Viral infections are a common cause of morbidity and mortality in transplant recipients.
To identify the most frequent viruses that affect Cuban transplanted patients and the value of the qPCR in the early diagnosis and treatment.
A total of 236 patients, 48 pediatric (30 liver, 13 kidney and 5 bone marrow) and 188 adult patients (44 liver, 96 kidney and 48 bone marrow) were studied. Serum and urine were analyzed prospectively by qPCR for CMV, HSV, EBV, HHV6, VZV, JC and BK for a period of 24 weeks.
Viral DNA was detected in 45.3% of the patients. Most patients tested positive for CMV (25.4%) or BK (21.2%). Although some differences in the frequency and type of viruses were observed between bone marrow and solid organ transplant, no association between viral load, virus disease and transplant type in adult or pediatric recipients was found. Analyzing all the recipients together, CMV was more frequently detected in serum and in patients with symptoms and complications. In general, CMV in serum, BK in urine and HSV in both samples (over 11950, 1.63x106 and 4265 copies/ml, respectively) predicted the presence of specific viral complications. All the patients responded to treatment, but three that died of complications directly linked to viral infection (one with BK and two with BK/CMV).
The early viral detection and follow up with qPCR allowed the opportune treatment. CMV, HSV and BK should be tested as part of the follow up of the Cuban transplant recipients.
Immune suppression after transplantation renders the transplant recipient vulnerable to a broad array of pathogens, being viral infections very common. Different viruses present different challenges at different times after transplantation due to variable degrees of immunocompromise in transplant recipients. Although cytomegalovirus (CMV) is the most common opportunistic pathogen seen in transplant recipients, other viruses may also affect clinical outcome. Among them, other herpesviruses, polyomaviruses and adenoviruses are important [1-3].
Some viruses stablish latency, whereas others are constantly replicating at low levels determined by the effectiveness of the host’s immune response. Multiple factors contribute to viral activation after transplantation, including immune suppression (especially reduction of cytotoxic immunity), graft rejection and therapy, inflammation (cytokines), and tissue injury [4]. The types and epidemiology of these infections are different between children and adults and depend on the type of transplant and the type and degree of immunosuppression [5].
Major advances in the management of all these viral infections have been achieved because of the availability of novel pharmaceutical agents. In addition, the establishment of polymerase chain reaction (PCR)-based qualitative and quantitative (qPCR) monitoring of viral DNA in blood, plasma or serum (DNAemia) has allowed optimal management of antiviral treatment in many countries, as it permits the identification of preclinical or early stages of virus-related pathology [6].
Cuba initiated the kidney transplantation program in 1970, the liver in 1986 and the bone marrow (BM) in 1985. In the year 2016 more than 5600 kidney, 370 liver transplants and 400 BM had been done [7,8]. However, before 2009, only serological pre-transplant screening was carried out, whereas specific viral tests (qualitative PCR) were requested when clinical signs and symptoms, suggestive of viral disease, appeared. In 2009 the routine monitoring at scheduled intervals of viral infections using quantitative methods was initiated [9] and the results are presented in this paper.
Thus, the aim of this research is first to identify the most frequent viruses that affect Cuban transplanted patients, including both adult and pediatric recipients and second to evaluate the impact of this monitoring in the management and outcome of the patients.
The study population included Cuban pediatric and adult patients who underwent to transplantation between November 2009 and February 2016. Part of the pediatric population follow up was published previously [9,10].
The main hospitals in Cuba that perform transplants: pediatric (University Pediatric Hospital "William Soler", University Pediatric Hospital of "Centro Habana", Institute of Hematology and Immunology) and adults (Clinical-Surgical Hospitals "Hermanos Ameijeiras", "Centro de Investigaciones Médico Quirúrgicas- CIMEQ" and the Institute of Hematology and Immunology).
A total of 48 consecutive pediatric patients undergoing solid organ transplantation (SOT) or bone marrow (BM) (30 liver, 13 kidney and 5 BM) and 188 adult patients (44 liver, 96 kidney and 48 BM transplant recipients) were included, for a total of 236 patients and 3874 samples. Samples were analyzed prospectively for a period of 24 weeks, except for autologous BM transplant recipients, which were only followed for one month. Table 1 provides general information about the studied cohort. Clinical and therapeutic follow-up information was available for 178 patients (41 children and 137 adults).
Table 1: General information of the transplanted patients studied. View Table 1
This research was approved by the Ethical Committees of the participating institutions and complies with the principles laid down in the Declaration of Helsinki. Parents provided informed consent with regard to the transplantation procedure, including extended viral monitoring. Clinical and therapeutic data from the transplanted patients were collected through a questionnaire performed to the patients or the parents (for pediatric recipients) as well as from clinical records of the patients.
The basic immunosuppressive regimen was triple therapy: anticalcineurinic (cyclosporine or tacrolimus), mycophenolate and steroids. CMV prophylaxis during the study period, in the adult centers, was pre-emptive treatment and, in the pediatric centers, universal prophylaxis.
