Acute appendicitis secondary to gastrointestinal Kaposi sarcoma is a rare but critical manifestation of this condition. An acute abdomen in patients with HIV-AIDS can be secondary to Kaposi sarcoma with appendiceal involvement. The timely identification of other clinical manifestations of pathologies associated with immunosuppression can lead to a promptly diagnosis. Regardless of the management of the underlying pathology, the treatment of choice for acute appendicitis is surgical.
Acute appendicitis, Kaposi's sarcoma, Acute abdomen, HIV-AIDS
Kaposi's sarcoma is the most frequent malignancy in patients with HIV-AIDS (60%) and currently the most common variety is that associated with AIDS. Its presence suggests immunocompromise and associates a poor prognosis if timely antiretroviral treatment is not instituted [1,2].
Kaposi's sarcoma is defined as a low-grade vascular tumor associated with Human Herpes Virus 8 (HHV-8) and immunosuppression in the context of inflammation and angioproliferation [1-5]. The lesions are nodular or flat, and may present on the skin, mucous membranes and internal organs including lymph nodes, however they can also present in the respiratory and gastrointestinal tracts [2-4].
Abdominal pain that prompts medical attention occurs in 12 to 45% of patients with HIV infection, and only 11% has an aetiology associated with AIDS; among these causes are acute appendicitis, which comprises 30% AIDS's patients [6].
The prevalence of acute appendicitis in the general population is 0.1%, while in HIV-AIDS patients it is 0.6-3.6%. Some of the causes described in acute appendicitis with HIV-AIDS are fecalith, lymphoid hyperplasia, CMV infection, mycobacterial infection, and Kaposi sarcoma [6,7].
The gastrointestinal involvement of Kaposi sarcoma has been reported in up to 40% of patients; an atypical presentation of this includes appendiceal, rectal and mesenteric involvement. The association between acute appendicitis and visceral Kaposi sarcoma is rare, it's a unique case of acute abdomen in patients with HIV-AIDS with few cases registered in the international literature, most generally in the context of multicentric or metastatic disease [1-4].
Until 2011, only 6 cases of appendiceal kaposi have been reported in the English medical literature [2].
The pathophysiology of this entity corresponds to the basic principle for the development of acute appendicitis, which is the progressive obstruction and obliteration of the appendicular lumen, in this case due to the visceral involvement of sarcoma [2].
Some of the most common clinical manifestations of gastrointestinal Kaposi's sarcoma are extensive skin lesions with visceral involvement, gastrointestinal manifestations such as gastrointestinal bleeding, abdominal pain, nausea, vomiting, malabsorption, intussusception, weight loss, intestinal obstruction, and diarrhea. When this is associated with appendiceal involvement it has been reported fever, nausea, vomiting, anorexia, right lower quadrant pain and tenderness. Alterations in laboratory studies such as leukocytosis with bandemia, leukopenia or normal WBC or with low levels, have been described in these patients [2,6].
A screening method for gastrointestinal Kaposi sarcoma is the fecal occult blood test (based on the vascular pathophysiology of the lesion) [1]. Occasionally, as part of the gastrointestinal bleeding study protocol, endoscopic studies are performed identifying the injuries [2].
A 19-year-old male presented to the ED with a 48-hours history of abdominal pain associated with fever, anorexia, nausea, and vomiting. He reported diffuse periumbilical abdominal pain, with subsequent migration to the lower right quadrant. As a relevant antecedent, he presented slightly elevated, bluish-violaceous skin lesions on the trunk and extremities of months of evolution, previously treated without improvement (Figure 1). The patient did not refer to any other medical or surgical history to direct questioning.
