Introduction: Reconstruction of the nose and cheek after oncologic resections or severe infections resulting in facial necrosis is challenging.
Sometimes different facial regions must be repaired, and different flaps must be used to achieve a good functional and aesthetic result. Local flaps and in cases of extensive defects, regional flaps are an excellent option for the reconstruction.
Objectives: To determine the efficacy and complications in the reconstruction of nasal pyramid and cheek soft tissue defects with local and regional flaps after oncological resections for malignant tumors and necrotizing facial infections.
Methods: A retrospective and descriptive study was carried out that included patients with defects in the nasal region and in the cheek caused by oncological resections for malignant tumors and necrotizing facial infections between the years 2000 and 2022.
Patients were grouped according to the location of the facial defect: Nose (reconstructed subunits) and cheek.
Skin defects on the cheek were considered small (< 3 cm), medium (> 3 cm and < 6 cm), and large (> 6 cm).
Results: 13 reconstructions were done,
In eight the reconstructions were of a single region of the face.
In 5 the reconstructions were made with more than one flap, due to facial defects that compromised the upper lip and nose and the cheek and nose.
In seven patients the nasal pyramid was reconstructed using different local flaps (nasogenian, midfrontal, nasal lateral wall) and in 5 the cheek was reconstructed using the Mustardé flap and the posterior trapezius musculocutaneous regional flap.
Conclusions: Reconstruction of the nasal pyramid and cheek with local and regional flaps was very effective, as it allowed to repair defects of moderate and large size, as well as to reconstruct complex defects that included different regions of the face and a multilayer reconstruction of the nose.
There was no partial or total necrosis of the flaps, and only one defect in the donor bed required delayed closure with a rotary flap. We believe that the use of these flaps continues to be the best option for reconstruction of these regions due to their excellent vascularization, reliability, and few complications.
Nasal and cheek reconstruction, Local and regional flaps, Squamous cell carcinoma
Cutaneous invasion of the facial region by the nasal cavity and paranasal sinuses tumors or necrotizing facial infections are uncommon. Skin involvement by basal cell or squamous cell carcinomas originating in the skin of the face is more common.
Repair of skin defects caused by oncological resections is challenging and often requires complex reconstructions.
Local flaps are an excellent option because they are within the surgical field, have very good irrigation, and because the same surgical team can perform the repair at the same time as the resection.
The posterior trapezius flap is very useful to repair extensive facial defects where the use of local flaps is insufficient.
To determine the efficacy and complications in the reconstruction of nasal pyramid and cheek soft tissue defects with local and regional flaps after oncological resections for malignant tumors and necrotizing facial infections.
A retrospective and descriptive study was carried out that included patients with defects in the nasal region and in the cheek caused by oncological resections for malignant tumors and necrotizing facial infections between the years 2000 and 2022.
The following data were recorded: Age, sex, histology and staging of tumors, type of facial infection, reconstructed nasal subunits, and size of the cheek defect after surgical resection, flaps used, reconstruction success (vitality of the flaps and ability to repair the defect), and complications.
Patients were grouped according to the location of the facial defect: Nose (reconstructed subunits) and cheek.
Skin defects on the cheek were considered small (< 3 cm), medium (> 3 cm and < 6 cm), and large (> 6 cm).
Patients with malignant rhinosinusal tumors were evaluated by nasal endoscopy, computed tomography and/or magnetic resonance imaging and computed tomography of the brain, neck, thorax, abdomen, and pelvis, or positron emission tomography (PET-CT).
In the oncological resections, free margins were obtained, confirmed by intraoperative biopsies and their deferred histological analysis.
In resections of tissue devitalized by infections, the margin was considered healthy when the facial tissue bled.
Eleven patients were treated, ten for malignant tumors and one for a necrotizing facial infection, which required reconstruction with local and regional flaps.
There were ten men and one woman, the average age was 75.53 years.
The location of the malignant tumors was the nasal cavity and paranasal sinuses (9/10) and the skin of the nose (1/10).
One patient had facial necrosis from a pseudomonas infection (ecthyma gangrenosum).
