Maridi county hospital faces a critical shortage of space and staff, and this study is intended to evaluate the possibility of introducing telephone calls to replace face-to-face postoperative clinic visits. We were looking at new ways of how the surgical team can decongest the physical postoperative clinic, so that they can have adequate time to assess new patients on clinic days.
A structured questionnaire was administered to postoperative patients who consented to the study and the data was analyzed using Stata 13.0.
The mean age was 38.9 years with an equal number of male and female participants. Hernias and chronic appendicitis were the commonest pathologies noted with herniorrhaphy and appendectomy being the main procedures performed. Out of 120 participants, 56 (46.7%) had access to a telephone that they owned. 88.3% of the study participants said they would prefer a face-to-face postoperative clinic follow up compared to only 11.7% who preferred postoperative follow up by telephone call.
Many patients find face-to-face postoperative clinic visits more convenient than the possibility of using a telephone call. Amidst this unexpected finding, the surgical team is looking at conducting another study comparing the traditional face-to-face and the use of a telephone call for postoperative follow up, with particular focus on patient satisfaction, health outcomes and financial savings.
Face-to-face, Postoperative, Telephone call
OBGY: Obstetrics and Gynecology; USA: United States of America
Access to surgical care is still a big challenge in many low- and middle-income countries. Sub Saharan Africa is no exception with enormous deficits in human resource and infrastructure [1-3]. Postoperative clinic visits following discharge forms an integral part of this surgical care. Maridi county hospital, located in Western Equatoria State, South Sudan currently has one general surgeon who provides both general surgical and obstetrics and gynecology (OBGY) surgical services. Consults to the general surgery service, OBGY and medical clinic are currently combined for one clinic day every week. This clinic is run by the general surgeon, assisted by one general practitioner (medical doctor) depending on his/her availability plus a nurse aide. Our facility has a critical shortage of space and staff as well as limited clinic hours.
In 2019, Maridi county hospital served 55,000 patients with outpatient visits averaging 80 patients per day. Due to the limited space and staff shortage, the surgery department is looking at ways of decongesting the face-to-face clinic attendance by use of telemedicine, specifically use of the mobile telephone for phone calls. We are looking at the use of a phone call for routine postoperative follow-up visits, which is usually a brief encounter with the doctor, lasting about 10 minutes. In the traditional face-to-face encounter, patients and care givers have to cover transport costs and miss work time to attend postoperative clinics, and doctors lose valuable time to assess new patients when attending to postoperative cases [4,5].
Studies done in high income countries, where access to the mobile phone is wide spread show that telemedicine usage for postoperative review provided significant convenience and financial benefits to the patient and health facility [4,6-8]. McVay, et al. in Arkansas, USA found 90% of families contacted on phone were satisfied and did not request face-to-face appointment [9]. Others found using telemedicine to deliver health care in remote areas saved travel time and costs [6].
To date, no study has been done to evaluate patient preferred choice of follow up in sub-Saharan Africa. Furthermore, we wanted to evaluate access to mobile technology to gauge feasibility of an upcoming study on the use of mobile phone call as an alternative to face-to-face postoperative visits.
Institutional approval was received to conduct the survey on patients who presented to the general surgery ward and underwent a surgical procedure. Patients who consented to be part of the survey were given a structured questionnaire before discharge. The questionnaire was administered by a member of the nursing staff or one of the doctors and specific data collected included demographics, whether the patient or caregiver had access to a mobile phone, the preferred method of follow up, means of transport to the hospital, among others (Appendix 1).
Completed questionnaires were entered into a computer using Epidata. The data was then exported to Stata 13.0 for analysis. Data was summarized into means and standard deviations for normally distributed data and inter quartile range and median for skewed data. Categorical data was presented inform of frequencies and percentages. The results were presented in form of tables and figures.
Majority (44.2%) of the participants were aged between 31 to 45 years, the mean age was 38.9. Equal number of male and female patients participated in this survey. The results are summarized in Table 1.
