With over a billion people across the globe living with hypertension and over a tenth of the global annual mortality being attributed to hypertension, it is no surprise why this disease is of great public health concern. In the bid to reduce the prevalence of hypertension by 25% by the year 2025, recent data about the current prevalence and disparities in health intervention is required. This study provides relevant information about the prevalence of hypertension in a distant rural community in Southwestern Nigeria, and the available hypertension monitoring and management services available in the community. The community-based survey was cross-sectional in design; purposive sampling was used to select 138 adults from about 500 rural dwellers. Data was analyzed using descriptive and inferential statistics like chi-square, t-test and ANOVA which were measured at 0.05% level of significance. The respondents' average age was 45.96 ± 16.89 years; their major occupations were farming 72 (52.2%), and trading 36 (26.1%). The study recorded 26.8% prevalence of hypertension among the villagers; the prevalence of hypertension was higher among women (30.0%) than the men (20.8%). There were statistically significant associations between the respondents' age and their systolic blood pressure-SBP (p = 0.000) and diastolic blood pressure-DBP (p = 0.021). There were no statistically significant relationships between the sex of respondents and their SBP (p = 0.370) and DBP (p = 0.605). There were statistically significant differences between the respondents' marital status and their average SBP (p = 0.021) and average body weight (p = 0.002). There were no laid structures for monitoring and controlling the prevalence of hypertension in the village. The village was void a functional primary health care centre and pharmacy. Reducing the prevalence of hypertension significantly cannot be achieved if the rural communities are sidelined from health interventions. It is recommended that all Federal and State Governments, Non-governmental organizations, and private organizations support the Local Government by providing necessary resources required for effective health monitoring and management.
Hypertension, Rural community, Health monitoring, Disparities
Hypertension is a global menace contributing to a significant morbidity and mortality numbers; over a billion people across the globe are living with hypertension and over a tenth of the global annual mortality is attributable to the disease [1,2]. Hypertension is also commonly regarded has a silent killer due to its asymptomatic nature at the early stages, by the time symptoms appear the cardiovascular system must have been subjected to consequential damage [3]. Due to the detrimental impact of non-communicable diseases like hypertension, global leaders representing all 194 WHO member states set a target for a 25% relative reduction in the prevalence of hypertension by 2025 [4].
Globally, disparities exist in relation to the prevalence of hypertension. For instance, the burden of hypertension in Africa has been estimated to be greater than any other region [2]. According to a WHO status report for non-communicable diseases in 2010, about half of the adults in the Africa region were hypertensive [1]. Although the disparities in prevalence between rural and urban areas are not conclusive, previous studies have suggested higher urban prevalence [5,6] while more recent studies reported varying results. A survey assessing the rural-urban disparity within Chinese communities revealed small difference between rural (47.2%) and urban prevalence (48.6%) [7]. Other studies in Northeastern China reported a higher prevalence of hypertension among rural areas; a study by Xing, et al., reported a 52.5% prevalence in the rural area compared to 50.2% the urban area (50.2%) while another study reported a prevalence of 25.9% among rural dwellers and 22.7% among urban dwellers [8]. However, in Uttar Pradesh; a State in Northern India, urban prevalence was 10.5 while rural was 8.3% [9]. While in Nigeria, an urban prevalence of 30.6% and a rural prevalence of 26.4% were reported [10].
Another survey, conducted in rural and urban centers in Akwa Ibom State; South southern Nigeria, reported that hypertension prevalence was significantly higher in the rural communities (44.3%), compared to the urban areas (28.6%) [11]. Prevalence from other surveys conducted in Nigerian urban centers has reported, a 33.1% prevalence among adults in Ibadan North Local Government [12], a 27.5% prevalence in Lagos city [13], and a 22.8% prevalence in Anambra State [14]. Studies conducted in rural areas reported: A prevalence rate of 19.3% [15], a 32.8% prevalence rate in communities in the south [16], and a 44% prevalence among communities in Delta State [17].
