position. In case of left adrenalectomy, three trocars were sufficient; however, an additional trocar was required in case of right adrenalectomy for liver retraction. Accessory ports sometimes were required especially in obese patients and in case of intra-abdominal extensive fibrosis. The first step was to ligate the renal vein to control any hormonal overexpression during tumor mobilization and to avoid avulsion of the short adrenal vein. Careful ligation and division of adrenal artery branches were performed. After ensuring adequate hemostasis, the resected adrenal tumors were removed from the abdominal cavity through one of the trocars ports. Open radical adrenalectomy was performed in case of adrenal malignancy using subcostal incision. Intraabdominal drain was not frequently used. 79 patients underwent complete laparoscopic adrenalectomy, five patients underwent laparotomy for pre-operatively diagnosed malignant adrenal mass, and four cases were converted to open.36 patients underwent right adrenalectomy, 49 with left adrenalectomy and three underwent bilateral adrenalectomy for pituitary Cushing. Average tumor size was 5.36 ± 3.95 cm. The mean operative time was 160.78 ± 53.47 min for the laparoscopic group, and 215.13 ± 56.19 min for the open group. The average blood loss was 49.5 ± 19.49 ml for the laparoscopic group and 74.5 ± 25.12 ml for patients who had open adrenalectomy.
The mean hospital stay was 4.15 ± 3.6 days for the laparoscopic group. In the open group, the average hospital stay was 9.66 ± 9.31 days; four patients in this group a had hospital stay longer than 10 days; two of them were diagnosed as adrenal carcinoma and underwent radical adrenalectomy, one diagnosed as large B-cell lymphoma and underwent radical adrenalectomy and one adrenalectomy in a patient who was on warfarin (Table 2).
Table 2: Comparison of operative outcomes between laparoscopic and open surgery. View Table 2
20 patients (22.7%) were diagnosed as non functioning adenoma on clinical/laboratory evaluation; six of them who were hormonally silent and were diagnosed as sub-clinical Cushing, as suggested by the improvement of the general condition postoperatively. 20 patients (22.7%) were diagnosed as functional adrenal adenomas; five of them were diagnosed as Conn's syndrome by pre-operative elevated Aldosterone level +/- hypertension and hypokalemia, 15 patients were diagnosed as cortisol-producing adenoma as proven pre-operatively by high blood pressure and high plasma cortisol levels (Figure 1A and Figure 1B). Three patients were diagnosed as pituitary Cushing and underwent bilateral adrenalectomy. A total of 26 patients was diagnosed as pheochromocytoma as proven by the clinical pictures and increase in the plasma Normetadrenaline and Metadrenaline levels. Five patients were diagnosed as adrenocortical carcinoma and underwent radical adrenalectomy; all the five cancers were left sided (Figure 1C). Four patients were diagnosed as metastatic renal cell carcinoma, three were left sided and one was right sided (Figure 1D).