13 reconstructions were done (one patient had a recurrence post maxillectomy and reconstruction and needed a new excision with another reconstruction two years later and another had a recurrence 16 months after a rhinectomy, for which a new excision of the tumor and another reconstruction was performed).
In eight the reconstructions were of a single region of the face.
In 5, reconstructions were made with more than one flap, due to facial defects that compromised the upper lip and nose (2/13), and the cheek and nose (3/13).
In one patient the nasal ala was reconstructed with a nasogenian flap and in two the nasal ala and upper lip were repaired with a nasogenian and advancement flap for the lip (post-maxillectomy recurrence and Mustardé flap) and in another with a midfrontal and nasogenian flap for the upper lip (Figure 1, Figure 2 and Figure 3).
 Figure 1: (A,B,C) Nasal ala reconstruction with nasogenian flap with upper pedicle due to adenocarcinoma; (D,E) Nasal ala and upper lip reconstruction with nasogenian and lip advancement flaps.
View Figure 1
Figure 1: (A,B,C) Nasal ala reconstruction with nasogenian flap with upper pedicle due to adenocarcinoma; (D,E) Nasal ala and upper lip reconstruction with nasogenian and lip advancement flaps.
View Figure 1
 Figure 2: Nasal and upper lip reconstruction with midfrontal and nasogenian flaps.
View Figure 2
Figure 2: Nasal and upper lip reconstruction with midfrontal and nasogenian flaps.
View Figure 2
 Figure 3: Nasal cavity melanoma with invasion of soft tissues, periorbita and skull base (A,B,C) Resection; (C,D) Midfrontal and Mustarde flaps reconstruction; E) Postoperative after radiotherapy and before sectioning the pedicle of the midfrontal flap.