Even with the evident prevalence of hypertension in both rural and urban areas, majority of the interventions being implemented to curb this menace has been focused more on urban areas as opposed to rural communities [18,19]. In the bid to reduce the prevalence of hypertension by 25% by the year 2025, it is essential to also prioritize rural interventions. This study aims to provide data on the prevalence of hypertension in a marginalized rural community in Southwestern and Nigeria and also assess whether there are structures in place to monitor and control hypertension.
The study was carried out in Abimbola, a rural village located in Ayedaade Local Government Area (7°19'N4°21'E/7.317°N4.350°E), Osun State in the Southwestern region of Nigeria. Ayedaade is situated in the northern area of Gbogan town, which is surrounded by Isokan, Irewole and Aiyedire to the east and Ife north to the west. It consists of over 50 districts and villages, including Abimbola community where this study was conducted. There are around 70 households in the village, with a population of about 500. The people belong to the Yoruba speaking tribe and the predominant occupation of the people were farming and trading. A medical outreach was conducted in the community by trained medical practitioners under the auspices of an Non-Governmental Organization (Livingstone Explorers Initiative) for three days. Figure 1 shows the Map of Ayedaade LGA [20].
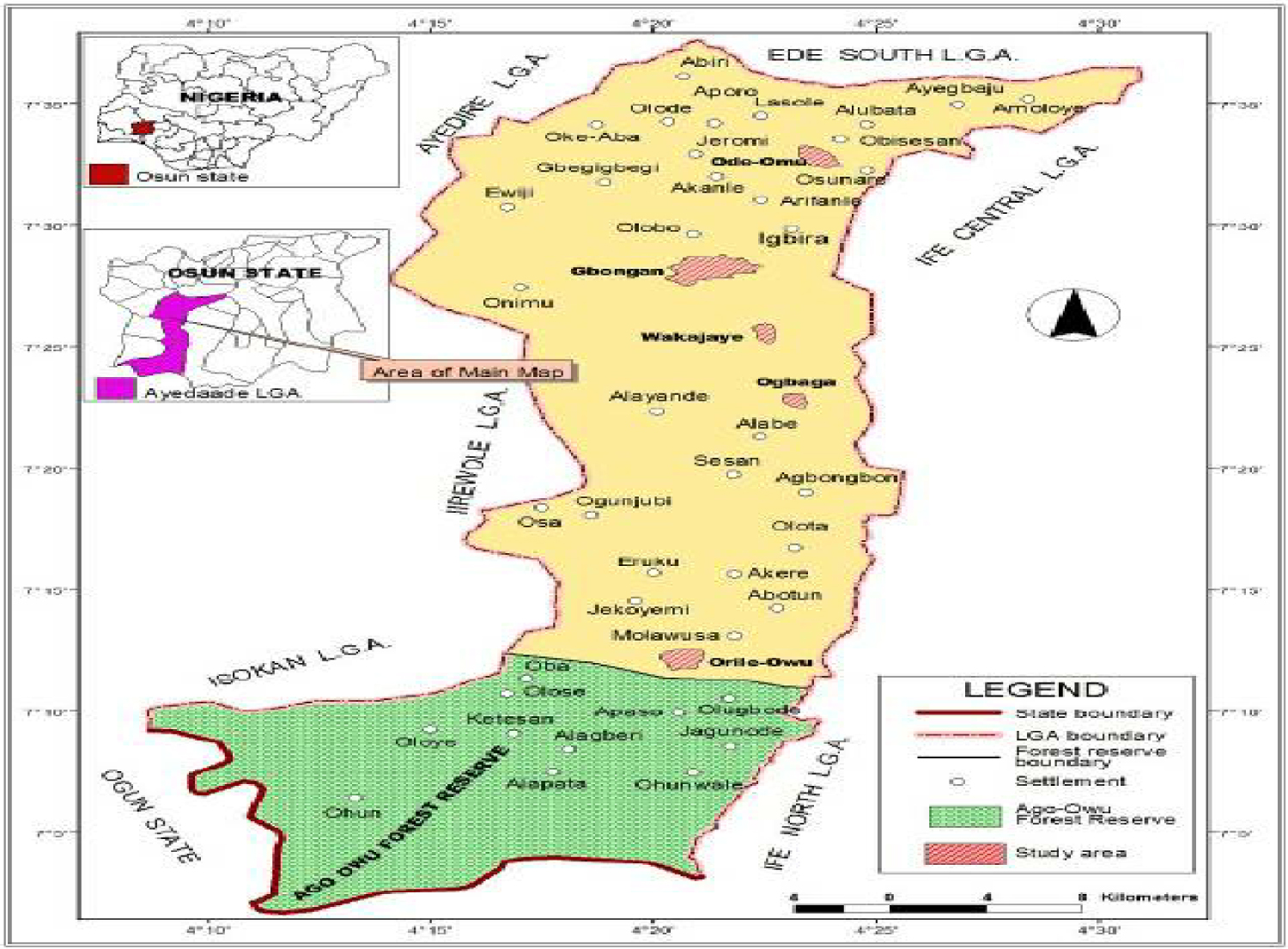 Figure 1: Map of Ayedaade LGA [20].
