The determination of brain death has long been legally established [1-3]. However, cultural and religious acceptance of brain death diagnosis in Asia still lags behind [4,5]. The Singapore Human Organ Transplant Act (HOTA) [6] is a legislative law that allows for recovery of four organs - kidneys, liver, heart and cornea in the event of death [3]. It is an opt-out system in which an individual above 21 of age, is deemed an organ donor if he or she is certified brain dead and had not opted out of HOTA. Opting out of being an organ donor can occur anytime by filling up a prescribed form. Once an objection is raised and acknowledged by the Director of Medical Service, it will be kept in a confidential registry governed by the Ministry and can only be assessed by the relevant personnel when required. This process of opting out can only be done by oneself and no next-of-kin can intervene before or after death. If no formal request to opt out of organ donation is made, presumed consent for organ donation applies to all Singaporeans who are deemed mentally competent and HOTA will kick in immediately once one passed away.
The Medical Therapy, Education and Research Act (MTERA) [7] on the other hand, is an opt-in scheme where people can pledge their organs or any body parts for the purpose of transplant, education or research after they pass away. This opt-in system can be done by the deceased themselves when they were alive or by their next-of- kin after they have passed on.
Despite these measures, the average waiting time for organs is long. The average waiting time for a kidney transplant in Singapore is still 9 to 10 years, and 1 to 2 years for liver or heart [8].
The COVID-19 pandemic makes the already difficult process more challenging given the limited resources available, the restricted movement of medical teams across institutions, the uncertainty of the transmission of the Coronavirus, the turnaround time for SARS-nCOV2 PCR testing in the deceased, the higher threshold for organ procurement, the stringent visitor policy, and the heightened emotions of the family members of the deceased [9-11]. We described a case of successful organ donation during this COVID-19 pandemic in an opt-out system in Singapore and outline the unique challenges in this system during a pandemic.
The patient is a 43-years-old gentleman with a history of poorly controlled diabetes, chronic pancreatitis and alcohol dependence. His alcohol dependence started since 2007 and he was admitted multiple times for alcohol related complications which included pancreatitis, dyspepsia, alcohol withdrawal and falls from alcohol intoxication. He was followed up by the Addiction Treatment Centre in Singapore and was offered the National Addictions Management Service (NAMS) which consist of a multidisciplinary team of addiction experts to assist patients through inpatient detoxification and at the same time, provides social and emotional support. Despite that, the patient was not compliant to the process of abstinence and defaulted his appointments recurrently. He was not known to be on long term medications based on the national electronic medical records, and he was not prescribed any long-term benzodiazepines, anti-depressants or anti-psychotics.
He was admitted after he was found by his roommate lying on the ground unable to move. He vomited prior to the ambulance arrival and upon arrival to the emergency department, he was intubated for airway protection due to a Glasgow Coma Score of 6 and for severe metabolic acidosis. He was diagnosed to have diabetic ketoacidosis and after stabilization of his blood pressure in the emergency department, he was sent for a Computed Tomography (CT) of his brain which revealed extensive intracranial haemorrhages with midline shift, subfalcine herniation and impending hydrocephalus (Figure 1). He was reviewed by the neurosurgeon and deemed to have very grim prognosis. After discussion with the family, surgical intervention was not offered.