View Figure 3
Figure 3: Nasal cavity melanoma with invasion of soft tissues, periorbita and skull base (A,B,C) Resection; (C,D) Midfrontal and Mustarde flaps reconstruction; E) Postoperative after radiotherapy and before sectioning the pedicle of the midfrontal flap.
View Figure 3
All nasogenian flaps were dissected with upper pedicle.
In another patient, a Mustardé and midfrontal flap were used to repair the nasal dorsum and cheek skin.
In two, the nasal pyramid was reconstructed in three layers: Mucosa, with a unilateral flap from the lateral wall with anterior pedicle, cartilaginous support with cartilage grafts from the auricular concha, and coverage with a midfrontal flap.
The two patients previously had a partial anterior maxillectomy due to epidermoid carcinomas that compromised the floor of the nasal cavity (Figure 4).
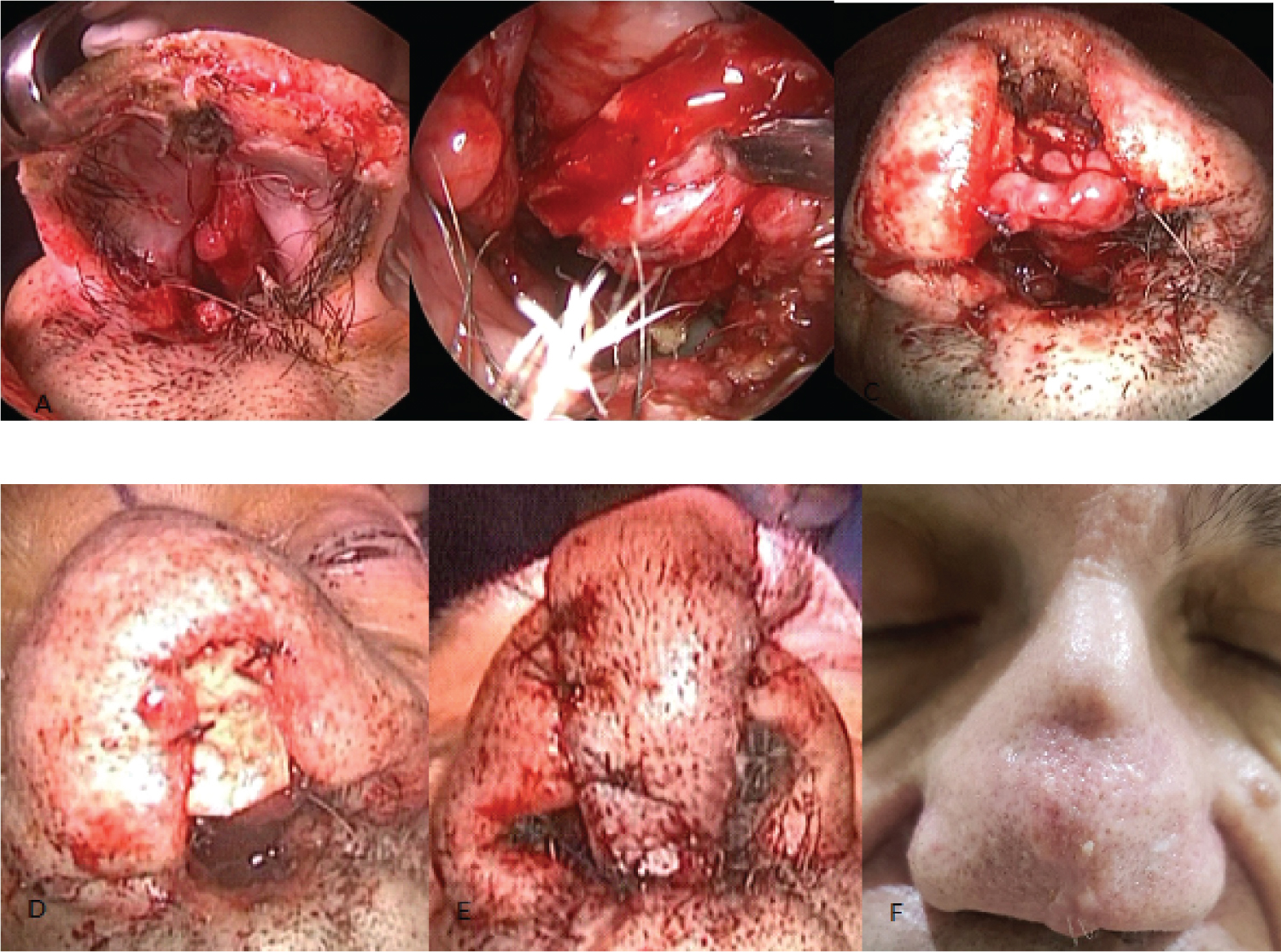 Figure 4: Multilayer nasal reconstruction (A) Rhinectomy; B) Mucosal reconstruction with lateral wall flap; C,D) Auricular concha cartilage graft; E) Midfrontal flap; F) Postoperative at 15 months.
View Figure 4
Figure 4: Multilayer nasal reconstruction (A) Rhinectomy; B) Mucosal reconstruction with lateral wall flap; C,D) Auricular concha cartilage graft; E) Midfrontal flap; F) Postoperative at 15 months.
View Figure 4
One of them had a recurrence 16 months later, and the defect caused by the resection was repaired using a contralateral lateral nasal wall flap, auricular cartilage, and midfrontal and Mustardé flaps. The reconstructions included the nasal tip, columella, nasal wings and in one also the nasal dorsum.
Three patients had previous or postoperative radiation therapy (Figure 5).