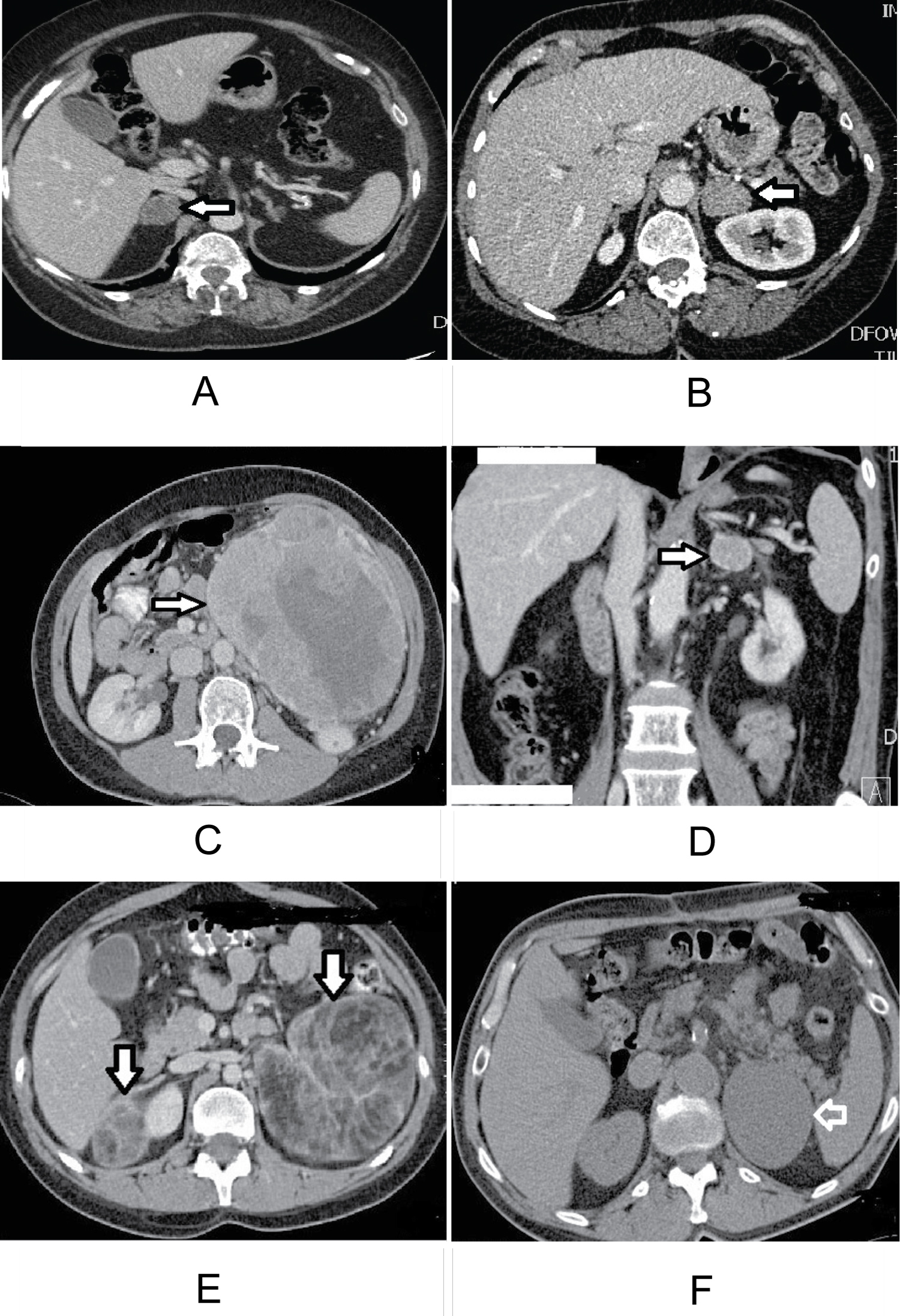 Figure 1: MSCT abdomen showing (a) Bilateral myolipoma; left 10 × 11 cm, right 4.6 × 3.3 cm; (B) Left adrenal epithelial lined cyst 6.3 × 7.7 cm; (C) Left adrenal metastatic mass, 3 × 2.8 cm; (D) Left adrenocortical adenoma, 30 mm; (E) Left adrenocortical carcinoma 16.8 cm; (F) Right adrenal adenoma 2.8 cm × 2.2 cm.
View Figure 1
Figure 1: MSCT abdomen showing (a) Bilateral myolipoma; left 10 × 11 cm, right 4.6 × 3.3 cm; (B) Left adrenal epithelial lined cyst 6.3 × 7.7 cm; (C) Left adrenal metastatic mass, 3 × 2.8 cm; (D) Left adrenocortical adenoma, 30 mm; (E) Left adrenocortical carcinoma 16.8 cm; (F) Right adrenal adenoma 2.8 cm × 2.2 cm.
View Figure 1
Two patients were diagnosed as B-cell lymphoma; one underwent right adrenalectomy, and one underwent left radical adrenalectomy. One case was consistent with lung metastasis, and one had a metastatic melanoma. Other cases were diagnosed as cavernous hemangioma, myelolipoma, pseudocyst, true cyst, and two post-operative inflammatory reactions (Figure 1E and Figure 1F), (Table 3).
Table 3: Final histopathology diagnosis. View Table 3
We used the cut-off value of 30 days of follow-up for benign adrenal lesions, while patients with adrenal malignancy have been followed-up for at least 2 years. Post-operative complications included one patient who developed an incisional hernia after radical adrenalectomy, two patients developed collection; one was on warfarin and developed subcutaneous collection and cellulitis, the other one developed intra-abdominal collection at the adrenal bed. Two patients developed chest infection. Two patients developed a recurrence of the malignancy within two years after surgery. One mortality was reported in this study due to an advanced malignancy during the operation (Table 4).
Table 4: Post-operative complications. View Table 4
Over the last few decades, mini-invasive adrenalectomy has been introduced as an alternative to the conventional open technique. Since the first laparoscopic adrenalectomy performed by Gagnerin [3], Several subsequent studies have proven the safety and feasibility of laparoscopic surgery compared with open surgery, including shorter hospital stay, faster recovery, decreased postoperative pain, lower incidence of complications, and lower morbidity and mortality rates [4,5]. Laparoscopic/robotic adrenalectomy is now considered the standard treatment for small adrenal lesions (< 8 cm) [6]. In selected cases, LA has also been used in the management of small (< 5 cm) malignant adrenal carcinomas [7]. Open adrenalectomy is associated with slightly higher mortality (2%-4%) and morbidity rates, including bleeding, pain, pulmonary and cardiac complications, and wound infections. Thus, open adrenalectomy is reserved for large tumors (> 6 cm) and primary malignancies [8,9]. However, diagnostic laparoscopy has been tried in our study in some cases of suspected malignancy to exclude widespread tumor metastasis in the abdominal cavity to avoid any unnecessary major intervention in an advanced malignancy. Nevertheless, there is no general agreement regarding the best surgical approach [10].