One milliliter of serum was obtained before the transplant in order to investigate the serological status (IgG antibodies) of each patient and donor (when available) against Herpes Simplex virus (HSV), CMV and Epstein Barr virus (EBV) using ELISA assays and following the protocol described by the manufacturers (IBL, Hamburg, Germany).
One milliliter of serum and urine samples was obtained weekly in the first month post-transplant. At thirty to 90 days post-transplantation, samples were collected every two weeks. After 90 days, samples were collected monthly up to 24 weeks post-transplant. In total 11 samples of urine and serum were expected to collect per each patient.
Samples from all patients were sent to STI Laboratory of the Institute of Tropical Medicine ¨Pedro Kourí¨ (Havana, Cuba) for testing. Viral detection and quantification of CMV, EBV, HSV (HSV1 and HSV2), Varicella Zoster virus (VZV), Human Herpesvirus 6 (HHV6), and polyomaviruses (BK and JC) was prospectively monitored in serum and urine samples by qPCR.
DNA extraction was performed from serum and urine using QIAmp DNA minikit (Qiagen, Hilden, Germany) following the recommendations of the manufacturers. Seven different qPCR kits were used for the detection and quantification of CMV, EBV, HSV (including subtyping), HHV6, VZV and polyomaviruses (BK and JC within the same kit), following the protocols and the cycling parameters described by the manufacturers (TIB MOLBIOL, Germany). These kits were designed to be assayed under the LightCycler 1.5 platform (Roche Diagnostics, Germany). They include the mix (Light Mix) of specific primers and probes (hybridization probes) for each specific virus, the viral standards and an internal control. In addition the LightCycler FastStart DNA Master HybProbe was used to prepare the master mix for the qPCR.
The analysis and quantification of the samples were automatically performed by the second derivative maximum method, version 3.3 of the LightCycler software. The results were converted to copies/mL according to the formula (Result in copies/mL = Result in copies/μL × Elution volume in μL/Sample volume in mL). Clinical samples were considered negative (non-detectable viral load) if the crossing point exceeded the cycle 40 or if the viral load was below 10 copies/mL, described as the analytical detection limit of the kits.
For statistical analysis, a database was created using the package SPSS version 21.0. In order to determine an association among clinical features, serological results and/or virological findings, the odds ratio (OR) with 95% of confidence intervals were calculated. The presence of statistically significant association (p) was considered if p ≤ 0.05. Comparisons between different groups of patients or between samples were made by using the Fisher exact test, for categorical data, and for numerical variables the Kruskall-Wallis and Mann-Whitney tests were used.
Quantitative PCR was analyzed in two ways. The detection of any virus in patients/samples was interpreted as qualitative outcome and the results were interpreted as quantitative outcome and the numerical values of the viral load in each clinical sample were considered.
We assessed the discriminative power of the viral load level using recipients-operating characteristic curves (ROC). Their accuracy to discriminate between the viral load of a virus associated with further detection of another virus and/or an specific disease was classified according to the value of the area under ROC curve (AUC) [11] in: Non-informative (AUC ≤ 0.5), less accurate (0.5 < AUC ≤ 0.7), moderately accurate (0.7 < AUC ≤ 0.9), highly accurate (0.9 < AUC < 1) and perfect (AUC = 1). The value of the viral load with the highest sensitivity, above 50% specificity, for discriminating the detection of other virus was taken as the optimal cut-off point.
As shown in Table 1, the average of age and gender were similar in BM and SOT recipients, however female sex was more likely detected among pediatric recipients compared to adult recipients (29/48 vs. 84/188 p = 0.037, OR:1.89 CI:1.0-3.5). Sixty-six patients received the organ from a live donor (28.0%), mostly BM recipients.
Viral DNA was detected in 107 out of 236 patients (45.3%) and 19.4% of the screened samples (752/3872) (Table 2 and Table 3). Viral shedding in urine (39.4%, 93/236) was more frequent than shedding in serum (22.5%, 53/236). The median time to first detection of viral DNA following transplantation was 2 weeks (inter quartile range 1-3 [IQR]: 0-6 weeks). In urine, the interval was 2 (IQR: 0-6), while in serum it was 6 (IQR: 2-9.3).
Table 2: Distribution of positivity for different viruses, among Bone Marrow recipients studied. View Table 2
Table 3: Distribution of positivity for different viruses, among Solid Organ Transplant recipients studied. View Table 3
Most patients tested positive for CMV (60/236 patients, 25.4%) or BK (50/236 patients, 21.2%). The other viruses were less frequently detected (HSV: 5.1%, HHV6: 2.1%, EBV: 4.2%, JC: 11.9%) and VZV was not detected in any patient (Table 2 and Table 3).
CMV was more frequently detected in serum compared to the others viruses (43/53 patients with viremia; p < 0.001, OR:4.60, CI:2.12-9.99) (Table 2 and Table 3).
Twenty-eight patients out of the 60 positives to CMV (46.7%) were detected with CMV in the two compartments (serum and urine), being more likely that patients having CMV DNA detectable in urine also have CMV DNAemia (p < 0.001, OR: 9.33, CI: 3.9-21.8) compared with the other viruses.