View Figure 1
Figure 1: Map of Ayedaade LGA [20].
View Figure 1
This was a descriptive, cross-sectional community-based study. Purposive sampling was used to select 210 adults based on the inclusion/exclusion criteria from the total villagers who voluntarily visited the temporary outpatient clinic for their health checkup. Simple random sampling was used to select 138 adults.
The sample size was estimated using the Taro Yamane formula with 95% confidence level:
, where N = community population size, e = allowable error (%)
n = 210 ÷ 1 + 210 (0.05)2 = 137.7 adults.
1. Only adults over the age of 18 years were allowed to be enrolled into the study.
2. Only permanent residents of Abimbola village were allowed to participate in the study.
1. Individuals with debilitating illnesses were not enrolled into the study.
A health check-up service by qualified trained medical and public health practitioners was conducted in a temporary out-patient clinic for a period of three days. Data were collected using standardized case forms that captured the study variables. Data obtained include socio-demographic characteristics, weight, and systolic and diastolic blood pressure. The weight was recorded in kilograms to the nearest 0.1 kg using a weighing scale.
The participants were allowed to rest at least for 15 minutes in a sitting position then blood pressure was measured using Aneroid mercury sphygmomanometer and 3 M Littmann classic II SE stethoscope. Weights of the participants were measured by an Analog weighing scale. The scale was placed on a smooth and flat surface.
Data was only obtained from case notes of selected respondents who voluntarily agreed to participate in the study and also fit the inclusion-exclusion criteria. Not all that visited the clinic participated in the study but selected participants (138) undergo all health check-up tests according to their requirements.
The data collected for the study were analyzed using the Statistical Package for Social Sciences (SPSS), version 20. Descriptive analysis was conducted to derive the frequencies and proportions the respondents' socio-demographic characteristics. Inferential statistics like the independent t-test, ANOVA and Chi-square test statistics were used to derive associations between selected variables at 0.05 level of significance. Since the blood pressure readings were taken at a cross-section, the blood pressure status of the respondents is subject to confirmation.
The recorded blood pressure values of the participants were classified into four [21];
• Normal: Systolic lower than 120 mmHg and Diastolic lower than 80 mmHg,
• Pre-hypertension: Systolic 120-139 mmHg and Diastolic 80-89 mmHg,
• Stage 1 Hypertension: Systolic 140-159 mmHg and Diastolic 90-99 mmHg,
• Stage 2 Hypertension: Systolic ≥ 160 mmHg and Diastolic ≥ 100 mmHg
The respondents suspected for hypertension were those whose blood pressure were within the Stage 1 hypertension (systolic or/and diastolic) and Stage 2 hypertension (systolic or/and diastolic) ranges.
Permission to conduct the medical outreach and report some of the findings was obtained from the village leaders and every single respondent. Verbal consent was received from each of the 138 adult respondents. The respondents were guaranteed utmost confidentiality of data; their names were excluded from all the instruments. No undue compensation was given to any of the respondents as a reward for joining the study. All the respondents were treated with dignity and respect. Ethical approval could not be obtained from a research ethics board due to three reasons: the brevity of the medical outreach, poor road accessibility from the distant village to the State capital and the long duration required to process the approval (about 3 months).
