Department of General Surgery, Sungai Buloh Hospital, Malaysia
Introduction
Follicular thyroid carcinoma is prevalent in the age group 40-60 years old and accounts for 10% of the types of thyroid cancers [1]. FTC has the propensity to spread via hematogenous route, mainly to the bones and lungs.
Case Presentation
A 95 years old man presented to a district hospital with left hip pain after a trivial fall from bed. He is able to walk without any abnormal gait post trauma.
X-ray pelvis was done-showed suspicious lesion over the left superior and inferior pubic rami.
CECT of neck, thorax and abdomen was subsequently done and showed expansile bone lytic lesion of left superior and inferior pubic rami extending into the obturator internus, obturator externus and pectineus muscle measuring 8 cm, with single peritoneal nodule at the left abdomen with mediastinal lymphadenopathy. A calcified left thyroid nodule measuring 0.7 cm was seen on the scan, with no retrosternal extension. He was then referred to our tertiary hospital under orthopaedics for further management. Orthopaedics team ordered a CT guided biopsy of the pelvic mass and turned out to be a metastatic follicular carcinoma of the thyroid (Immunohistochemistry-thyroglobulin+, CK7+, CK20-, TTF1+). He was then transferred to the General Surgical ward. Clinical examination of the skull and neck is unremarkable. He shows no features of hyperthyroidism nor hypothyroidism. Thyroid function test reveals euthyroidism. TSH: 1.41. He has no previous history of neck lumps. Ultrasound of his neck shows left calcified thyroid nodule measuring 0.9 cm by 0.5 cm with bilaterally normal sized thyroid gland, with no lymphadenopathy. We did a PET-CT scan to prepare the patient for suitability of RAI. PET-CT revealed increased uptake of FDG in the left superior and inferior