The total of patients with any co-infection (including viral and nonviral) were 44 (18.6%) and 14.8% (35/236) showed viral co-infections either in the same or in different compartments at the same time point (concurrently). CMV was associated to co-infections (28/35 patients, p < 0.001, OR: 12.25, CI: 4.8-30.7) and CMV-BKV was the most common viral co-infection (20 patients), although other co-infections were detected (Table 4). Viral co-infections were more likely detected in pediatric patients than in adult recipients (12/48 vs. 23/188 p = 0.025, OR: 2.39, CI: 1.1-5.2, Table 4). HSV was only detected in adult recipients; the majority were HSV type 1, except for three liver recipients who excreted HSV 2 in urine.
Table 4: Viral co-infections detected in the patients studied, according to the type of transplant. View Table 4
Overall, pre-transplant seroprevalence to CMV, EBV and HSV was high in all the recipients and only significant differences were found for HSV, where lower frequency of prevalence were observed in children compared to adults (79.5% vs. 94.0% p = 0.023, OR: 4.01 CI: 1.4-11.6). Despite the majority of donors were seropositive for CMV, EBV and HSV (only five were seronegative), Seropositive donor (D+)/seronegative recipients (R-) status was not associated with viral disease.
In adults, for CMV, 9 patients were D+/R-, 3 D-/R- and 104 D+/R+. Three kidney recipients out of the 9 D+/R-, had CMV detection in serum and urine, asymptomatically, in the weeks 8, 10 and 20 of the follow up, and only one of them was pre-emptively treated with VGV. For HSV, 3 adult patients were D+/R-, 1 D-/R- and 112 D+/R+. Patient No. 43, from the D+/R-, had clinical symptoms, HSV in urine and was treated with ACV (Table 5). For EBV, the 2 D+/R- and the 1 D-/R- patients had no EBV detection during the follow up.
Table 5: Characteristics of patients and monitoring of viral load in those receiving pre-emptive or therapeutic antiviral treatment. View Table 5
The majority of the pediatric recipients were D+/R+. However, 4 pediatric recipients were CMV D+/R-, and two of them had CMV detection during the follow up, with other complications (no viral disease) that was successfully treated. Eight pediatric patients had HSV D+/R- and 4 EBV D+/R-, and none of them had viral detection or viral disease during the follow up.