A systemic approach has been followed in our patients. A detailed history and clinical examination have been conducted. Based on the clinical picture, the appropriate biochemical screen for a functioning adrenal tumor was performed. This usually includes plasma electrolytes, renal function tests, low-dose dexamethasone suppression test, plasma cortisol levels, plasma ACTH and 24 h free urinary for the diagnosis of cortisol-producing tumors, measurements of metanephrines and fracted catecholamines in the urine and plasma for catecholamine-producing tumor diagnosis, measurement of the plasma concentration of aldosterone, renin plasma activity and renin to Aldosterone ratio for the diagnosis of Aldosterone-producing tumors, measurement of sex hormones and a 21-hydroxylase level for Androgen and estrogen producing tumors. Radiological evaluation included computed tomography (CT), magnetic resonance imaging (MRI), or ultrasonography. All cases were discussed in an endocrine multidisciplinary team including endocrinologists, endocrine surgeons, radiologist, pathologist and anesthesiologists. Pre-operative management included a correction of any electrolyte disturbance, control of hypertension and medical control of pheochromocytoma symptoms by α and β blockers.
One of the most important factors in considering surgery for adrenal lesions is to determine whether the tumor is functioning or not, according to the guidelines of the (AACE) and (AAES) [11]. If the tumor is proved to be functional after hormonal work-up, surgery is considered. Surgery is generally not recommended for non functional adrenal tumors; however, we considered surgery in our study for 20 patients with negative hormonal work-up; six patients of them had subclinical adrenal tumor as indicated by the clinical picture, and 14 had a significant increase in the size of the adrenal lesion on radiological follow-up. Surgery was considered in other patients with negative hormonal work-up, either due to an increase in the size of the tumor on follow-up or indeterminate appearance of the tumor on the scan.
Tumor size is one of the important factors to be considered before laparoscopic surgery. Although most surgeons may use the cut off value of 5 or 6 cm for laparoscopic adrenalectomy, Mac Gilliv Ray and Henry reported safe laparoscopic adrenalectomy with tumor up to 12 cm [12,13]. Although laparoscopic adrenalectomy may be not optimal with large tumors because of the increased risk of malignancy, difficult dissection and time consumption; however, we proved in our study that laparoscopic adrenalectomy is safe and reasonable even with large glands > 12 cm. Nevertheless, open surgery is still recommended whenever adrenal carcinoma is suspected or confirmed. Due to the aggressive nature of adrenal tumors, open surgery is sensible for en-bloc resection [14]. In general, there is no universal endorsement regarding the best surgical approach, as many studies have proven equivalent results for open adrenalectomy compared to laparoscopic adrenalectomy [15].
The mean operative time in our study was 160 min for the laparoscopic group. Other studies have reported operating times ranging between 100 and 202 min [16,17]. However, in our study we found significant reduction in operative time after the 1st twenty patients due to improvement in the learning curve. The mean operative time in patients who had open adrenalectomy was 215 min; however, these patients had open surgery mainly due to hugely enlarged glands or suspected malignancy, so prolonged and excessive dissection was expected. Average blood loss was less than 50 ml. Nevertheless, we found that open radical adrenalectomy was associated with more blood loss than laparoscopic adrenalectomy. The mean hospital stay was 4 days for patients who had laparoscopic adrenalectomy. Other studies have reported a mean hospital stay of less than three days [18]. In the open adrenalectomy group, the mean hospital stay was 9 days. Again, excessive dissection for large/malignant adrenals in the open group has contributed to the prolonged hospitalization. Four patients (4.5%) needed conversion to open adrenalectomy. Difficulty to control bleeding, extensive adhesions or injury to nearby structures were the mean reasons for conversion to open. Gagner M, et al. and Brunaud L, et al. also reported conversion rate of 3%-6% [19,20]. The main intra and post-operative complications included abdominal collection in two patients, chest infection in two patients, two patients with recurrence after one year who had adrenocortical carcinoma, and one patient developed incisional hernia after radical adrenalectomy. One mortality was reported because of an advanced tumor, and four patients needed conversion to open. Other studies have also reported complication rate of 9.5% [21].
On the other side, we have some limitations in our study. First, the total number of patients included in the study was small which could affect the general contribution of the current study to the literature. Secondly, our main objective was to evaluate our general surgeon experience in adrenalectomy. Additionally, we compared the outcomes between open and laparoscopic adrenalectomy; however, the population in both groups was not identical in characteristics or diagnosis, which may form a source of bias in our comparative analysis between both groups.
Pathological conditions affecting the adrenal gland range from benign conditions to highly aggressive tumors. An accurate pre-operative assessment is essential for selection of eligible patients for surgery. We found that the ongoing development in the learning curve in our study was associated with significant improvement in the clinical outcomes. Although adrenalectomy can be done by either open or mini-invasive techniques, we can report that laparoscopic adrenalectomy is associated with betters outcomes including less post-operative pain, shorter hospital stays, less overall costs, and decreased morbidity.
Not applicable.
None.
None.