Vitamin D deficiency can cause many health problems and higher mortality. Chronic liver disease impairs vitamin D status by various mechanisms. The aim of our study was to estimate and directly compare vitamin D status in liver recipients before and within six months after LT to see whether there is an impact of restoration of proper liver function on 25(OH)D concentration.
Serum 25(OH)D concentration was determined and compared in the group of 110 adult patients before and within six months after LT. Measures performed right before transplantation were related to the etiology of liver disease, stage of cirrhosis and a season when the examination was done. 25(OH)D in the study group was also compared to the vitamin D concentration in the control group of 110 healthy persons matching the patients with respect to the age (p = 0.16), sex (p = 0.18) and body weight (p = 0.12). 25(OH)D concentration below 20 ng/mL was considered deficient, between 20 and 30 ng/mL insufficient and > 30 ng/mL sufficient. Frequencies of some clinical episodes like fractures, infections, deaths and diabetes mellitus were compared between groups.
25(OH)D concentration was significantly higher in the study group compared to the control group (20.83 + 13.48 vs. 14.8 + 8.39, p = 0.0001). There was a significant impact of summer-autumn season on better 25(OH)D concentration both in the study group and in the controls. The lowest concentration of vitamin D in the study group before LT was noted in alcoholic liver disease compared to the other etiologies (15.56 + 10.42 vs. 23.61 + 14.13, p = 0.002). The mean 25(OH)D concentration in the study group significantly improved after LT (27.37 + 12.5 vs. 20.83 + 13.48, p = 0.00001), but still more than 50% of recipients were significantly deficient.
Vitamin D deficiency is ubiquitous. Liver insufficiency does not have much impact on vitamin D status. Patients with chronic liver disease as well as healthy subjects require regular vitamin D monitoring and supplementation when appropriate. Patients with alcoholic liver cirrhosis and the end-stage disease are in a special need. After LT concentration of vitamin D improves, but more than 50% of the recipients require either proper prophylaxis or treatment.
Chronic liver disease, Deficiency, Liver transplantation, Vitamin D concentration
The term 'vitamin D' encompasses a group of steroid organic fat-soluble compounds, influencing many regulatory functions in humans, calcium homeostasis and bone metabolism being the most significant [1]. Vitamin D exists in two major forms: D2 and D3. The D2 form (ergocalciferol) derives from ergosterol, supplied to the organism with plant food and dietary supplements, whereas D3 form (cholecalciferol) is synthesized from cholesterol in the skin after exposure to ultra violet beam (UVB) light. This process is a source of 80-90% of vitamin D. Another source of D3 is fish and supplements ingestion, but dietary factor is not essential to cover requirements for vitamin D, as the exposure to sunlight should be sufficient, making this substance a hormone rather than a true vitamin. D2 and D3 are converted to an active form by carbon hydroxylation in positions 1 and 25. The first step of hydroxylation is done by the liver where 25(OH)D (calcidiol) is formed. The second hydroxylation - to the form of 1,25(OH)2D2 or 1,25(OH)2D3 (calcitriol) - takes place in kidneys and the other organs. Calcitriol is the right active hormone that stimulates vitamin D receptor. Circulating 25(OH)D binds to the albumin and vitamin D binding protein (DBP), and this complex reflects vitamin D reserves and makes up to 99% of its total concentration in the body [2]. Measurements of 25(OH)D are used to determine the vitamin D status, not only because of its highest concentration, but also because of the relatively long half-life of 2-3 weeks. The active form of vitamin D has a half-life of about 4 hours, 1000 times lower serum concentration, its level depends on 25(OH)D, and the metabolism is regulated by serum levels of parathormone (PTH), calcium and phosphates. Due to secondary hyperparathyroidism serum level of 1,25(OH)2D is frequently normal or elevated despite severe vitamin D deficiency [3].
Classically, vitamin D is responsible for the calcium-phosphate homeostasis and metabolism. It increases an uptake of calcium and phosphorus from gastrointestinal tract, and inhibits secretion of PTH by a direct influence on parathyroid glands and indirectly by increasing calcium and phosphorus concentrations. But the role of vitamin D is far broader. It regulates the expression of about 200 genes and its deficiency is associated with higher mortality, higher frequency of cardiovascular disease, malignancies, decreased immunity, infections and diabetes [4,5].
The most desirable serum level of 25(OH)D is around 30 ng/mL (~75 nmol/L). Levels between 20 and 30 ng/mL mean insufficient concentration, and below 20 ng/mL define vitamin D deficiency. Sometimes levels below 10 ng/mL are considered a severe deficiency. Vitamin D toxicity is rare, but levels above 100 ng/mL should not be exceeded [5,6].