Two hundred and one of the 236 transplanted patients (85.2%) had a successful outcome at the completion of the follow-up, with best results observed for adult recipients, compared to pediatrics (87.2 % vs. 77.1%, Table 1).
Pediatric bone marrow transplant: Viral DNA was detected in 2 out of the 5 patients (Table 2). One of these recipients had an autologous transplant and HHV6 DNA was detected in serum in the first two weeks after transplant, with no clinical complications (Supplementary Supplementary Figure S1A). The second patient (No. 17), had increasing BK load in urine (starting in 2nd week after the graft) and CMV and BK DNA detection in serum, particularly after the loss of the graft as consequence of the relapse of the disease, developing hemorrhagic cystitis (HC) and deceasing (Table 2, Table 4, Table 5, Figure 1A, Supplementary Figure S1A and Supplementary Figure S1B). Another pediatric allogenic BM patient deceased because of a relapse of the disease and a bacterial infection, after 4 weeks of the graft.
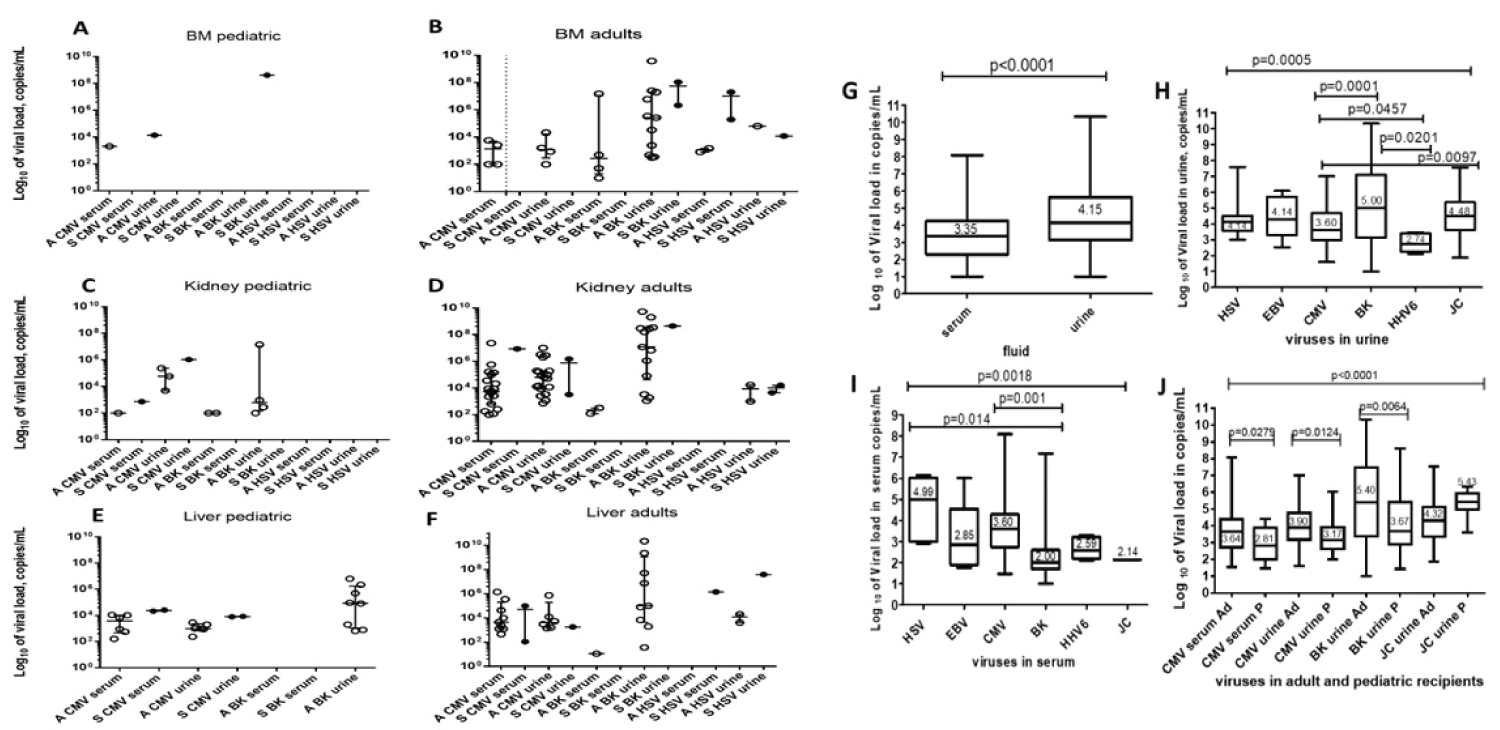 Figure 1: Viral load levels of the different virus detected according to type of transplant, clinical evolution, and type of fluid.
BM pediatric (A) and adult (B), kidney pediatric (C), Kidney Adult (D), Liver pediatric (E), Liver adult (F), Serum vs. Urine (G), viruses in urine (H), viruses in serum (I), viruses in adult vs. recipients (J).
Abbreviations: CMV: Cytomegalovirus; HHV6: Human Herpes Virus 6; EBV: Epstein Barr Virus; HSV: Herpes Simplex Virus; BK: BK Virus; JC: JC Virus; A: Asymptomatic; S: Symptomatic; Ad: adult; P: pediatric.
View Figure 1
Figure 1: Viral load levels of the different virus detected according to type of transplant, clinical evolution, and type of fluid.
BM pediatric (A) and adult (B), kidney pediatric (C), Kidney Adult (D), Liver pediatric (E), Liver adult (F), Serum vs. Urine (G), viruses in urine (H), viruses in serum (I), viruses in adult vs. recipients (J).
Abbreviations: CMV: Cytomegalovirus; HHV6: Human Herpes Virus 6; EBV: Epstein Barr Virus; HSV: Herpes Simplex Virus; BK: BK Virus; JC: JC Virus; A: Asymptomatic; S: Symptomatic; Ad: adult; P: pediatric.
View Figure 1
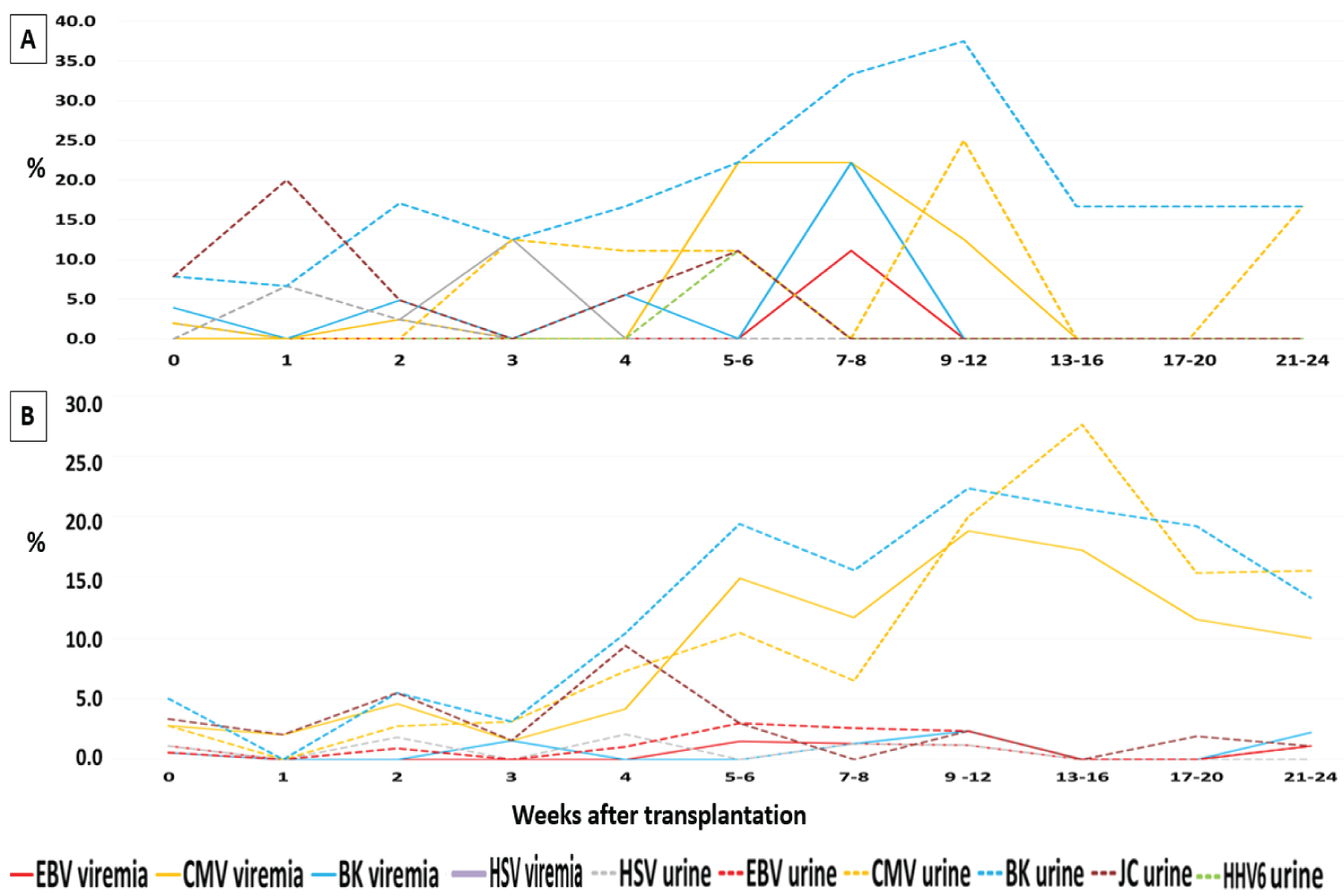 Figure 2: Longitudinal analysis of viral detection in clinical samples from transplanted patients during the 24 weeks of follow-up. (A) Bone Marrow recipients; (B) Solid Organ Transplant recipients.