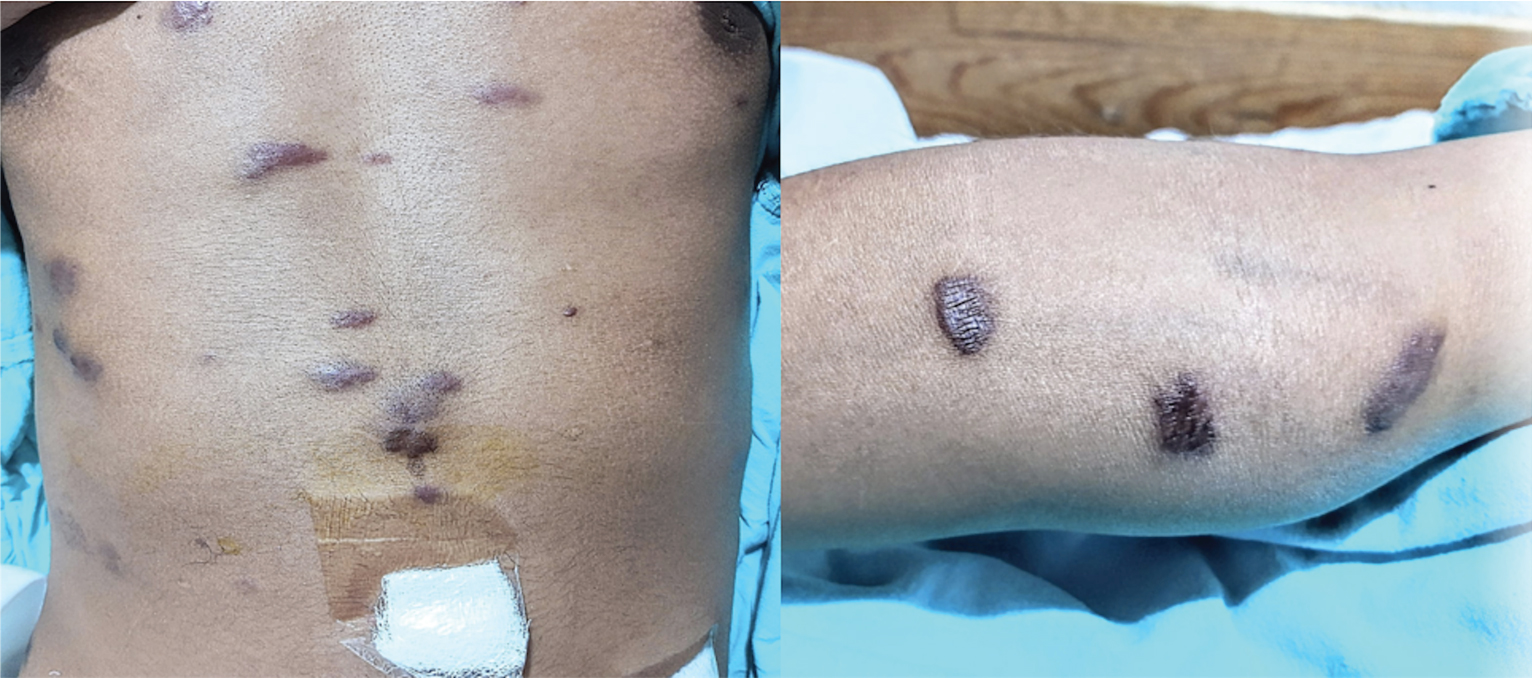 Figure 1: Slightly raised, bluish-violaceous skin lesions on trunk and limbs.
View Figure 1
Figure 1: Slightly raised, bluish-violaceous skin lesions on trunk and limbs.
View Figure 1
Upon admission, he presented fever (> 38.5 °C) and tachycardia of 110 bpm; the rest of vital signs were within normal parameters. Abdominal examination revealed deep and superficial tenderness at the level of the right iliac fossa, rebound and peritoneal irritation. In laboratory studies, leukocytosis of 15,000 cells/ml with a left shift (85% neutrophils) was reported. Imaging studies were performed; a simple abdominal X-ray showed psoas sign, with no evidence of free air in the cavity nor localized ileus. The diagnosis of acute appendicitis was reached with an Alvarado score of 10 points and RIPASA of 16 points.