In chronic liver disease the optimal vitamin D levels were not clearly defined, but according to the standard definition deficiency and insufficiency are observed in the majority of patients, ranging between 64 and 92% [7]. It is attributed to many factors such as: Malabsorption, liver failure to hydroxylate D2 and D3, and decreased albumin and DBP synthesis [8,9]. Moreover, bed-rest, quite common in the end-stage disease, and limited exposure to sunlight play an important role. The incidence of deficiency increases together with the progression of liver disease. Liver transplantation can reverse many pathophysiological mechanisms impairing vitamin D status and improvement in vitamin D concentration is expected in the recipients. Despite the potential of vitamin D deficiency to induce various morbid conditions, including dysregulation of immune cell function, important in the transplant setting [10], publications on vitamin D in the context of liver transplantation are scarce. The purpose of this study was to determine and directly compare vitamin D status in patients before and within six months after liver transplantation to see whether there are significant changes in 25(OH)D concentrations after restoration of proper liver function. Additionally, we aimed to evaluate 25(OH)D serum level in association with Child-Turcotte-Pugh (CTP) classification, etiology of liver disease (alcoholic versus non-alcoholic), model of end-stage liver disease (MELD) score and the time when surgery was done (winter-spring vs. summer-autumn).
This prospective cohort study was performed in the group of 110 consecutive patients transplanted between August 2015 and June 2017. This group consisted of 65 (59%) males and 45 (41%) females in the median age of 57 years (intelligence quotient range: IQR 45 - 63); The mean age was 53 + 13 years. The model of end-stage liver disease (MELD) was calculated in every case and the median score was 12 points (IQR: 8-17). CTP classification was as follows: Child A - 44 patients (40%), Child B - 45 patients (41%), Child C - 21 patients (19%). Alcoholic liver disease was diagnosed in 38 patients (35%), and in the remaining 72 patients (65%) the etiology was non-alcoholic with the predominance of HCC (23 patients) and chronic HCV infection (22 patients). The reason to transplant Child A patients was HCC in most cases. These data are shown in Table 1. In the post-transplant observation a special attention was paid on bone fractures, infections, diabetes mellitus and death.
Table 1: Characteristics of the study group and the control group. View Table 1
Control group consisted of 110 healthy persons with no evidence of liver disease (ultrasound normal, liver enzymes within normal range) matching the study group with respect to the age (p = 0.16), sex (p = 0.18) and body mass index (BMI, p = 0.1226). This group was selected from the HIV-negative controls, used for the project supported by the National Science Center in Poland: OPUS UMO-2011/01/B/NZ7/04260, devoted to vitamin D status in HIV patient population. Episodes of bone fractures were more frequent in the control group (p = 0.028), whereas diabetes mellitus (DM) was noted significantly more frequently in the study group (p = 0.0000). There were 9 deaths in the study group, 5 in the first 30 days post-transplant and no death was noted in the control group. Infectious episodes such as urinary tract infection, pneumonia, acute tonsillitis or sinusitis, erysipelas, etc., did not differ significantly between groups.
In all patients from the study group, 25(OH)D was measured before liver transplantation. LTs were performed between 1st of November and 31st of May in 76 patients, whereas in 34 patients LTs were performed between 1st of June and 31st of October. Similarly, the control group was divided in the same manner - 60 measurements were performed in the autumn-winter time, and 50 in spring-summer time. Vitamin D status was then checked in 105 liver recipients approximately 6 months after LT. In 5 patients it was not measured due to the early post-transplant death. These data are shown in Table 2. All post transplant patients received a daily dose of 600 units of vitamin D supplementation [6].
Table 2: Concentration of 25(OH)D in the study group and the control group. View Table 2
Statistical analysis was performed using the commercial software Statistica (13PL, STATSOFT Polska, Warsaw, Poland). The Mann-Whitney's U-test and Student-T tests were used for the comparisons of parametric independent variables, Wilcoxon test for dependent parametric variables and ANOVA and Chi2 test for non-parametric variables. Confidence intervals (CI) and interquartile ranges (IQR) were indicated where appropriate. P value < 0.05 was considered statistically significant.