Abbreviations: CMV: Cytomegalovirus; HHV6: Human Herpes Virus 6; EBV: Epstein Barr Virus; HSV: Herpes Simplex Virus; BK: BK Virus; JC: JC Virus.
View Figure 2
Figure 2: Longitudinal analysis of viral detection in clinical samples from transplanted patients during the 24 weeks of follow-up. (A) Bone Marrow recipients; (B) Solid Organ Transplant recipients.
Abbreviations: CMV: Cytomegalovirus; HHV6: Human Herpes Virus 6; EBV: Epstein Barr Virus; HSV: Herpes Simplex Virus; BK: BK Virus; JC: JC Virus.
View Figure 2
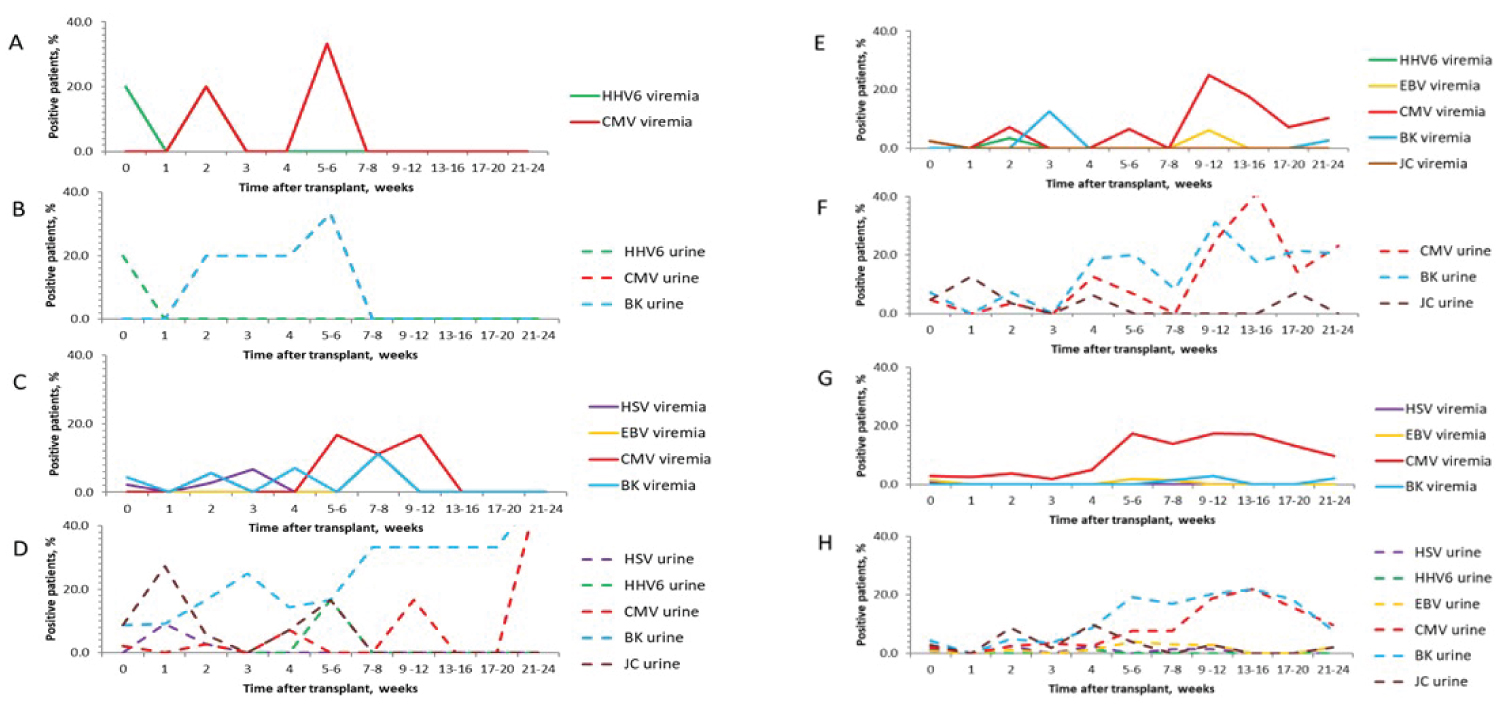 Supplementary Figure 1: Longitudinal analysis of viral detection in clinical samples from transplanted patients during the 24 weeks of follow-up. Bone Marrow recipients, BM Pediatric (A & B) and Adults (C & D); Solid Organ Transplant recipients, SOT Pediatric (E & F) and Adult (G & H).
Supplementary Figure 1: Longitudinal analysis of viral detection in clinical samples from transplanted patients during the 24 weeks of follow-up. Bone Marrow recipients, BM Pediatric (A & B) and Adults (C & D); Solid Organ Transplant recipients, SOT Pediatric (E & F) and Adult (G & H).
Abbreviations: CMV: Cytomegalovirus; HHV6: Human Herpes Virus 6; EBV: Epstein Barr Virus; HSV: Herpes Simplex Virus; BK: BK Virus; JC: JC Virus.
View Supplementary Figure 1
Adult bone marrow transplant: JC, BK and CMV were frequently detected in urine during the follow up. During the week’s fifth to 12 after transplantation there was an increase of CMV and BK DNAemia. After this date, BK and CMV viruria were frequently detected (Supplementary Figure S1C and Supplementary Figure S1D).
CMV, HSV and BK were commonly detected in asymptomatic recipients. The levels of Viral load of CMV and BK of asymptomatic recipients was not significantly different from the viral load of symptomatic patients (Figure 1D).
HSV was identified in two out of seven BM symptomatic patients (oral, trunk or genital lesions, Table 5) and in 2 patients with other complications (graft versus host disease and ameba enteritis). All these patients had an autologous graft and were having ACV prophylaxis (Supplementary Figure S1). Consequently, ACV dose was increased (400 mg every 4 hours orally or 5-10 mg/Kg/IV every 8 hours) showing an effective response to therapy (Table 5).