pubic rami as well s the acetabulum with soft tissue component measuring 8.3 cm by 6.6 cm extending into the left obturator and pectineal muscles .Mild uptake was noted in the calcified nodule in the left thyroid measuring 1.1 cm by 1.7 cm. PET CT did not show increased uptake in the peritoneal nodule as previously seen in the CT (Figure 1, Figure 2, Figure 3 and Figure 4).
 Figure 1: The initial x-ray pelvis done at emergency department.
View Figure 1
Figure 1: The initial x-ray pelvis done at emergency department.
View Figure 1
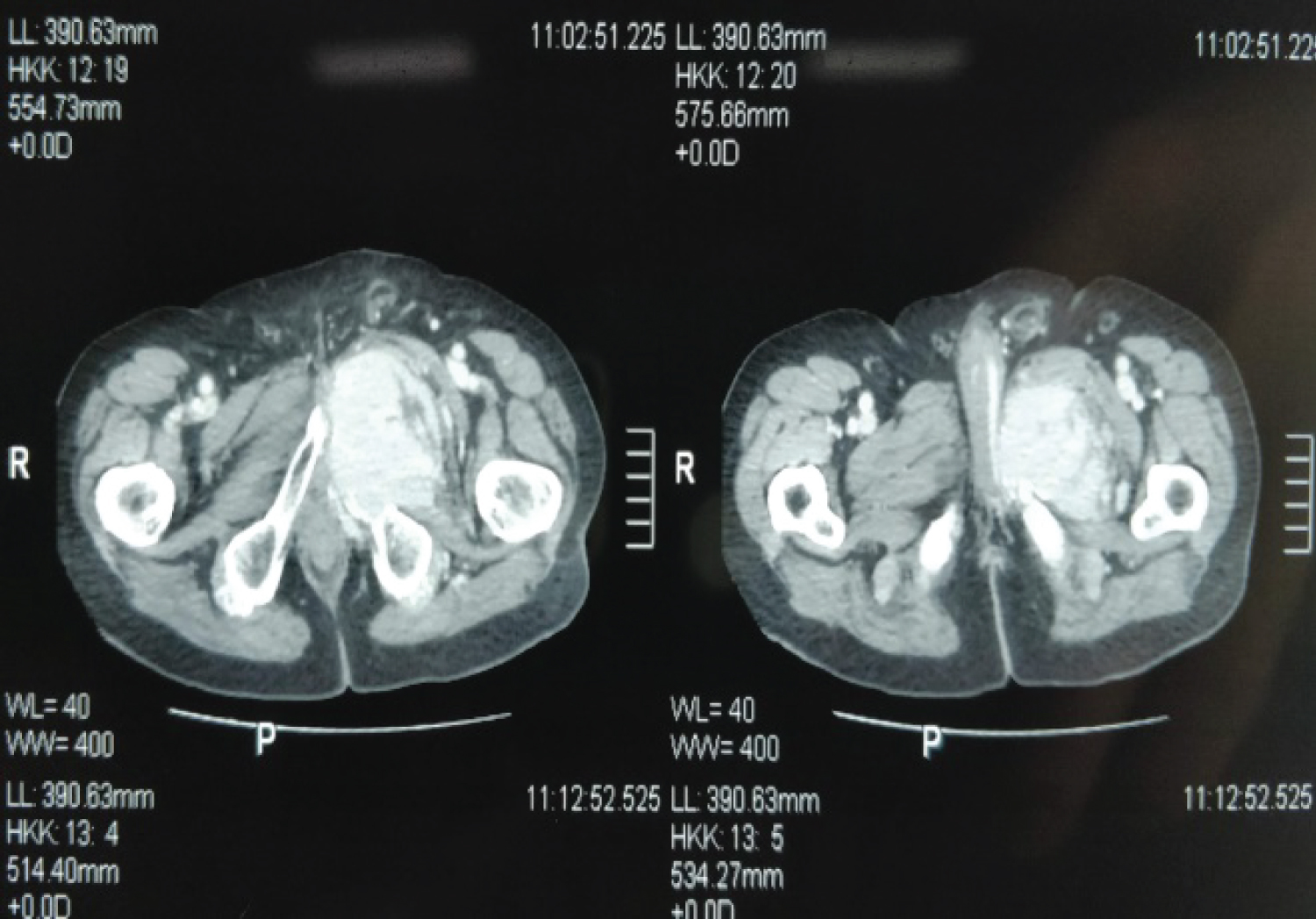 Figure 2: CECT reveals expansile bony lytic lesion in the left pelvis.
View Figure 2
Figure 2: CECT reveals expansile bony lytic lesion in the left pelvis.
View Figure 2
 Figure 3: No thyroid swelling seen or palpable clinically.
View Figure 3
Figure 3: No thyroid swelling seen or palpable clinically.
View Figure 3
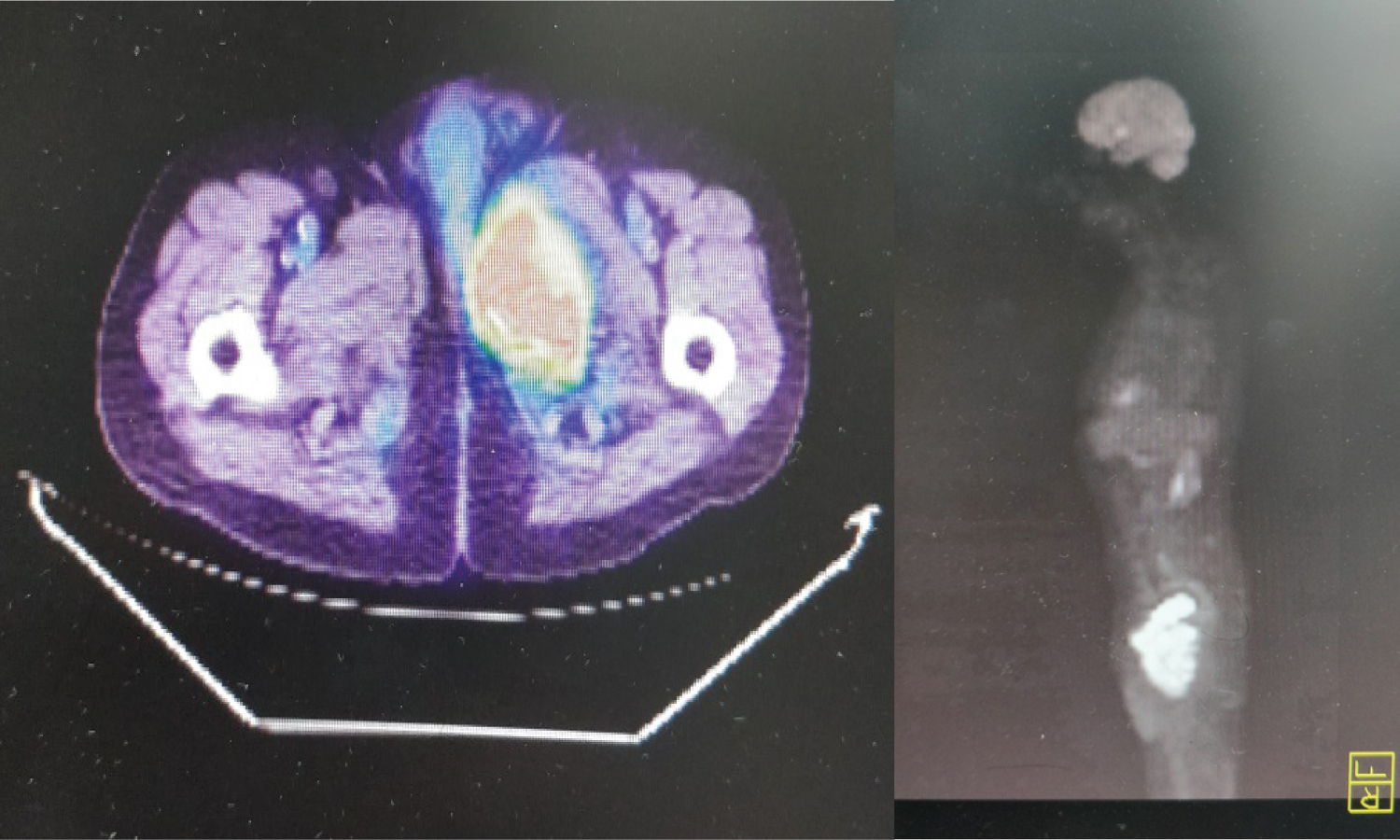 Figure 4: a) PET scan showed increase FDG uptake in the pelvic mass; b) PET scan showed increase FDG uptake in the pelvic mass.
View Figure 4
Figure 4: a) PET scan showed increase FDG uptake in the pelvic mass; b) PET scan showed increase FDG uptake in the pelvic mass.
View Figure 4
Discussion
Metastatic thyroid carcinoma usually presents with a clinically palpable neck lump. Retrospective case reports from Singapore which involved 732 patients of well differentiated thyroid carcinoma showed only 2.6% of the total patients present with metastasis as the sole initial feature. Out of the 2.6%, 10.5% were asymptomatic [2-7]. In this patient, he had no hip pain/compressive symptoms at all until he fell and sustained a pathological fracture.