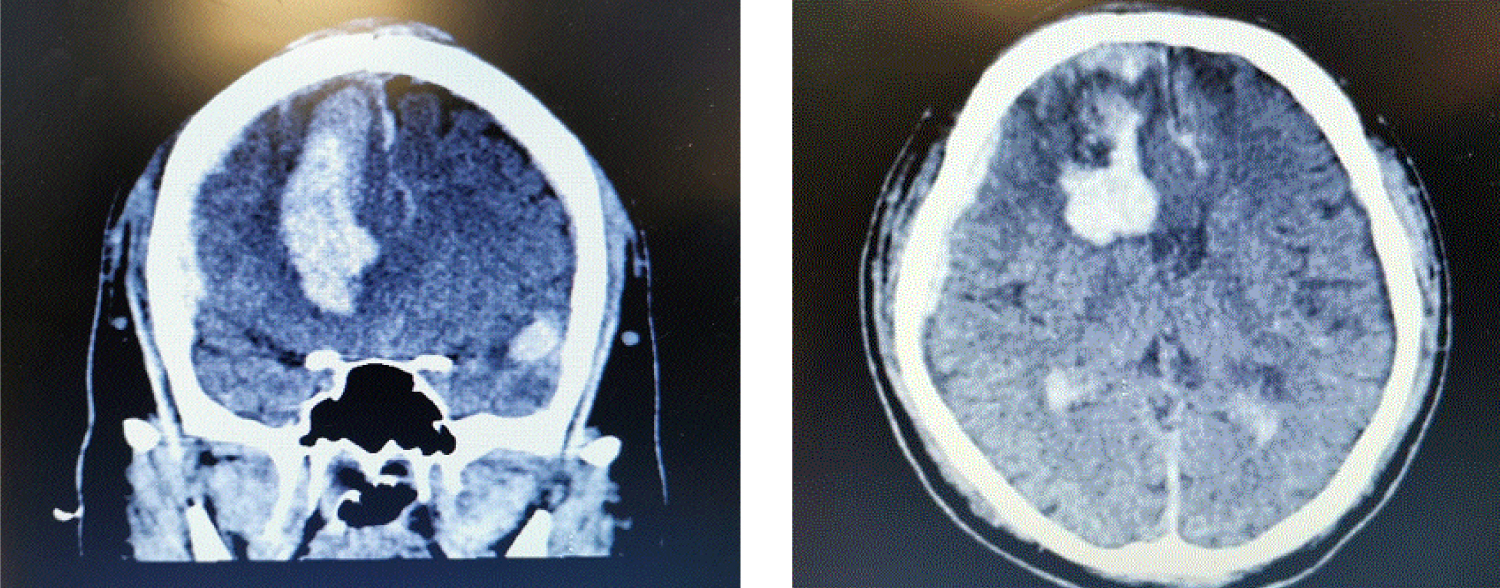 Figure 1: Computed tomography of the brain.
View Figure 1
Figure 1: Computed tomography of the brain.
View Figure 1
The chest X-rays on arrival to the emergency and after intubation were normal. However, the subsequent chest X-rays after resuscitation showed bilateral opacities in both the lower zone (Figure 2). Based on the latest case definition for COVID-19 suspect [12], the patient had to be screened for COVID-19. Hence, he was sent to the outbreak intensive care unit (ICU) for isolation and further management.
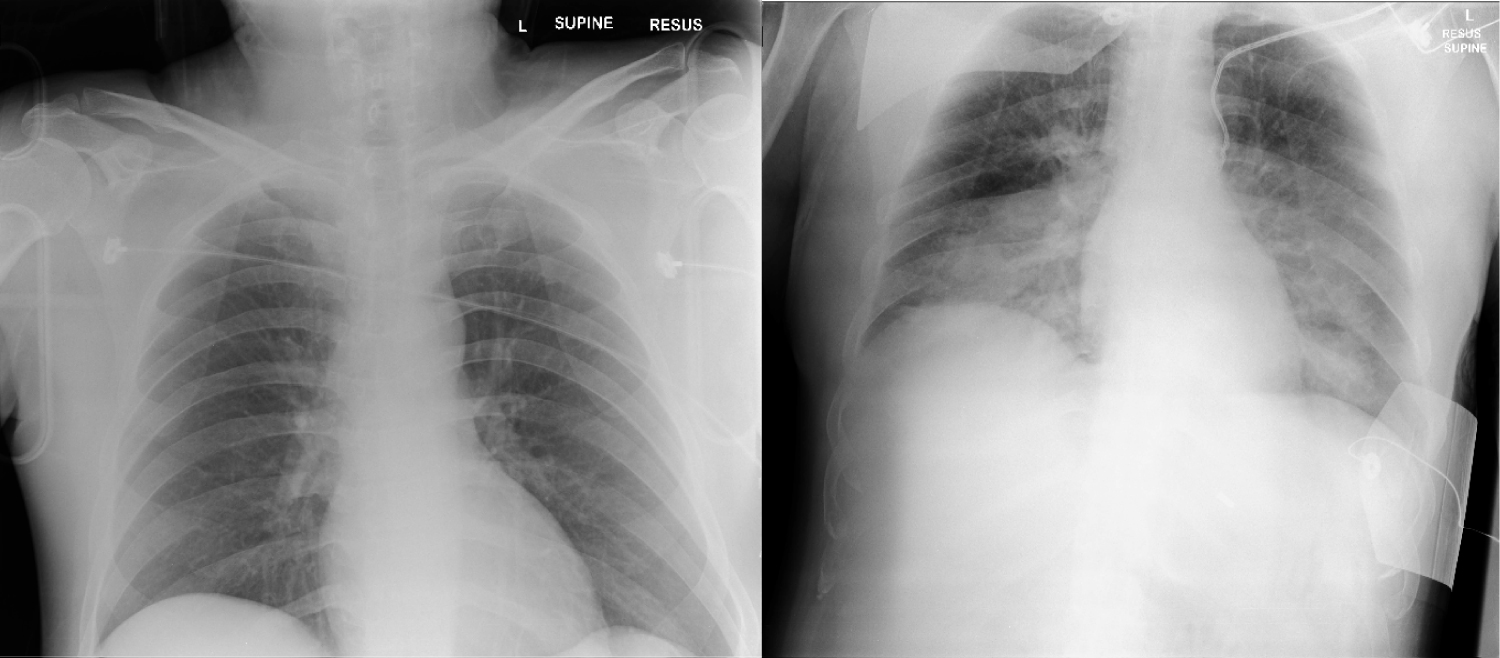 Figure 2: Chest X-ray before (left) and after resuscitation (right).