The patient underwent a laparoscopic appendectomy; the diagnostic laparoscopy revealed red-violaceous nodular lesions in localized areas of the small intestine and mesentery (Figure 2), as well as a cecal appendix. We observed Inflamed and erythematous 45 × 20 mm lesions, covered with a thin layer of fibrino-purulent exudate (Figure 3), and a violaceous nodule at the base of the appendix and in the mesoappendix (Figure 4). The appendectomy was completed and the surgical specimen was sent to histopathological study. The patient was discharged with complete recovery on the third postoperative day. The pathology report stated: "In the histological sections analyzed, a cecal appendix is observed showing mucosa with extensive ulceration, replaced by acute inflammatory infiltrate; In the lamina propia and submucosa, a neoplasm consisting of spindle cells with moderate pleomorphism, arranged in short fascicles immersed between the collagen glands and fibers, with multiple small, thin-walled, dilated vessels is identified. There are extravasated erythrocytes, hemosiderin deposits, and up to 5 mitoses in ten high-power fields. The muscularis propria with a prominent inflammatory infiltrate due to polymorphonuclear cells that extends to the serosa and the adipose tissue of the mesoappendix" (Figure 5). These findings are consistent with an Appendiceal Kaposi's sarcoma with superimposed acute appendicitis.
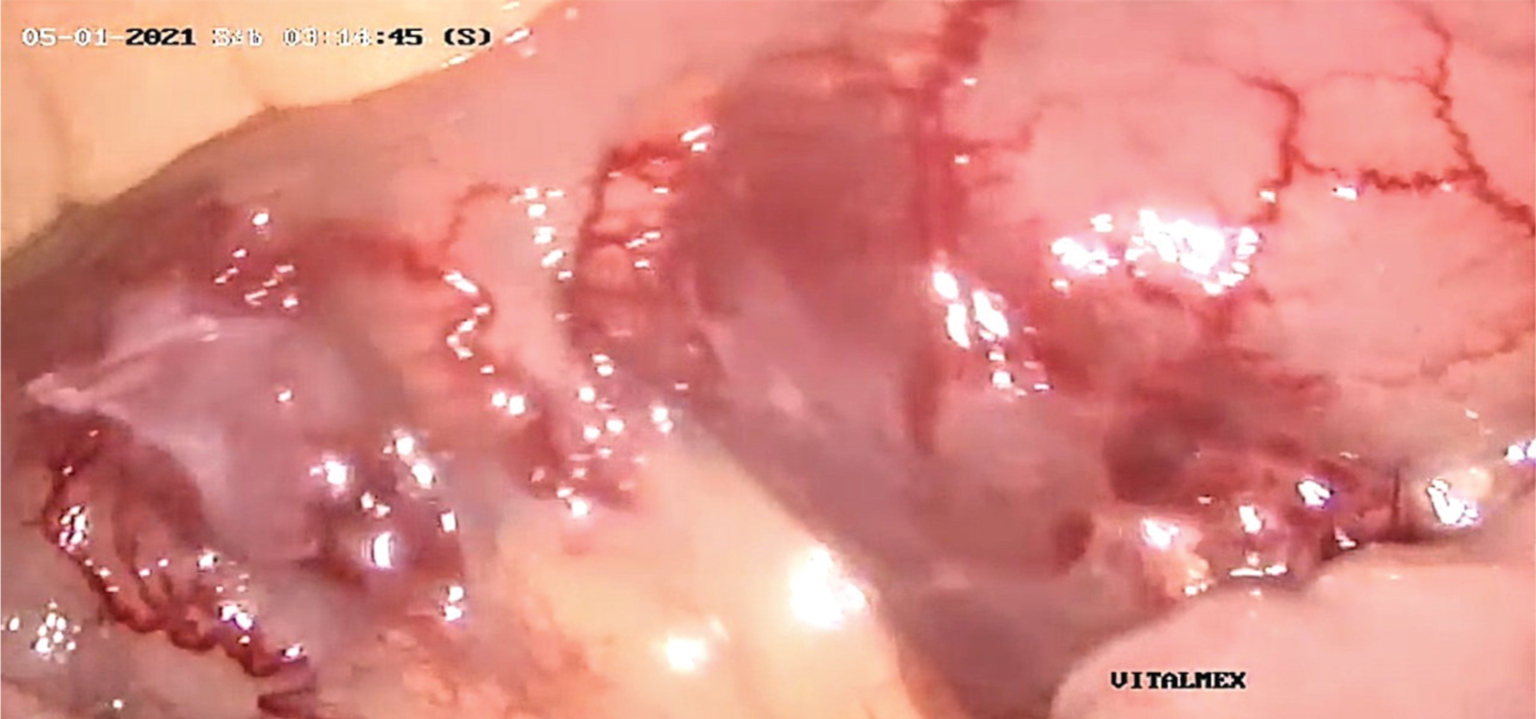 Figure 2: Nodular red-violaceous lesions in localized areas of the small bowel and mesentery.