In any patient presented with lytic bony lesions, the approach should be full body CT scan with concurrent biopsy to look for the primary, which was done in this patient. However the primary remains vague from CT scan-only a calcified 0.7 cm thyroid nodule, mediastinal lymphadenopathy and single peritoneal nodule is seen. A HPE sample was finally obtained via biopsy from the bone metastasis site. HPE is the golden standard for diagnosis of cancer of unknown primary, but due to the time consumption and the invasive nature, CT scan/PET-CT is a valuable tool for clinicians to detect and identify the primary site. But in this case, clearly HPE solved the mystery. The final AJCC classification of this case is T1aN0M1-stage IVc.
Competing Interest
None.
Patient Consent
Patient's consent was obtained for case report publication.
References
-
Sarani B, Strong M, Pascual J, Schwab C (2009) Necrotizing fasciitis: Current concepts and review of the literature. J Am Coll Surg 208: 279-288.
-
Khamnuan P, Chongruksut W, Jearwattanakanok K, Patumanond J, Yodluangfun S, et al. (2015) Necrotizing fasciitis: Risk factors of mortality. Risk Manag Healthc Policy 8: 1-7.
-
McHenry C, Piotrowski J, Petrinic D, Malangoni M (1995) Determinants of mortality for necrotizing soft-tissue infections. Ann Surg 221: 558-565.
-
Wong C, Chang H, Pasupathy S, Khin L, Tan J, et al. (2003) Necrotizing fasciitis: Clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am 85: 1454-1460.
-
Wong CH, Wang YS (2005) The diagnosis of necrotizing fasciitis. Curr Opin Infect Dis 18: 101-106.
-
Goh T, Goh L, Ang C, Wong C (2014) Early diagnosis of necrotizing fasciitis. Br J Surg 101: 119-125.
-
Miller L, Perdreau-Remington F, Rieg G, Mehdi S, Perlroth J, et al. (2005) Necrotizing fasciitis caused by community-associated methicillin-resistant Staphylococcus aureus in Los Angeles. N Eng J Med 352: 1445-1453.
-
Puvanendran R, Huey JC, Pasupathy S (2009) Necrotizing fasciitis. Can Fam Physician 55: 981-987.