View Figure 2
Figure 2: Chest X-ray before (left) and after resuscitation (right).
View Figure 2
On arrival to the ICU, his pupils were fixed at 5 mm and there was no cough or gag reflex. There was also no spontaneous breathing. Medical treatment for diabetic ketoacidosis and septic shock from pneumonia were instituted. The patient also had KDIGO stage 1 acute kidney injury and mild ischemic hepatitis. His blood pressure was supported with adrenaline, vasopressin and noradrenaline to ensure mean arterial pressure target was met for cerebral and end-organ perfusion.
The patient stabilized after 24 hours of ICU support. His vasopressors requirement gradually decreased and both his creatinine and transaminases normalized by day 3 of ICU stay. However, his brainstem reflexes remained absent. Impending brain death certification and potential organ donation was informed to his parents as he was divorced. According to his mother, the patient had been doing odd jobs and staying with his friend since his divorce 3 years ago. His only child is under custody of his ex-wife and she has been updating his ex-wife about his condition as well. She also related the grim prognosis and potential course of brain death and organ donation to his ex-wife. We engaged the donor coordinator from NOTU and medical social worker from the hospital to prepare the family emotionally and mentally for the eventual process of brain death and organ donation.
Based on the national guidelines, all patients with pneumonia are considered COVID-19 suspect and will need to undergo screening to rule out COVID-19 [12]. Based on their epidemiological risk factors and 2 negative nasopharyngeal/sputum SARS-nCOV2 PCR tests, the patients will be de-isolated after a joint discussion with the infectious disease specialists [13].
The possibility of asymptomatic carriers and false negativity of the SARS-nCOV2 PCR is a real concern [13]. For organ donation and transplant, it is even more important to ensure both the transplant team and the transplant recipients are protected from getting the coronavirus [14-16]. Hence more stringent measures have been put in place. A deceased donor is excluded if he/she has a travel history in the last 28 days, or with respiratory symptoms or fever in the preceding 28 days without the presence of SARS-nCOV2 PCR test, or previously confirmed for COVID-19 infection but has recovered from the infection for less than 3 months [17]. Table 1 shows the organ and tissue recovery and transplantation activities to be continued in Singapore during the COVID pandemic.
Table 1: Organ and tissue recovery and transplantation activities to be continued in Singapore during the COVID pandemic [17]. View Table 1
According to the local guidelines, a potential organ donor will need 3 paired samples of nasopharyngeal and endotracheal samples of SARS-nCOV2 PCR to be negative. After brain death is confirmed, a CT thorax is required and further discussion with the infectious disease specialist from the recipient hospital will be done to assess donor suitability [17]. Figure 3 shows the workflow locally during the COVID pandemic.