The study group and the control group differed in respect to the 25(OH)D concentration which was significantly higher in the study group compared to the control group (20.83 + 13.48 vs. 14.8 + 8.39, p = 0.0001). Albeit higher in the study group, statistical significance disappeared between measures performed in summer-autumn period (20.15 + 8.88 vs. 24.7 + 13.48, p = 0.1006). Mean 25(OH)D concentration was significantly higher when examined in summer-autumn period in comparison with winter-spring measurements, either in the study group (p = 0.0435) or in the control group (p = 0.0002). It is shown in Table 2. The lowest concentration of vitamin D in the study group before LT was noted in patients with ALD and the mean value was comparable to the mean value in the control group (15.56 + 10.42 vs. 14.8 + 8.39, p = 0.6512), whereas it differed significantly from the mean 25(OH)D concentration in non-ALD patients (15.56 + 10.42 vs. 23.61 + 14.13, p = 0.002). These comparisons are shown in Table 3. Lower 25(OH)D concentration corresponded to the severity of liver disease as the MELD score was significantly higher in ALD group than in the non-ALD patients (16.13 + 7.99 vs. 12.92 + 7.71, p = 0.042) (Table 1).
Table 3: 25(OH)D concentration in the study group before and after LT. View Table 3
The mean 25(OH)D concentration in the study group was significantly higher after LT than before (27.37 + 12.5 vs. 20.83 + 13.48, p = 0.00001). According to ANOVA analysis deaths after transplantation were not correlated with vitamin D concentration, neither infectious episodes, de novo diabetes mellitus development and bone fractures (Table 4). Higher frequency of diabetes mellitus in the study group in comparison with the control group was related to the diabetogenic influence of immunosuppressive drugs such as prednisolone and tacrolimus, causing new-onset DM.
Table 4: Comparison of 25(OH)D concentration after LT (n = 105) in relation to the clinical episodes. View Table 4
The study group and the controls were also split into subgroups: with severe vitamin D deficiency defined as 25(OH)D < 20 ng/mL, insufficiency (25(OH)D 20-30 ng/mL) and sufficiency (25(OH)D > 30 ng/mL), and then compared. The Chi2 analysis revealed significant differences in percentage of subjects while comparing study group before and after transplantation to the control group, with higher frequency of vitamin D deficiency in the control group (76.4% vs. 51%; p = 0.00003 and 76.4% vs. 29%; p = 0.00000, respectively) (Figure 1 and Figure 2). The percentage of subjects in previously mentioned groups were also significantly different while comparing results in the study group before and after LT. After LT severe vitamin D deficiency was less frequent with higher frequency of vitamin D sufficiency. It increased from 29% before LT to 51% after LT (p = 0.036) as shown in Figure 3.
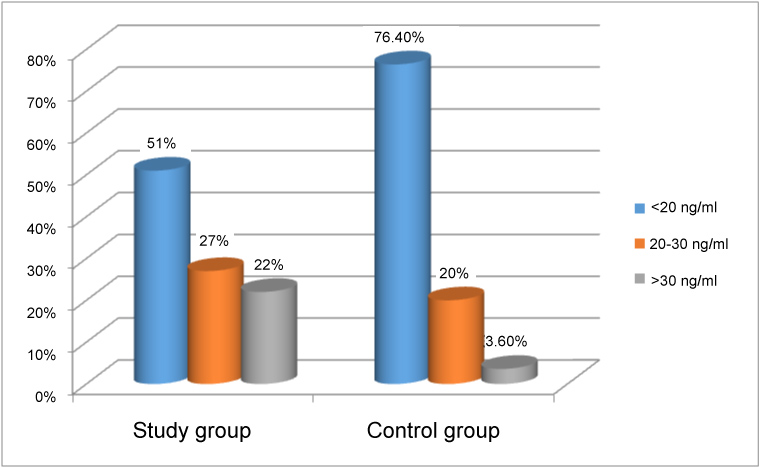 Figure 1: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/ml), insufficiency (25(OH)D 20-30 ng/ml) and sufficiency (25(OH)D > 30 ng/ml) between liver recipients prior to transplantation and the control group. View Figure 1
Figure 1: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/ml), insufficiency (25(OH)D 20-30 ng/ml) and sufficiency (25(OH)D > 30 ng/ml) between liver recipients prior to transplantation and the control group. View Figure 1