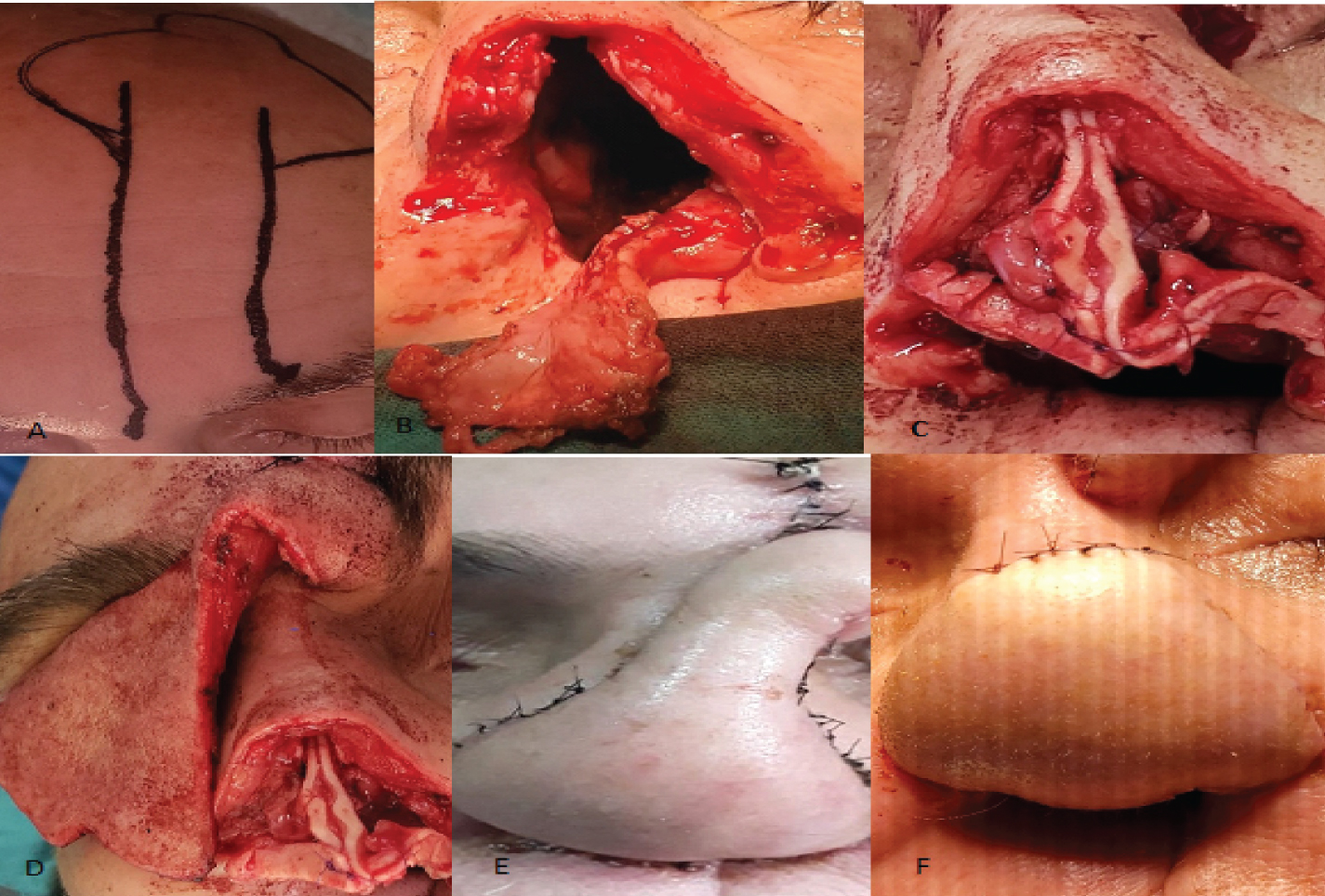 Figure 5: Total rhinectomy. A) Midfrontal flap; B) Lateral wall mucosal flap; C) Auricular concha cartilage graft; D) Midfrontal flap; E) Immediate postoperative; F) Postoperative after section of the pedicle of the midfrontal flap.
View Figure 5
Figure 5: Total rhinectomy. A) Midfrontal flap; B) Lateral wall mucosal flap; C) Auricular concha cartilage graft; D) Midfrontal flap; E) Immediate postoperative; F) Postoperative after section of the pedicle of the midfrontal flap.
View Figure 5
All defects could be completely repaired, there was no total or partial necrosis of the flaps. In two patients, a dehiscence occurred in the suture of the midfrontal flap with the upper lip (columella reconstruction).
In patients who had reconstructions with midfrontal flaps, a second surgical time was performed to section the pedicle between 45 and 90 days after the initial surgery.
In a patient with a mediofrontal flap, the donor bed could not be closed, leaving a sector of the frontal bone exposed, which required a third surgical procedure in which a rotating scalp flap was used to repair the defect.
In another of the patients, the thickness of the midfrontal flap used to repair the nasal tip was reduced and laser hair removal was performed with the DOT technique (CO2 laser and radiofrequency) (Table 1).