Three patients developed HC (patients No 84, 127, 181) and BK was detected in two of them. Patient No 181 lost the graft and deceased 28 days after transplantation due to this complication. Patients 84, 127, 20 and 79 had CMV detection and were treated with VGV pre-emptively, because they were asymptomatic or had another complication (Table 5).
In total, four adult BM patients (2 autologous and 2 allogenic) deceased during the follow up (1 graft versus host disease, 1 myocardial infarction, 1 post surgery complication, and 1 BK infection).
Pediatric solid organ transplant: Viral detection was over 50% in this group, mainly due to urine shedding of CMV and BK. Liver recipients had more diversity of viruses detected in serum (Table 3). Viral co-infections were detected in over 20% of the recipients, with CMV/BK being the most frequent (Table 4).
During the follow up, CMV viremia was detectable in more than 20% of the patients in the weeks 9 to 16. There was also an increase of the CMV and BK shedding in urine after week 9 of the graft (Supplementary Figure S1E and Supplementary Figure S1F).
Viral load between asymptomatic and symptomatic recipients was similar (Figure 1B and Figure 1C). Patients No 22, 23 and 15 had CMV complication and were treated with GCV or VGV (Table 5). Other patients had CMV in serum and suffer another complication (Patient No. 18) or were asymptomatic (Patients No. 1, 8 and 12) and received pre-emptive antiviral treatment (Table 5).
Five patients deceased in the first two weeks after the graft due to mainly by complications directly linked to the surgery or due to the low Karnofsky performance status at the time of transplantation. Four patients lost the graft due to acute rejection (1 kidney), rejection as a result of discontinuing the immunosuppressive therapy (1 liver), and two with vascular thrombosis (kidney recipients).
Adult solid organ transplant: Liver recipients had more virus detection compared to kidney recipients, mainly due to polyomavirus shedding in urine (Table 3). JC was more likely identified among adult liver recipients compared to kidney recipients (11/44 vs. 7/96, p = 0.005, OR: 4.24, CI: 1.56-11.5, Table 3). JC shedding was frequent in the first month after the graft. BK and CMV shedding in urine started increasing the frequency after the first month (Supplementary Figure S1H). Viremia was detected mainly due to CMV, particularly after the fifth week of the graft (Table 3, Supplementary Figure S1G).