Table 1: Table showing social demographic characteristics of 120 study participants. View Table 1
The most common (18.3%) diagnosis was right inguinal hernia while herniorrhaphy was the most common (59.2%) surgical procedure. The results are summarized in Table 2.
Table 2: Surgical diagnosis and procedure among study participants. View Table 2
Almost half (46.7%) of the participants owned a telephone while 35% had no access to a telephone at all. The results are summarized in Figure 1.
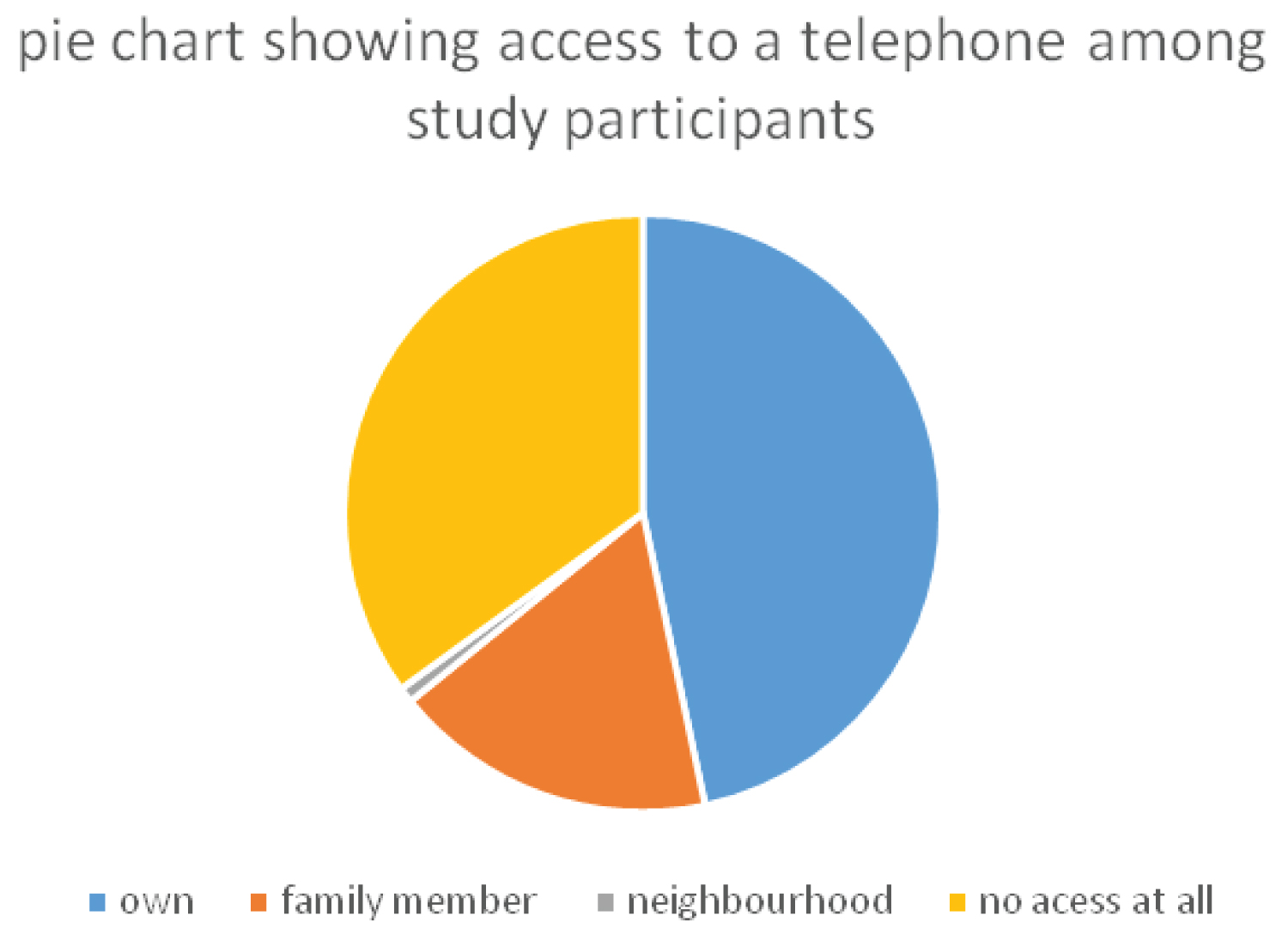 Figure 1: Pie chart showing access to a telephone among study participants.