View Figure 2
Figure 2: Nodular red-violaceous lesions in localized areas of the small bowel and mesentery.
View Figure 2
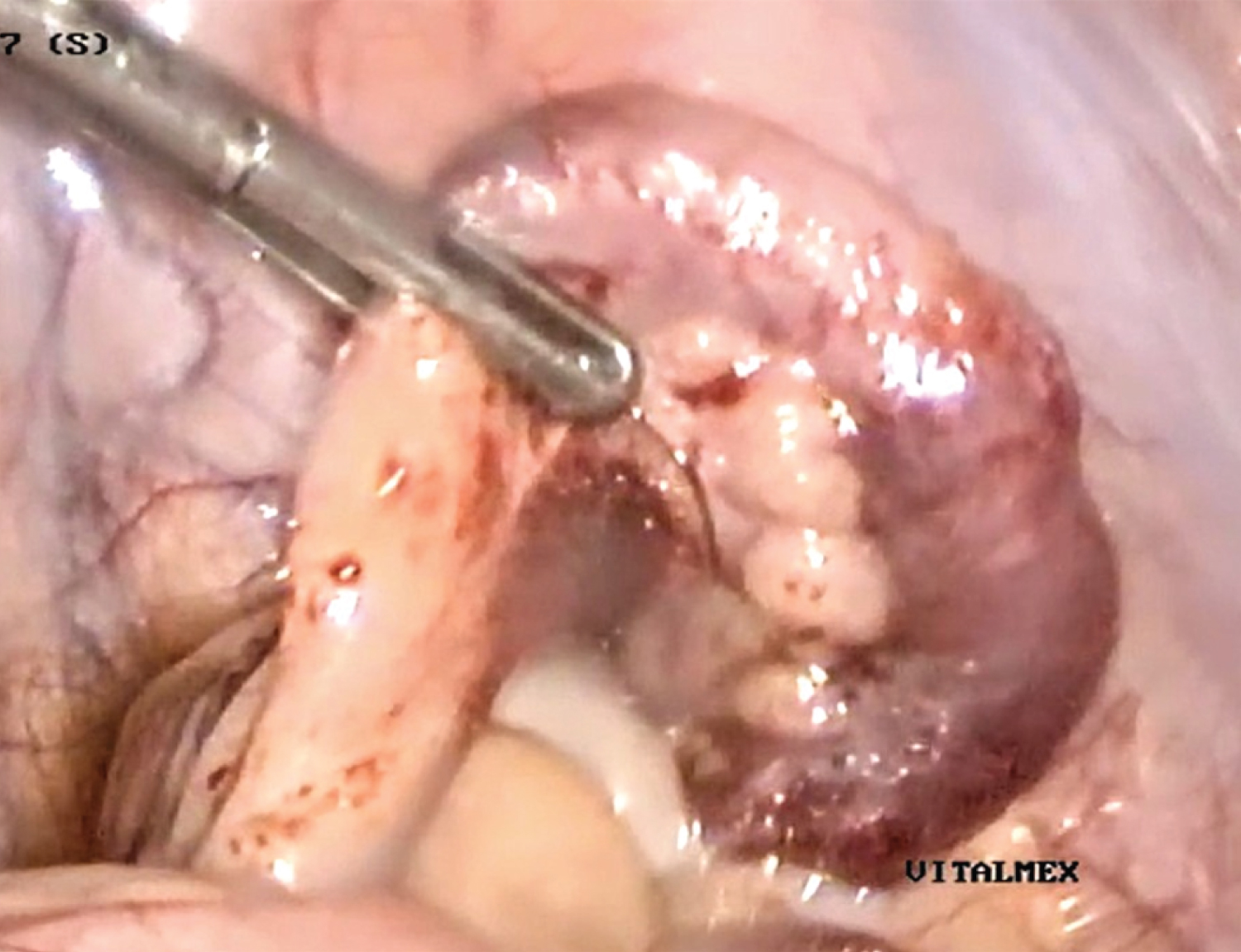 Figure 3: Swollen and erythematous cecal appendix measuring 45 × 20 mm, covered with a thin layer of fibrinous-purulent exudate.