There were no laid structures for monitoring and controlling the prevalence of hypertension in the village. The village was void a functional primary health care centre and pharmacy. There was no way for the villagers to monitor their blood pressure or access drug services within the village, even at a fee. Due to how distant the community was to an urban center, accessing basic health treatment was quite hurdle.
Of the 138 participants from different households, 48 (34.8%) were males and 90 (65.2%) females. Their average age was 45.96 ± 16.89 years, the average age for males and females were 44.83 ± 18.85 and 46.56 ± 15.81 years respectively. From the total participants, 124 (89.9%) were married while 14 (10.1%) were single. The respondents' major occupations were farming 72 (52.2%), trading 36 (26.1%), and lumbering 7 (5.1%). Table 1 shows detail of the respondents' demographic characteristics.
Table 1: Socio-demographic characteristics of respondents. View Table 1
The respondents had a mean systolic blood pressure (SBP) of 122.12 ± 28.27 mmHg, while the mean diastolic blood pressure (DBP) was 70.45 ± 14.71 mmHg. Furthermore, there was a 26.8% prevalence of hypertension among the villagers, of which 43.2% of them had both hypertensive SBP and DBP. Figure 2 shows the proportion of male and female respondents within the various BP groups. The prevalence of hypertension among men was 20.8%, while the prevalence among women was 30.0%.
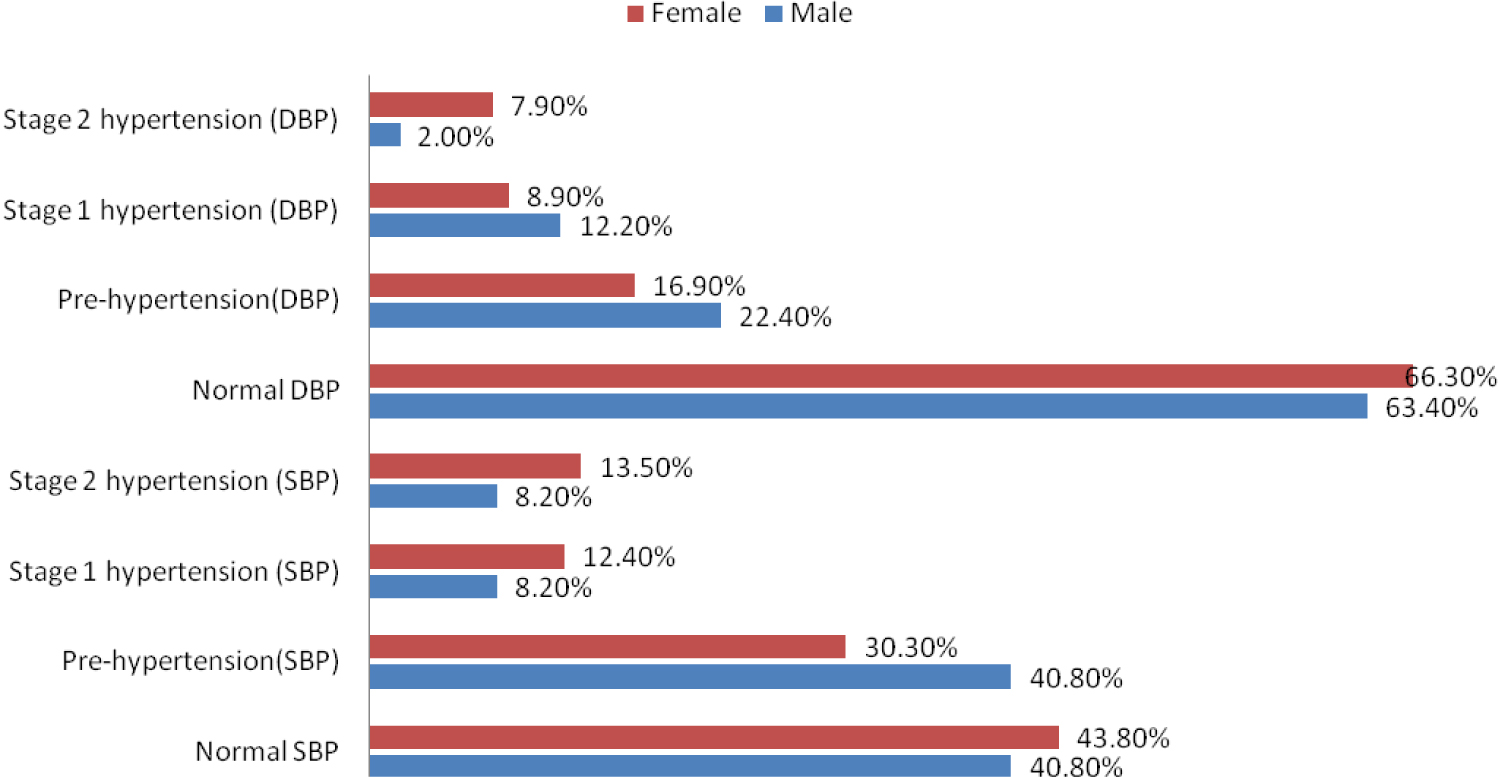 Figure 2: JNC classification of blood pressure based on respondents' sex`.