Table 1: Nasal reconstruction. View Table 1
In five patients, the cheek skin that was infiltrated by squamous cell carcinoma was reconstructed at the same surgical time as the maxillectomy.
In another patient, the skin of the cheek was resected in a second surgical procedure to widen the margin in a malignant Schwannoma of the infraorbital nerve.
In five patients the reconstructions were done with a Mustardé rotary flap and in another who had a total cheek defect (10 × 9 cm) and orbital exenteration with a posterior trapezius flap.
Three had adjuvant treatment with radiotherapy (Figure 6 and Figure 7).
 Figure 6: Total maxillectomy with invasion of soft tissues of the cheek. A) Maxillectomy and Mustardé flap incision; B,C) Patients after reconstruction.
View Figure 6
Figure 6: Total maxillectomy with invasion of soft tissues of the cheek. A) Maxillectomy and Mustardé flap incision; B,C) Patients after reconstruction.
View Figure 6
 Figure 7: Cheek and anterior maxillary sinus wall resection due to malignant schwannoma of the infraorbital nerve. Mustardé flap reconstruction.
View Figure 7
Figure 7: Cheek and anterior maxillary sinus wall resection due to malignant schwannoma of the infraorbital nerve. Mustardé flap reconstruction.
View Figure 7
In a patient with ecthyma gangrenosum that compromised the skin of the cheek, dorsum, lateral wall, left nasal wing, and the eye, an orbital exenteration and a wide facial skin resection (10 × 8 cm) were performed. The defect was reconstructed with a posterior trapezius musculocutaneous flap (cheek) and a midfrontal flap (dorsum, lateral wall, and nasal ala) (Figure 8).
 Figure 8: Cheek reconstruction with posterior trapezius musculocutaneous flap. A) Facial necrosis due to gangrenosum ecthyma: Necrotic facial tissue resection; B) Posterior trapezius musculocutaneous and midfrontal flaps; C) Closure of the donor site of the flap; D) Squamous cell carcinoma of the maxillary sinus with invasion of facial soft tissues; E) Computed tomography; F) Posterior trapezius musculocutaneous flap.
View Figure 8
Figure 8: Cheek reconstruction with posterior trapezius musculocutaneous flap. A) Facial necrosis due to gangrenosum ecthyma: Necrotic facial tissue resection; B) Posterior trapezius musculocutaneous and midfrontal flaps; C) Closure of the donor site of the flap; D) Squamous cell carcinoma of the maxillary sinus with invasion of facial soft tissues; E) Computed tomography; F) Posterior trapezius musculocutaneous flap.
View Figure 8
There was no total or partial necrosis of the flaps, nor dehiscence. The donor bed in the posterior trapezius flaps could be closed by dissecting and advancing the skin (Table 2).
Table 2: Cheek reconstruction. View Table 2
Resection of malignant tumors of the paranasal sinuses or nasal cavity with extension to the facial soft tissues or skin necrosis caused by infections, leaves defects that require a reconstruction to improve the function and obtain a good aesthetic result.
The nasal region is complex to reconstruct, since in cases of partial or total rhinectomy, the repair must be multilayered: Mucosal lining, cartilaginous support, and skin coverage [1].
The use of local flaps to carry out the reconstruction is the main option and there are several possibilities. The mucosa can be reconstructed with skin flaps such as the nasogenian flap or with mucosal flaps that are dissected from the nasal cavity.
The latter are the ones we prefer since they are located within the surgical field, they can be dissected using an endonasal approach or through the defect created by the oncological resection and under the magnified vision.
It is also the ideal tissue, with the same epithelium, which makes mucosal reconstruction more physiological.
There are different possibilities, but the unilateral lateral wall flap with or without extension to the nasal floor, with an anterior pedicle (anterior ethmoid and facial artery [2]) allows reconstruction of the mucosal lining, reaching the anterior sector of the nasal tip when it is rotated [3,4].
The cartilaginous support is obtained from cartilage grafts from the auricular concha with which the alar, columella and nasal tip cartilages are reproduced.
Skin coverage is achieved with the midfrontal flap with a unilateral pedicle (supraorbital and supratrochlear artery). It can be done in one time, tunneling the pedicle under the nasal dorsum or as we prefer, with an external pedicle and section after 45 days.