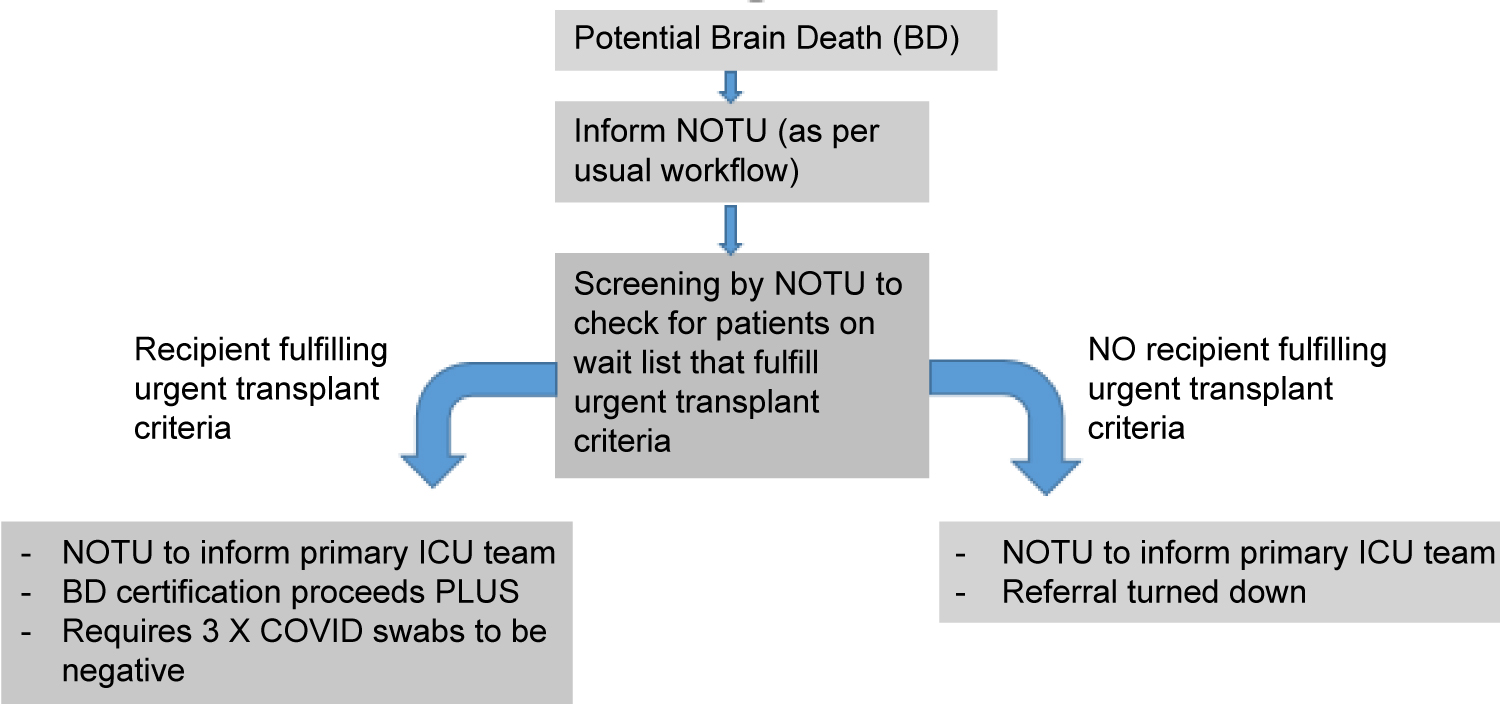 Figure 3: Workflow during the COVID pandemic.
View Figure 3
Figure 3: Workflow during the COVID pandemic.
View Figure 3
We identified the immediate goals to achieve in this case which include:
1. To continue the medical management of the patient while supporting the organs.
2. To confirm patient's COVID-19 status as soon as possible to allow visiting and to preserve the organ donation opportunity.
3. To facilitate the communication between the family and the patient and to allow the family to visit as soon as possible before the patient passes on.
We involved the donor coordinator from National Organ Transplant Unit (NOTU) to clarify the new guidelines involving COVID clearance. They also assisted to confirm that the patient has not opted out from HOTA previously.
Due to restrictions imposed by the COVID-19 outbreak, physical meet ups among different medical care teams was discouraged. We convened an urgent online meeting among the ICU consultant, the Infectious Disease Specialist and the ICU directors on Day 3 of ICU stay to review the guidelines on organ donation and transplant during COVID-19 pandemic. We also considered the possibility of fulfilling the stringent criteria of clearing COVID-19 status for organ donation and the time we had given the clinical instability of the patient. We decided that better medical decision can be made if we were more certain of patient's donation opportunity. If patient was deemed unsuitable for organ donation, withdrawal of treatment and palliation would allow the family to spend the last moments of life with the patient.
Hence we requested for a preliminary assessment of the chance of donation given the profile of the patient. A separate discussion was held with the various transplant teams from the other hospitals to assess the urgency and the likelihood of organ procurement and transplant in this patient. The patient was deemed a potential liver and cornea donor pending further assessment at time of procurement. At the same time, the patient was also assessed for lung donation as there was a potential recipient who required lung transplant urgently.
Concurrently, the infectious disease specialists in the various transplant teams worked with the primary team to assess risk of COVID-19 infection in the patient by reviewing the patient's epidemiological risks, presenting symptoms and the result of the samples sent. Two endotracheal samples, eighteen hours apart where already sent and were negative. There was a paired nasopharyngeal and endotracheal sputum sent and was pending at the time of discussion. The patient was deemed as low risk for COVID-19 infection and could be de-isolated and be accepted as a potential donor, if all four samples for SARS-nCOV2 PCR were negative.