View Figure 2
Figure 2: JNC classification of blood pressure based on respondents' sex`.
View Figure 2
As shown in Figure 3; 60 (43.5%) and 90 (65.2%) of the participants had normal systolic and diastolic blood pressure respectively; 47 (34.1%) and 26 (18.1%) had pre-hypertension systolic and diastolic blood pressure respectively; 16 (11.6%) and 14 (10.1%) had Stage 1 hypertension systolic and diastolic blood pressure respectively and 16 (11.6%) and 8 (5.8%) had Stage 2 hypertension systolic and diastolic blood pressure respectively.
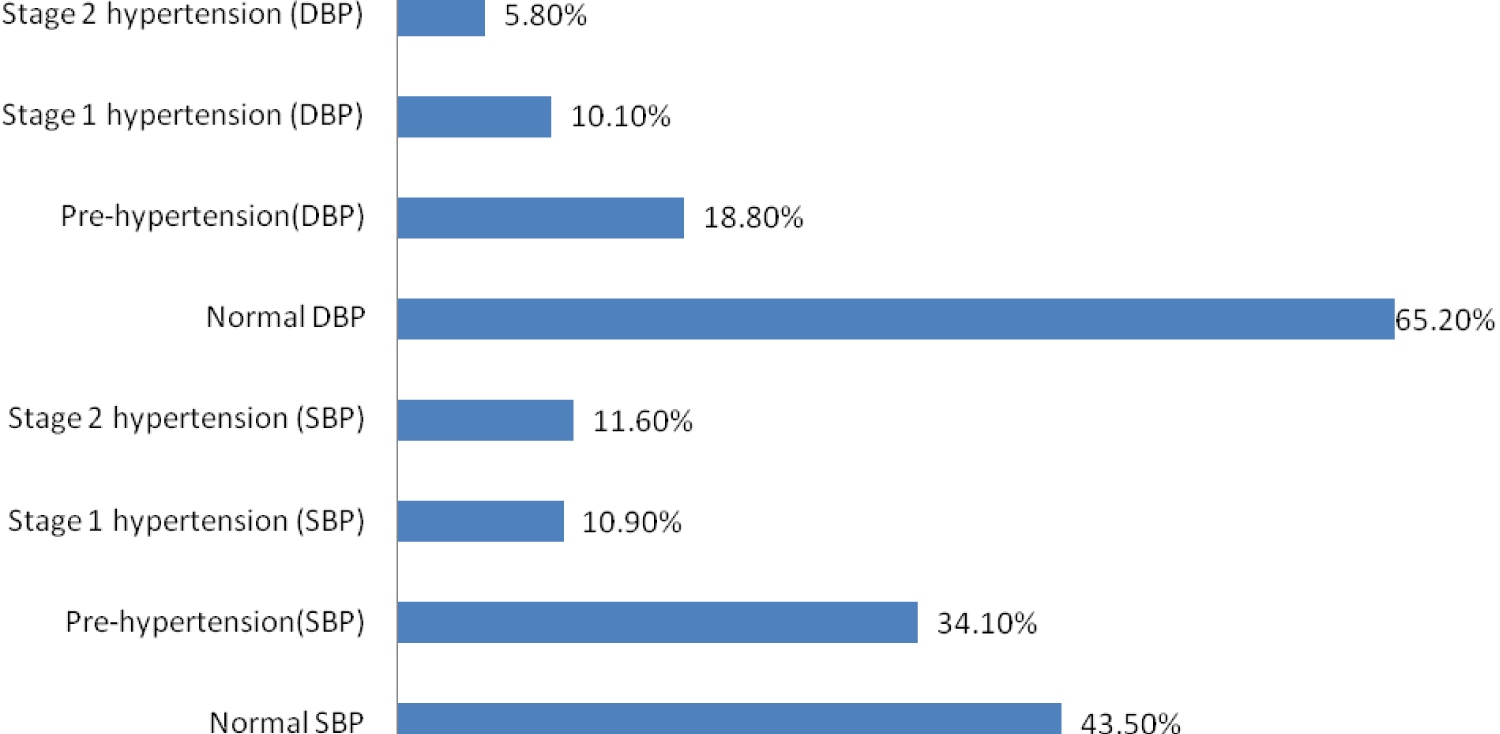 Figure 3: JNC classification of respondents' blood pressure.
View Figure 3
Figure 3: JNC classification of respondents' blood pressure.
View Figure 3
Moreover, the respondents' mean weight was 62.15 ± 12.67 Kg, with the males having a slightly higher average (63.71 ± 11.77 Kg) compared to the females (61.33 ± 13.11 Kg).
There were statistically significant associations between the respondents' age and their SBP (p = 0.000) and DBP (p = 0.021) blood pressure. Majority (74.2%) of the respondents that had Stage 1 and 2 SBP hypertension were over 50 years of age, while 22.6% were between 36 to 50 years and 3.2% were under 36 years. Details of this can be found in Table 2. The mean SBPs for respondents less than 36 years, between 36 to 50 years and over 50 years were 107.45 ± 15.25 mmHg, 120.26 ± 25.64 mmHg, and 136.73 ± 32.04 mmHg respectively, while the mean DPBs for respondents less than 36 years, between 36 to 50 years and over 50 years were 70.47 ± 12.67 mmHg, 74.96 ± 16.50 mmHg, and 70.45 ± 14.71 mmHg.
Table 2: Association between respondents' age categories and their blood pressure. View Table 2
Table 3 reveals the association between the respondents' sex and their BP. There were no statistically significant relationships between the sex of respondents and their SBP (p = 0.370) and DBP (p = 0.605). The average SBP and DBP for the male was 119.17 ± 21.91 mmHg and 69.75 ± 13.57 mmHg respectively, while the average SBP and DBP for the female 123.71 ± 31.17 mmHg 70.82 ± 15.35 mmHg respectively.