By performing the flap with a narrow pedicle (1.5 cm), the possibility of a new reconstruction with a contralateral flap can be preserved, as occurred in one of our patients.
In larger defects, reconstruction with free flaps may be an option, especially when the possibility of using local flaps is not feasible. The most used flap is the radial [5,6].
Bioengineering tissue using 3-D printing is a future possibility for nasal reconstruction.
Tissue development through bioengineering using 3D printing is a future possibility for nasal reconstruction. Instead of synthetic material, cells are placed to create solid organs. The advantages would be to perform the reconstruction in a single procedure, not using immunosuppressive drugs and not needing donor tissue from the patient [7].
Although no bioengineered solid organ has been transplanted into a human, bioengineered artificial skin is currently commercially available.
In small nasal ala defects, the nasogenian flap can be used, and it can also be useful in complex repairs of the nose and upper lip, as in one of the patients described.
The complications we had were two dehiscence of the suture of the midfrontal flap with the upper lip (reconstruction of the columella) without partial or total necrosis of the flap.
Both patients had an anterior partial maxillectomy of the infrastructure and used prosthesis to project the upper lip forward and fill the cavity. Possibly the modification of the projection of the lip when removing and placing the prosthesis again has favored the dehiscence.
Defects in the cheek region can be reconstructed when they are up to 6 cm with the Mustardé cervicofacial rotary flap. We have used it successfully in resections of the skin and subcutaneous soft tissues, due to infiltration of paranasal sinus tumors at the same time as the maxillectomy.
Cervicofacial rotary flaps can be dissected with an anterior pedicle (facial and submental artery) or posterior pedicle (superficial temporal artery and preauricular vessels in the face, vertebral and occipital artery in the neck, and perforating branches of the trapezium and thoracoacromial artery in the shoulder and thorax).
The dissection can be subcutaneous or in a deeper plane that includes the musculoaponeurotic system (advisable when there was previous radiotherapy).
In our patients, the reconstruction was with rotary flaps with an anterior pedicle, the dissection was subcutaneous and the defects compromised the entire thickness of the cheek.
In extensive facial defects and in cases where it was necessary to fill the defect created by a maxillectomy, even with orbital exenteration, the posterior trapezius musculocutaneous flap described by Dr. Francisco Demergaso was very useful for reconstruction.
The disadvantage of this flap is that the operative position of the patient must be changed from supine to lateral decubitus to perform the dissection, but its advantages are multiple: The possibility of repairing extensive defects, similar characteristics of the facial and back skin, very good irrigation through three vascular pedicles (transverse cervical, suprascapular and posterior scapular arteries) and adequate closure of the donor site [8,9].
Free flaps can also be an excellent option in these cases.
In the two patients with large defects in the cheek, the posterior trapezius flap was used to perform the reconstruction because one of them was operated on at the beginning of the series and we did not have a surgeon with experience in microanastomosis and in the other one who had an extensive skin necrosis, because he also suffered from multiple myeloma and had a high tendency to form thrombi, so we preferred to avoid a microanastomosis.
Nasal reconstruction
Rhinectomy:
• Midfrontal flap with unilateral pedicle + cartilage graft + lateral wall mucosal flap
Partial skin defects:
• Nose wing/columella: Nasogenian flap
• Nasal tip/dorsum/lateral wall/columella: Midfrontal flap with unilateral pedicle
Cheek reconstruction:
• Up to 2 cm direct closure
• Skin defects up to 6 cm: Mustardé flap
• Defects > 6 cm/post total maxillectomy/orbital exenteration: Posterior trapezius musculocutaneous flap or free flaps
Reconstruction of the nasal pyramid and cheek with local and regional flaps was very effective, as it allowed to repair defects of moderate and large size, as well as to reconstruct complex defects that included different regions of the face and a multilayer reconstruction.
There was no partial or total necrosis of the flaps, and only one defect in the donor bed required delayed closure with a rotary flap.
We believe that the use of these flaps continues to be the best option for reconstruction of these regions due to their excellent vascularization, reliability, and few complications.
The authors have no conflicts of interest to declare.