View Figure 1
Figure 1: Pie chart showing access to a telephone among study participants.
View Figure 1
Majority (88.3%) of the study participants preferred face-to-face follow up. This is shown in the bar chart (Figure 2).
 Figure 2: A bar graph showing participant's preferred method of follow up.
View Figure 2
Figure 2: A bar graph showing participant's preferred method of follow up.
View Figure 2
As shown in the table below, majority (65%) of the participants were not willing to use the nearest health facility for postoperative review (Figure 3). The results are summarized in Table 3.
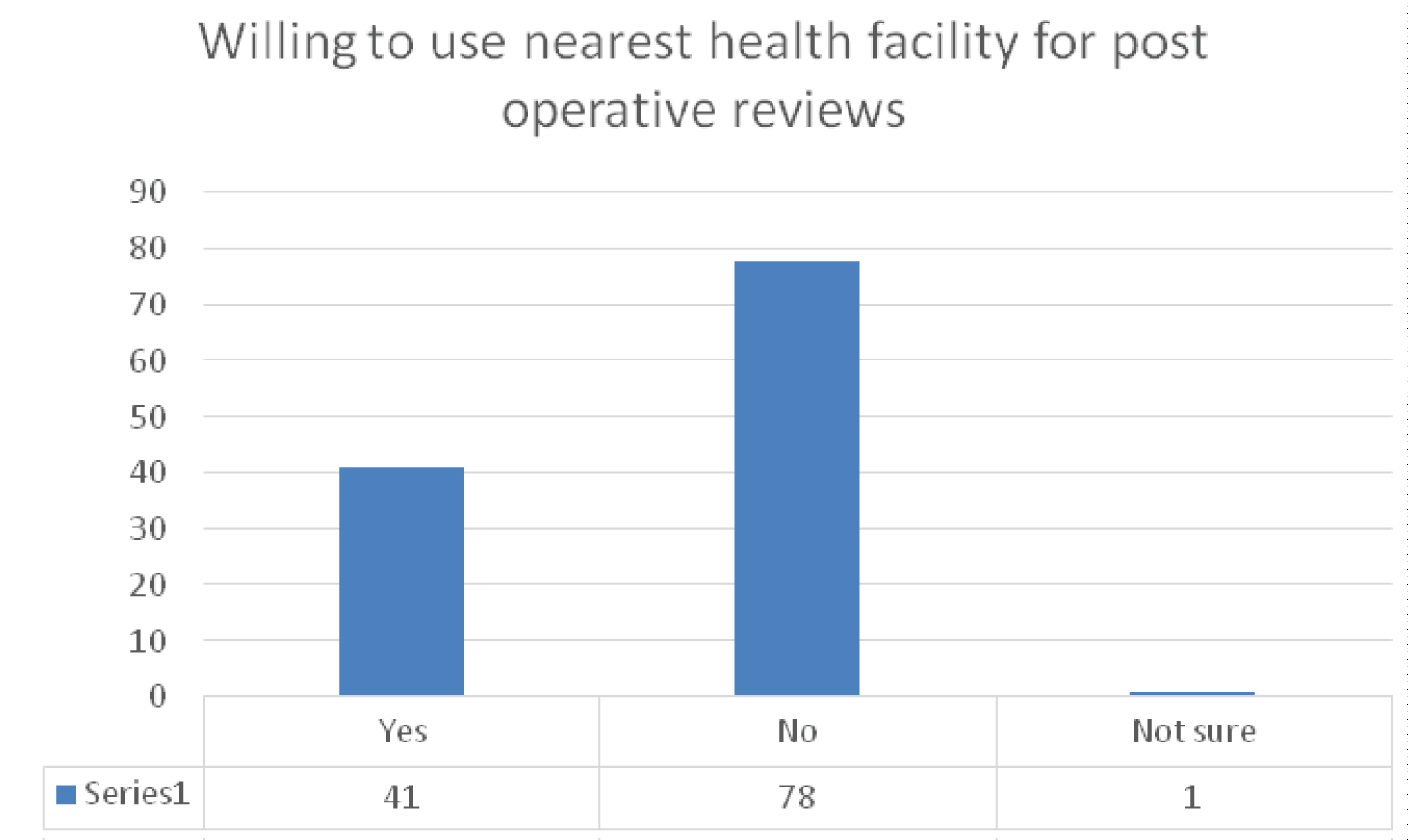 Figure 3: Figure showing participant willingness to use nearest facility for postoperative review.