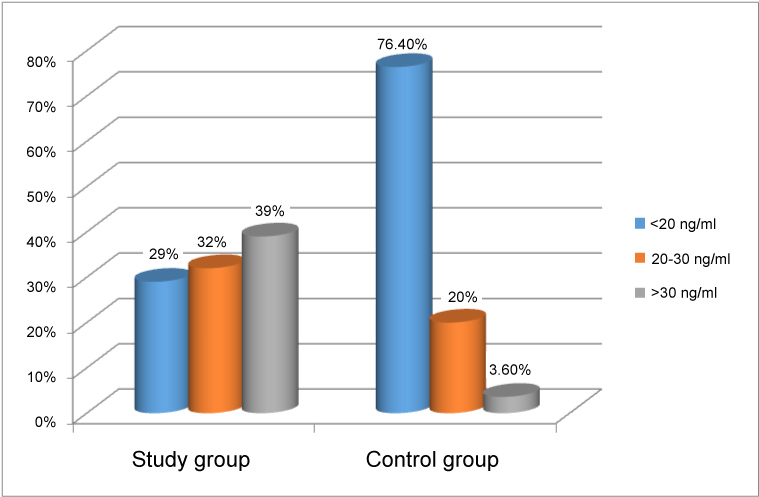 Figure 2: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/mL), insufficiency (25(OH)D 20-30 ng/mL) and sufficiency (25(OH)D > 30 ng/mL) between liver recipients after transplantation and the control group. View Figure 2
Figure 2: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/mL), insufficiency (25(OH)D 20-30 ng/mL) and sufficiency (25(OH)D > 30 ng/mL) between liver recipients after transplantation and the control group. View Figure 2
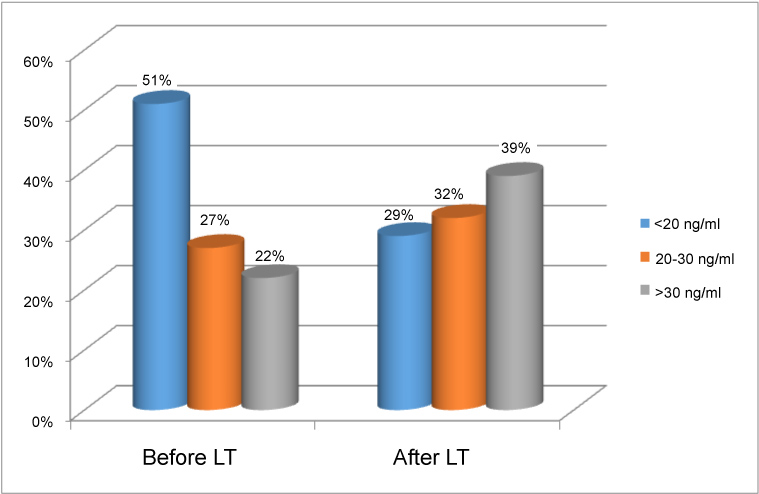 Figure 3: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/ml), insufficiency (25(OH)D 20-30 ng/ml) and sufficiency (25(OH)D > 30 ng/ml) between liver recipients before and after transplantation. View Figure 3
Figure 3: Comparison of percentage of subjects with severe vitamin D deficiency (25(OH)D < 20 ng/ml), insufficiency (25(OH)D 20-30 ng/ml) and sufficiency (25(OH)D > 30 ng/ml) between liver recipients before and after transplantation. View Figure 3
25(OH)D concentration differed in respect to the stage of liver cirrhosis. Child A patients had the highest vitamin D level when compared to the B and C classes (p = 0.0055). These differences disappeared after transplantation (Table 3).
Vitamin D deficiency is considered a world-wide problem. It is estimated that more than billion people in the world are mildly or severely deficient [11]. This deficiency is related to the inadequate sunlight exposure in most instances, even in sunny regions such as Australia, Middle East, India, Africa and South America [2]. Above or below certain latitude (33°) skin synthesis of vitamin D is almost absent in winter months, so at the end of winter more than 50% of healthy population in Northern Europe and in the United States show deficient vitamin D levels. In the summer months skin production of vitamin D can be reduced by many factors such as time of the day, clothes, topical application of sunscreens or skin hyperpigmentation. Sunscreens with protection factor of 30 (allowing to stay in the sun 300 minutes without burning by blocking UBV rays) reduce vitamin D synthesis in the skin by 95% [12]. Due to the fear of skin cancer the recommended time of sunlight exposure, however, was not proposed. Less important in causing vitamin D deficiency is poor dietary intake, higher need in some instances, decreased absorption or increases excretion. Very few foods contain naturally or are fortified with vitamin D, so people at risk require either prevention or treatment with vitamin D supplements for most of the year. Clinical consequence of vitamin D deficiency is rickets in children, osteoporosis and bone fractures in adults, tendency to develop diabetes mellitus, susceptibility to infections, cardiovascular complications and neoplasms [2,11]. It is also connected with depression, fatigue and obesity. It was shown that there is a relationship between low vitamin D concentration and breast, prostate and colon cancers [13]. The standard recommended daily intake of vitamin D for adults is 600 IU, but it is not known whether it is enough to protect from the potential nonskeletal health problems. To raise vitamin D to the appropriate level (> 30 ng/mL) in case of insufficiency approximately 1500-2000 units of D2 or D3 should be supplemented daily. Treatment in severe deficiency requires either dosing of 50,000 IU every week for 8 weeks or the equivalent of 6000 IU daily to achieve adequate concentration [6].