View Figure 3
Figure 3: Swollen and erythematous cecal appendix measuring 45 × 20 mm, covered with a thin layer of fibrinous-purulent exudate.
View Figure 3
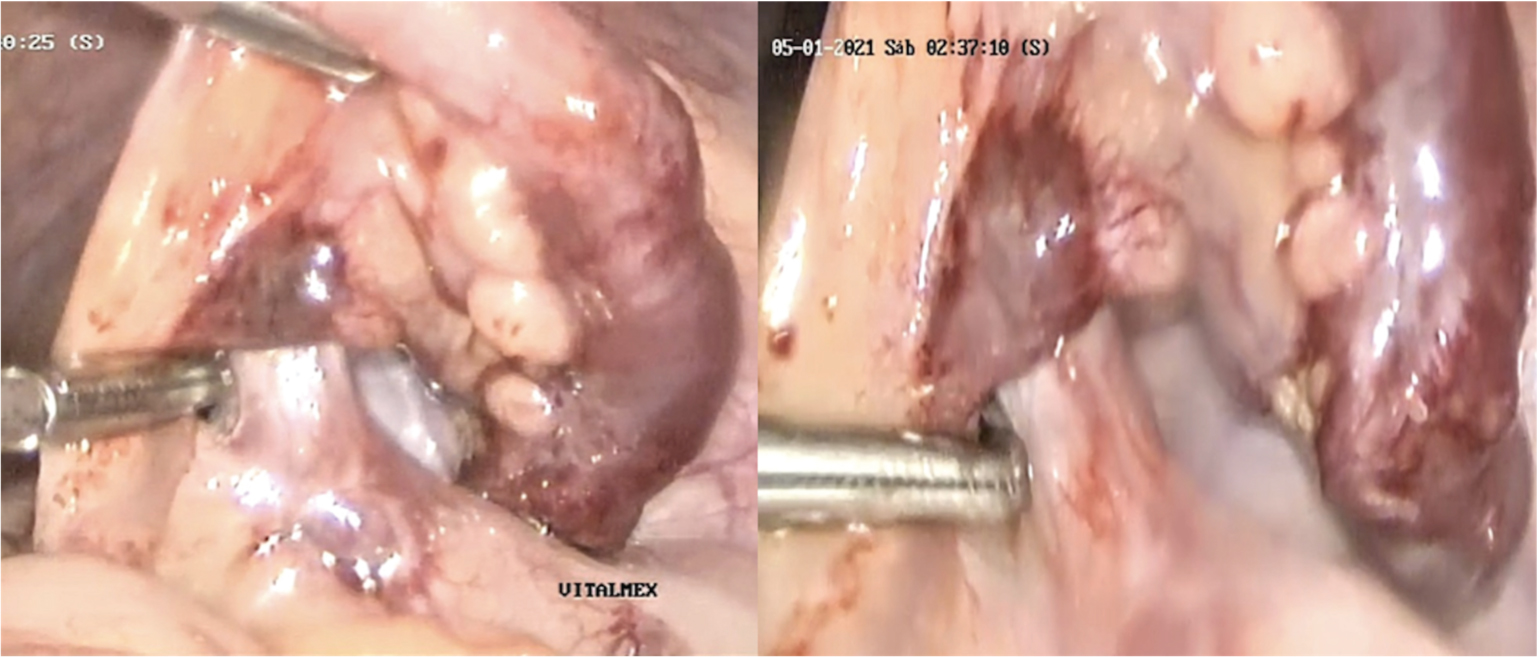 Figure 4: Violaceous nodule at the base of the appendix and the adjacent mesoappendix.