Table 3: Association between respondents' sex and their blood pressure. View Table 3
There were statistically significant differences between the respondents' marital status and their average SBP (p = 0.021) and average body weight (p = 0.002). However, there was no statistically significant difference with their average DBP (p = 0.283). The married respondents had an average SBP and DBP of 123.98 ± 28.96 mmHg and 70.90 ± 14.89 mmHg respectively, while the single respondents' average SBP and DBP were 105.71 ± 12.84 mmHg and 66.43 ± 12.77 mmHg respectively. The married respondents also had a significantly higher body weight (63.27 ± 12.74 kg) compared to the single respondents (52.29 ± 6.21 kg). Details of these associations are revealed in Table 4.
Table 4: Association between respondents' marital status and their average BP and weight. View Table 4
Table 5 provides information about the association between the respondents' occupation and their average weight and BP. There was a statistically significant difference between the respondents' occupation and their average body weight (p = 0.025). The drivers had the highest average body weight (70.00 ± 27.46 kg) while the lumbers had the least average body weight (53.008.52 kg). Average body weight for the farmers and traders were 63.85 ± 12.37 kg and 62.89 ± 12.60 kg respectively. However, there were no statistically significant associations between the respondents' occupation and their average SBP (p = 0.781) and DBP (p = 0.198). The farmers had the highest average SBP (123.94 ± 29.30 mmHg), while the lumbers had the least average SBP (111.43 ± 13.45 mmHg). Furthermore, the traders had the highest average DBP (73.47 ± 17.64 mmHg), while the drivers had the least average SBP (62.50 ± 12.58 mmHg).