-
Nordqvist G, Walldén A, Brorson H, Tham J (2015) Ten years of treating necrotizing fasciitis. Infect Dis 47: 319-325.
-
Khamnuan P, Chongruksut W, Jearwattanakanok K, Patumanond J, Tantraworasin A (2015) Necrotizing fasciitis: Epidemiology and clinical predictors for amputation. Int J Gen Med 8: 195-202.
-
Anaya DA, Dellinger EP (2007) Necrotizing soft-tissue infection: Diagnosis and management. Clin Infect Dis 44: 705-710.
-
Misiakos E, Bagias G, Patapis P, Sotiropoulos D, Kanavidis P, et al. (2014) Current concepts in the management of necrotizing fasciitis. Front Surg 1: 36.
-
Waldron C, Solon J, O'Gorman J, Humphreys H, Burke J, et al. (2015) Necrotizing fasciitis: The need for urgent surgical intervention and the impact of intravenous drug use. Surgeon 13: 194-199.
-
Sudarsky L, Laschinger J, Coppa G, Spencer F (1987) Improved results from a standardized approach in treating patients with necrotizing fasciitis. Ann Surg 206: 661-665.
-
Anaya DA, McMahon K, Nathens AB, Sullivan SR, Foy H, et al. (2005) Predictors of mortality and limb loss in necrotizing soft tissue infections. Arch Surg 140: 151-157
-
Sentochnik DE (1995) Deep soft-tissue infections in diabetic patients. Infect Dis Clin North Am 9: 53-64.
-
Hakkarainen TW, Kopari NM, Pham TN, Evans HL (2014) Necrotizing soft tissue infections: Review and current concepts in treatment, systems of care, and outcomes. Curr Probl Surg 51: 344-362.
-
Salcido R (2007) Necrotizing fasciitis: Reviewing the causes and treatment strategies. Adv Skin Wound Care 20: 288-293.
-
Lillian SK, Debbie FL, Samer NA, Todd SR, Samir SA, et al. (2011) Local variations in the epidemiology, microbiology, and outcome of necrotizing soft-tissue infections: a multicenter study. Am J Surg 202: 139-145.
-
Wong C, Khin L, Heng K, Tan K, Low C (2004) The LRINEC (laboratory risk indicator for necrotizing fasciitis) score: A tool for distinguishing necrotizing fasciitis from other soft-tissue infections. Crit Care Med 32: 1535-1541.
-
Keung E, Liu X, Nuzhad A, Adams C, Ashley S, et al. (2013) Immunocompromised status in patients with necrotizing soft-tissue infections. JAMA Surg 148: 419-426.
-
Paul RM, Joseph VS, Angela MM, Babak S, David DA Jr, et al. (2012) Hyperbaric oxygen therapy in necrotizing soft tissue infections. J Surg Res 177: 146-151.
-
Kobayashi L, Konstantinidis A, Shackelford S, Linda S Chan, Peep Talving, et al. (2011) Necrotizing soft tissue infections: Delayed surgical treatment is associated with increased number of surgical debridements and morbidity. J Trauma 71: 1400-1405.
-
Daniel NH, Angela MM, Brendan GC, Chris Wirtalla, Babak Sarani, et al. (2011) Transfer status: A risk factor for mortality in patients with necrotizing fasciitis. Surgery 150: 363-370.
-
Mills MK, Faraklas I, Davis C, Stoddard GJ, Saffle J (2010) Outcomes from treatment of necrotizing soft-tissue infections: Results from the National Surgical Quality Improvement Program database. Am J Surg 200: 790-796.
-
Timothy DL, Kent CC, Timothy AT, Dionne AS, Barbara AL, et al. (2010) Long-term outcomes of patients with necrotizing fasciitis. J Burn Care Res 31: 93-99.
-
Yuag Meng L, Chih Yu C, Mao Wang H, Chin Ming C, Wei Chih L, et al. (2005) Microbiology and factors affecting mortality in necrotizing fasciitis. J Microbiol Immunol Infect 38: 430-435.
-
Elliott DC, Kufera JA, Myers RA (1996) Necrotizing soft tissue infections. Risk factors for mortality and strategies for management. Ann Surg 224: 672-683.
Citation
Sheng KCK (2022) Occult Metastatic Follicular Thyroid Carcinoma-A Case of Unremarkable Clinical Neck Examination. Int J Surg Res Pract 9:143. doi.org/10.23937/2378-3397/1410143