View Figure 4
Figure 4: Violaceous nodule at the base of the appendix and the adjacent mesoappendix.
View Figure 4
 Figure 5: a) Ulcerated mucosa, lamina propria with abundant dilated vessels associated with fascicles of spindle cells (10x); b) Spindle cell fascicles surrounding vascular canals with erythrocyte extravasation (40x); c) The cells present ample cytoplasm, an irregular ovoid nucleus, moderate atypia, and increased mitosis activity (40x).
View Figure 5
Figure 5: a) Ulcerated mucosa, lamina propria with abundant dilated vessels associated with fascicles of spindle cells (10x); b) Spindle cell fascicles surrounding vascular canals with erythrocyte extravasation (40x); c) The cells present ample cytoplasm, an irregular ovoid nucleus, moderate atypia, and increased mitosis activity (40x).
View Figure 5
Kaposi's sarcoma with visceral involvement is usually asymptomatic and diagnosed incidentally on endoscopy or autopsies. It occurs more frequently in advanced stages of HIV-AIDS, but it can manifest with a normal CD4 count [2].
Refeering to acute appendicitis in infected patients with AIDS, the classic clinical picture is generally absent and there are no signs or symptoms to guide the differential diagnosis, resulting in a delayed one [7,8]. Signs of peritoneal irritation may be completely absent, even in surgical emergency situations, and more than one condition may be present at the same time in immunocompromised patients [6,8].
The clinical picture described in most case reports is that of a male patient with a previous diagnosis of HIV-AIDS, or with risk factors for this infection, with poor adherence to antiretroviral treatment, as well as inadequate follow-up, a history of melena or gastrointestinal bleeding and a classic picture of acute appendicitis [1,2]. Visceral involvement generally precedes skin lesions [2].
Despite the fact that currently most patients are aware of their HIV infection status, an undiagnosed pathology associated with this infection may become apparent at the time of a surgical procedure [6].
In the majority of reported cases, less than half had skin manifestations and just over half the appendix was perforated in HIV positive patients [2].
Currently, the prevalence and severity of this entity has decreased thanks to adequate highly active antiretroviral therapy (HAART) [2,5].
The main approach to the management of Kaposi sarcoma is based on the prevention of the progression of the immunosuppressive state, through HAART therapy that improves the CD4 count and reduces the viral load, which can limit the extent of the lesions and even their regression [1]. The management of appendicitis is surgical, regardless of its etiology [2].
An acute abdomen in the context of HIV-AIDS patients may be secondary to appendicular Kaposi's sarcoma and should be considered as part of the differential diagnosis, even in the absence of other clinical manifestations of Kaposi's sarcoma. A high index of suspicion is required on the part of the surgeon before the diagnostic and therapeutic approach of patients with this infection, especially once AIDS has developed.
All the authors fulfilled the following functions:
• Substantial contributions to the conception or design of the work.
• Acquisition, analysis, and interpretation of data for the work.
• Drafting the work, revising it critically for important intellectual content.
• Final approval of the version to be published.
• Agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
The authors declared that this study has received no financial support.
The authors have no conflict of interest to declare.
This case report exempted from ethical approval.
We have a confirmation with patient for this case report.