Viral load of CMV and BK was variable in asymptomatic SOT recipients and was not different from the symptomatic patients (Figure 1E and Figure 1F).
CMV was found causing direct complications in five patients (patients No 21, 38, 101, 148, 198, Table 5), who were treated with GCV or VGV. One of these patients had a fatal evolution, besides the GCV treatment (adult liver recipient, patient No 21). Patients No. 29, 91 and 93 had other complications with CMV detection and were treated with specific treatment and antivirals (Table 5). CMV was also detected in asymptomatic kidney recipients who received pre-emptive antiviral treatment (patients No 10, 11, 43, 44, 57, 82, 83, 87). HSV was causing symptoms in 5 SOT recipients (patients No 29, 93, 26, 39 and 43), mainly in the first month after the graft. Antiviral therapy on these patients was effective (Table 5).
Fifteen SOT recipients deceased due to surgical complications (2), vascular thrombosis (2), infection (4, 1 CMV, 2 sepsis and 1 central nervous system), acute rejection (2), dysfunction of the graft (3) and Diabetes mellitus (2). Additionally, five patients lost the renal graft due to acute rejection (2), vascular thrombosis (1), bacterial infection of the graft (1) and dysfunction of the graft (1).
Comparison between transplant types and group of age: Some differences were observed between the type of transplant and between adults and pediatric recipients, regarding the frequency of different viruses: CMV DNA detection was more likely detected among pediatric recipients (35.4%) compared to adult recipients (22.9%, p = 0.057, OR:1.85, CI: 1.00-3.63, Table 2 and Table 3). CMV was more likely detected in SOT recipients in comparison to BM recipients (29% vs. 13.2%, p = 0.02, OR: 2.67, CI: 1.15-6.17), this difference was also significant for adults liver recipients compared to adults BM recipients (31.8% vs. 12.5%, p = 0.023, OR: 3.10, CI: 1.12-8.51) (Table 2 and Table 3). HSV was only detected in adult recipients, the majority were HSV-1, except for three liver recipients who had HSV-2 in urine. HSV was more frequently identified in BM recipients compared to SOT recipients (6/53 vs. 6/183, p = 0.019, OR: 3.76, CI: 1.22 11.62). BK was more likely observed in adult BM recipients (14/48, 29.2%) compared to adult kidney recipients (14/96, 14.6%, p = 0.03, OR: 2.39, CI:1.05-5.42).
Viral load analysis for the different viruses in each type of fluid: In general, viral loads in urine were significantly higher than in serum (median: 1.43 × 104 vs. 2.25 × 103 copies/mL, respectively, p < 0.001, Figure 1G). CMV load in urine, at the cut off 134 copies/mL, predicted CMV DNAemia (less accurate prediction, AUC = 0.672, sensitivity of 73.3%, specificity of 51.2%). In the same way, BK load in urine, at the cut off 325 copies/mL, predicted BK DNAemia (moderately accurate prediction, AUC = 0.879, sensitivity of 87.4%, specificity of 76.9%).
The viral load levels, among viruses excreted in urine, were significantly different (p < 0.001). CMV exhibited significant lower viral load compared to BK and JC (p = 0.046 and p = 0.009, respectively) (Table 2, Table 3 and Figure 1H).
In serum, viral load levels from the different viruses detected were also significantly different (p = 0.002). CMV and HSV exhibited significantly higher viral loads compared to BK (p = 0.001 and p = 0.014, respectively) (Table 2 and Table 3, Figure 1I).
The detection of CMV in serum, at the cut off 550 copies/mL, was moderately accurate for prediction of BK detection in this fluid (AUC = 0.879, sensitivity: 92.3%, specificity: 75.3%).
Viral load in adults showed significant higher values compared with children (p < 0.001 in general, p = 0.028, p = 0.012 and p = 0.006 for CMV in serum, CMV in urine and BK in urine, respectively, Figure 1J).
The analysis of viral load values according the type of transplant only exhibited significant differences for CMV in urine, being the viral load in this fluid higher in kidney recipients (p < 0.001), compared to liver and BM recipients. No further differences were observed (data not shown).
General viral detection and clinical impact: Overall, 39 patients received antiviral pre-emptive or therapeutic treatment as it is shown in Table 5.
In general, CMV was the virus most frequently identified in patients with symptoms and complications. CMV load in serum over 11950 copies/ml predicted specific viral disease (less accurate prediction, AUC: 0.672, sensitivity and specificity 75%, p = 0.128). Five patients developed HC (pediatric BM No 17, adults BM 84, 127, 181, and adult kidney 100) and BK was detected in four of them; thus, HC was associated to BK infection (p = 0.001, OR: 16.5, CI: 1.8-151.5). BK load in urine over 1.6 × 106 copies/ml predicted HC (less accurate prediction, AUC: 0.640, sensitivity 75%, specificity 57.8%, p = 0.361). Four of the five patients presenting this clinical complication were BM allogeneic recipients and two of them (patients pediatric No 17 and adult 181) lost the graft and deceased.