Our study clearly shows that vitamin D deficiency is virtually ubiquitous in the Polish population. More than 96% of healthy subjects and 78% of patients with chronic liver disease had insufficient 25(OH)D serum levels, more than half of controls being significantly deficient (< 20 ng/mL)and 36 (33%) severely deficient (< 10 ng/mL). In contrast to the other studies where the prevalence of vitamin D deficiency was higher in patients with liver failure than in the general population [7,8], in our study vitamin D concentration was paradoxically better in subjects with liver cirrhosis than in the controls, but it can be explained by the medical care provided in chronic liver disease and efficient supplementation in some patients in need. On the other hand, our results give evidence for the dramatic lack of practice guidelines to support vitamin D supplementation in the general population in Poland, especially in winter months. A higher number of bone fractures observed in the control group compared to the study group can be considered as one of the consequence of more frequent and more severe hypovitaminosis D. As expected, measurements performed between November and April showed deeper vitamin insufficiency/deficiency both in patients and in the controls what is consistent with the other studies [14,15].
In our study vitamin D deficiency correlated with worsening liver function expressed as class C in CTP classification and with alcoholic etiology. In ALD patients mean vitamin D concentration was comparable to the overall low concentration noted in the control group. Hypovitaminosis D is no longer considered typical for cholestatic liver disorders and is related to the degree of liver insufficiency rather than to the etiology [16]. Correlation of vitamin D deficiency with alcoholic etiology was reported else were [17]. In fact, ALD candidates were the sickest in the study group according to the highest MELD score.
As expected, after liver transplantation mean vitamin D concentration significantly improved as well as the percentage of patients with sufficient levels. This observation is consistent with the other studies [18]. Despite this favorable effect, six months after LT more than 50% of liver recipients are still grossly deficient of vitamin D. One of the explanations is that a routine supplementation with 600 IU/d of vitamin D does not cover needs in most instances; deficient patients require not prevention, but treatment and a proper maintenance therapy after achievement of the desirable level. Therefore, vitamin D status should be carefully monitored in every transplant recipient and treatment introduced when necessary. The recommended maintenance dose of vitamin D in deficient patients is 1500-2000 IU/d. Another reason for vitamin D deficiency is glucocorticoid therapy carried out as the element of immunosuppressive regimen by three to six months post-LT. In this period vitamin D requirements seem to be especially high and supplementation should be doubled or even tripled. This is very important in the prevention of falls and bone fractures as these incidents typically increase in the first months after transplantation in comparison with pre-transplant period [19]. Accordingly, in our study group all 9 episodes of fractures took place in the first six months post-LT. Transplant during winter months was performed at the worse vitamin D status than surgery done in summer-autumn season, so more effective supplementation has to be taken into account in running the post-LT patients in this period.
Our findings show that vitamin D deficiency is very common in the Polish population and almost everybody needs either treatment or supplementation, at least in winter. Liver dysfunction does not have much impact on vitamin D status. Patients with chronic liver disease as well as healthy subjects require regular vitamin D monitoring and supplementation when appropriate. Patients in a special need of supplementation are those with alcoholic liver cirrhosis and with the end-stage disease (CTP class C and MELD > 15). After LT concentration of vitamin D improves, but due to the regular controls and supplementation rather than restoration of liver function. Nevertheless, conventional prophylactic dose of 600 IU is far not sufficient in most instances.
Data from the project supported by the National Science Center in Poland: OPUS UMO-2011/01/B/NZ7/04260 were used in the study (project leader: Dorota Bander, MD, PhD).
Hanna Wiśniewska, Marta Bander, Aleksandra Biront - Acquisition of data, analysis and interpretation of data, Dorota Bander - The concept and design of the study, statistical analysis, Samir Zeair - Final approval of the version to be submitted, Marta Wawrzynowicz- Syczewska - The concept and design of the study, drafting the article and revising the manuscript.