Acknowledging the family's emotions and advocating for what were important to them were crucial. As the living next-of-kin was not given the right to oppose to the HOTA Act, we pre-empted the distress they may have to go through to accept organ donation as part of the process. Besides getting medical social worker to provide emotional support, the medical team also communicated frequently with the family to explain to them about HOTA and to prepare them for the eventual process of organ donation. We also set the timeline for them to anticipate updates from the doctors. In addition, we scheduled regular video calls to address the family's wish to see and talk to the patient.
The patient was de-isolated with four negative SARS-nCOV2 PCR samples and transferred to a non-outbreak ICU where the family can visit. The process of brain death certification was initiated, and the patient was certified brain dead after fulfilling all 7 criteria [9]. However as there was detectable levels of Diazepam on toxicology screen, supplementary test with radionuclide brain scan was done to confirm the diagnosis of brain death [9]. As the family finally saw meaning in organ donation, they also agreed to donate other organs besides the ones designated by HOTA. Hence the patient went on to organ donation under HOTA and MTERA and successfully donated his heart valves, iliac vessels and cornea. His liver was deemed unsuitable after on-table biopsy.
The family was supported throughout by the medical social worker, the NOTU coordinators and the medical team. They returned to expressed gratitude and that they could finally seek comfort that their son had done something good in his lifetime and that he continues to live on in the lives of the recipients.
The unique feature of an opt out system, with presumed consent for organ donation after brain death in Singapore as legislated in the HOTA law is not universally seen worldwide. This means that unless they have raised an objection to organ donation in their lifetime, all adults in Singapore are considered an organ donor when they pass away. This creates conflict between families and the medical team, particularly in cases when the family is not in agreement with organ donation often based on religious or cultural grounds. However, this practise of an opt-out system is increasing gaining traction, with countries like England, also adopting an opt-out system for organ donation.
Prior to the COVID-19 pandemic, discussion of brain death and HOTA is already a challenging process as there is always a minority of population who is not well aware of HOTA despite ongoing campaigns in the public. Even with publicity, it is still somewhat a taboo in the Asian culture to discuss about death and organ donation. The COVID pandemic poses additional complexity to the discussion of brain death and HOTA.
Firstly, the strict visitor policy in all hospitals does not allow family members to visit freely. This creates an emotional barrier for the family members to come to an acceptance of death as it deprives them of the physical contact with their loved ones during the last moments of life. Without a proper closure, it is hard for family members to accept their love ones passing on and even harder to discuss about organ donation and the logistical part of it.
Secondly, the logistical part of organ donation and transplant is made more complex with the addition of SARS-nCOV2 PCR testing [14-16]. The uncertainty of risks exposure, the possibility of a false negative test and the high stakes of passing on to a vulnerable recipient are real concerns. This resulted in stringent guidelines to rule out COVID-19 but the additional process further delay brain death certification and organ procurement. Some patients may be too unstable to last till organ donation. Prolonging the process also means the use of more resources in organ preservation and is definitely a consideration in this resource-limited pandemic.
Thirdly, the threshold of organ procurement is much higher to ensure safety to the transplant recipients [18,19]. This means that there will be more complexity and uncertainty to the process and outcomes even with experienced doctors. Thus, it is difficult for the attending physicians to counsel and guide family members through the process. Due to the heightened barriers, some attending physicians would prematurely deem their patient to be a poor candidate for organ donation; hence choose to palliate the patient from the start to save resources.
For our patient, there were a few dilemmas. Cognitively it appeared to be easier to discuss with family about palliation and withdrawal of treatment, but it is also important to preserve the donation opportunity which was meaningful to the family. However, to achieve that, it would mean a delay in de-isolating the patient and potentially deprive the family of being with the patient during his last moments of life. It would appear as a penalization to the family in pursuit of the goodness in organ donation. At the same time, the guidelines and the visitor policy need to be enforced given the high-stake consequences if any of the samples turn out to be positive.
The process of organ donation and transplant is not easy. It is more tedious and complex during COVID-19 pandemic. Our case study demonstrated that it is still possible through multi-disciplinary and inter-institutional coordination and effort. Also, bringing forward the process of donor assessment and recipient matching before brain death certification will help the attending physician to guide family better and decide when to withdraw treatment in order to conserved ICU resources in this resource-limited climate.
Every effort should be taken to preserve every donation opportunity. We often have a premature judgement whether or not a patient is a good enough candidate for donation. Physician needs to be aware of this cognitive bias when managing a patient with impending brain death. However, as demonstrated in this case of ours, organ donation is not restricted to solid organs only and a successful donation may mean more than we can imagine for some families.
It is always easier to take the easy way out especially during a pandemic crisis when complexities are increased, resources are limited and emotions are heightened. However, the demand for organs to save lives does not stop and we should not let the COVID-19 pandemic deter us.