HSV detection over 4265 copies/ml in serum and urine predicted the presence of lesions (moderately accurate prediction, AUC: 0.816, sensitivity 100%, specificity 57%, p = 0.047). No significant association between immunosuppressive regimen and CMV or BK detection was found (p > 0.05, for the 178 patients with therapeutic follow up information). Sixteen patients had suspended or diminished the doses of some of the immunosuppressive drugs because of toxicity.
During pre-emptive therapy, no severe toxicities were observed. At the end of the follow-up three patients died of complications directly linked to viral infection and five patients had detectable virus, although no symptoms were detected (Table 5 and Figure 2).
The survival at 6 months after the graft was 85.2%, mainly due to surgical complications or to the low Kanorfski performance status [12] probably due to a delay in the transplant procedure because of the lack of compatible donors [13,14].
The pre-transplant seroprevalence of the EBV, CMV and HSV was high, in accordance with previous Cuban studies [15-17] and was not found to be a risk factor for developing viral disease, probably due to the close follow up and pre-emptive treatment.
The value of viral detection in urine would be the early detection, close follow up and treatment, especially for BK [18,19]. The frequency of virus shedding in urine was higher than the virus in serum and importantly viral urine shedding predicts the viremia, for BK [18,19]. The reactivation of CMV and BK in the places that they usually stablish latency is probably the first step after the immunosuppression is settled or increased and a secondary viremia is the consequence of the inability of control the viral replication in the initial site of reactivation. CMV and BK are opportunistic viruses commonly associated with higher immunosuppression level [20,21].
Detection of virus co-infection was common; particularly CMV and BK. This co-infection has been reported previously to be frequent in transplant recipients [22]. Is in debate how significant is the role of each of these viruses in the replication of the other [23,34].
The virus detection related with time was in agreed with other studies [25]. There was a delay in viremia and viruria in pediatric SOT probably due to the universal antiviral prophylaxis.
Virus shedding was common in urine and this confirms the value of urine as sample for the follow up of transplant recipients (except for BK). Viral load was not associated with viral disease in any particular transplant in the pediatric or adult populations; which constitute a limitation in the analysis of the results. When the results were analyzed in general, CMV, BK and HSV detection over certain cut off predicted the occurrence of viral disease. The present study confirms the value of qPCR for the follow up of transplant recipients and the monitoring the response to antiviral treatment. The majority of the patients responded to the specific antiviral treatment or the modification of the immunosuppression. The level of immunosuppression was not analysed in this study because of the lack of related data, constituting one of the limitations of the present study.
HC is a cause of morbidity in BM patients and is usually associated with reactivation of BK, adenovirus and CMV. Urine BK load value, with less accurate power, predicted HC and multiple studies have evaluated the factors associated with HC in allogeneic BM transplanted patients [19,26] or in kidney recipients [18].
Currently, there are recommendations for screening for BK in urine, with close monitoring for symptomatic patients for BK viruria after transplant, physicians will be able to intervene before complications appear [18,19,27].
There are recognized risk factors for CMV detection/ reactivation/disease as CMV seropositivity before transplant, acute rejection, graft-versus-host disease, lymphocyte depleting antibodies, HLA mismatch and other infections [20,28-30]. These factors were not identified in the present study, because one of the main limitations of this study was the lack of complete clinical records.
Other reports showed that patients with symptomatic CMV infection had significantly higher level of viral load [31,32]. Despite advances in post-transplantation care, CMV infection remains as the most common viral infection after transplant. The proper management of transplanted patients with CMV infection relies on the management of CMV levels by means of quantitative analysis of CMV markers.
Less frequent detected but associated with a particular type of transplant were JC with adult liver transplant and HSV with adult BM. JC has been reported as commonly excreted in urine of liver transplanted patients [33]. HSV is usually detected in the first month after transplant causing clinical skin or mucosa reactivation, particularly in very immunosuppressed recipients [34]. HSV detection and symptomatology should be minimal with the ACV prophylaxis. The presence of other complications or inadequate prophylaxis antiviral level could be the possible explanation of finding HSV in patients with ACV prophylaxis.
This study covers the detection and quantification of 7 opportunistic viruses during the follow up of 3 transplant types in adults and children. Importantly, the early viral detection allowed the opportune treatment. CMV, HSV and BK (in general) were common and were associated with specific viral disease and these viruses should be monitored in the follow up of Cuban transplant recipients.
To Calixto Hernández, José Antonio Copo, Aramís Núñez, Julio Valdivia, Margot Martínez, Julio César Hernández, Lourdes Pérez, Diana P. Duran, Yardelis Perez, Nancy Cazorla, Alberto Arencibia, Mabel González, and Iliana Alvarez for the contribution designing the study and the recruit of patients. The authors thank the NGO MediCuba-Suisse for the financial and material support through the collaboration project entitled: "Implementación en Cuba del monitoreo de los principales agentes virales que afectan a pacientes receptores de trasplante".