View Figure 3
Figure 3: Figure showing participant willingness to use nearest facility for postoperative review.
View Figure 3
Table 3: Table showing participant's willingness to use nearest health facility for review. View Table 3
Most (56.7%) of the participants used boda boda as a form of transport, majority (75.8%) were < 6 miles from the hospital. The results are summarized in Table 4.
Table 4: Table showing participants access to the hospital. View Table 4
The need to improve access to surgical care in rural Africa cannot be overstated, and any intervention geared towards this is viewed with keen interest. This is believed to be the first study that investigates patient preference with regards to postoperative follow-up care.
The survey revealed that 47% of the study participants had access to a mobile phone that they owned and a further 18% had access through a family member. However, only 12% of the respondents wanted their postoperative reviews conducted through a mobile phone call. This greatly contrasts to the 98% of the patients in Pennsylvania who opted for telephone postoperative visits [10]. This may be because the network connection provided by the current two service providers is unstable and occasionally the service is unavailable. Other reasons why most participants preferred face-to-face approach could be because they cannot afford to buy mobile phones. Furthermore, this approach to postoperative follow-up being new to the local population may be a victim of mistrust thus explaining why 88% preferred the traditional face-to-face review.
Participants were also asked if they were willing to use any of the nearest lower-level health facilities other than the hospital where the surgery was done. Many of them (65%) did not want to use the nearest lower-level health facilities with the main reason being inadequate services in these facilities. Other reasons reported were that the hospital was the nearest health facility to them, and absence of a doctor. This sentiment resonates with the ever-present challenge of inadequate qualified cadres across the healthcare systems in Africa [3,11].
We also wanted to find out how patients accessed the hospital in terms of need for care giver to accompany them, transport means, cost per single trip and mileage covered to reach the hospital. Significant to note is that majority of the respondents lived less than 6 miles from the hospital. This may explain why 37.5% of the study participants were able to walk to the hospital to access Medicare. This finding is in contrast to most studies where telemedicine was used and the average distance covered was way greater than six miles [6,12]. Telephone call may ease the burden on caregivers, as 65% of our patients required to be accompanied to the hospital for their follow-up visits. Our findings that 100 out of 120 participants felt they needed a postoperative review emphasizes the need for patient follow-up upon discharge. This follow-up forms an integral and critical component of continuity of surgical care and patient satisfaction.
Most of our respondents preferred the traditional face-to-face approach for their postoperative clinic visits. This puts the surgical team at Maridi county hospital in a dilemma since the team was looking at introducing the use of telephone calls to follow up patients who had undergone basic surgical procedures like herniorrhaphy and appendectomy. Nonetheless, we recommend a study that will look at the two arms of telephone call versus traditional face-to-face review comparing patient satisfaction, health outcomes and financial savings. This will help the team decide on whether to introduce telephone calls for postoperative reviews or stick to the well-known face-to-face approach.
We thank Dr. Mazzin Adil Severino, Dr. Mungumwa Wetemwami Thierry, theatre and surgical nursing staff of Maridi County Hospital.
None declared.
None.