Table 5: Association between respondents' occupation and their average BP and weight. View Table 5
Routine monitoring of the blood pressure is integral to early detection of hypertension and effective management of the ailment. The lack of primary health care centers or other health monitoring structures in the study location made it impossible for the locals to be aware of their health status or to manage the ailment effectively. Without proper measures in place for hypertension screening in rural areas, early diagnosis becomes a challenge [16]. There have been reports that majority of the interventions being put in place to reduce the prevalence and manage hypertension are focused on urban areas, thereby contributing to the high prevalence of hypertension being detected in the rural areas [18,19]. A survey conducted by Atinyi, et al. [19] to assess the prevalence and awareness of hypertension among rural and urban communities revealed that the rural dwellers had a higher prevalence of hypertension because they had a lower level of awareness and more limited control measures compared to the urban dwellers. Another study comparing hypertension in rural and urban communities in Madagascar revealed that hypertension was notably prevalent in both areas, however, it was significantly less treated in the rural areas due to low level of awareness and unavailability health centers or basic instruments like sphygmomanometer [22].
The 26% hypertension prevalence in the rural community is similar to a national rural prevalence of 26.4% estimated in 2014 [10]. However, more recent studies in selected rural areas have detected higher prevalence of hypertension. Prevalence as high as 44.3%, 32.8% and 44% have been reported among rural areas in Southern Nigeria [11,16,17]. The prevalence could be lower in Abimbola compared to the other study location due to their distinct cultural, social and behavioral habit. Furthermore, the higher prevalence of hypertension among women compared to men has also reported in other Nigerian rural surveys; such as a female to male prevalence of 77.7% to 24.4%, and 52.3% to 29.2% reported by Lawson and Iwasam [16] and Ofili, et al. [17]. However, several urban surveys in Nigeria have reported a higher prevalence among men; in study among adults in Ibadan North Local Government, the male adults had a prevalence of 36.8% compared to 31.1% prevalence among the female adults [12]. Another survey conducted in Lagos city, revealed the prevalence among males was 30.7% while that of females was 26.5% [13]. Moreover, the significant increase in the prevalence of hypertension with age and the higher prevalence of hypertension among married respondents was also reported by Ofili, et al. [17] and Lawson and Iwasam [16]. Age has long been identified as a risk factor for hypertension; married respondents probably have a higher prevalence of hypertension because they are older than the single respondents.
A limitation in this study was that the blood pressure readings were only collected one time due the conditions surrounding the outreach. However, as recommended by the American Heart Association, subsequent readings were collected at intervals for respondents that recorded high SBP and/or high DBP in order to verify the result [23].
It has become established that hypertension is prevalent in both rural and urban areas, with some situations of higher prevalence in the rural areas. Therefore, it is paramount for developing countries like Nigeria to begin channeling resources to these areas in a bid to effectively tackle the havoc caused by high blood pressure. The absence of screening materials as basic as sphygmomanometer in rural areas makes it impossible for blood pressure screening and monitoring. The global target of achieving a 25% deduction in the prevalence of hypertension by 2025 will be unachievable if the rural dwellers do not gain access to basic health services, instead the rural-urban health inequality gap would have widened even further.
This study just like similar studies in the past has refreshed our awareness about the prevalence of hypertension in rural communities. It is recommended that all Federal and State Governments, Non-governmental organizations, and private organizations support the Local Government by providing necessary resources required for effective health monitoring and management. Health policies must also be put in place to available antihypertensive drugs accessible and affordable to rural dwellers. Health promotion through campaigns and advocacy at grassroots level are also required to improve the health seeking behaviour of rural dwellers.
This study was supported by Living Stone Explorers, Nigeria. The authors of this research paper would like to appreciate everyone who participated in this study in one way or the other.
The authors declare no conflict of interest.