Recent guidelines have suggested combination therapy as initial treatment in hypertensive patients with ≥ grade 2 hypertension, aiming to achieve target blood pressure (BP) goal faster and more effectively. Both calcium channel blockers (CCBs) and angiotensin converting enzyme inhibitors (ACEIs) are in the list of first-line antihypertensives, however the choice of the combination therapy is left to the discretion of the clinician, and there are concerns that ACEIs are less effective in BP reduction among black hypertensives. We aimed to study the BP lowering effect after 4 weeks of treatment with Amlodipine (CCB) and Lisinopril (ACEI) each in combination with Bendroflumethiazide (thiazide diuretic) among adult hypertensive patients with ≥ grade 2 hypertension attending 3 district hospitals in Dar-es-Salaam, Tanzania.
We conducted a comparative study from November 2018 to January 2019. Eligible patients received Amlodipine/Bendroflumethiazide (5/5 mg) or Lisinopril/Bendroflumethiazide (5/5 mg) drug combinations. The primary outcome measure was the BP level after 4 weeks of treatment compared to baseline BP.
A total of 239/266 (89.8%) patients (121 Amlodipine, 118 Lisinopril) completed the study. Their mean age was 60 ± 12 years and 69% were females. The mean ± SD baseline BP was 173 ± 19/101 ± 15 mmHg for Amlodipine and 169 ± 15/101 ± 11 mmHg for Lisinopril groups, p = 0.088. After 4 weeks of treatment, the BP dropped by a mean of 43/22 mmHg and 40/22 mmHg in the Amlodipine and Lisinopril groups, respectively (p > 0.05). Overall, after 4 weeks of treatment majority (85.4%) of study participants in the total population achieved BP control (86.0% in Amlodipine, 84.7% in Lisinopril, p = 0.792).
Both Amlodipine and Lisinopril each in combination with Bendroflumethiazide showed impressive BP reductions in this cohort of native Tanzanian patients with ≥ stage 2 hypertension, and there was an insignificant difference between them. Both drug combinations can be used in the initial treatment plan when the priority is to reduce one's BP.
Hypertensive blacks, Amlodipine, Lisinopril, Blood pressure control, Sub-saharan africa, Hypertension, Combination therapy
Hypertension is a disease of public health importance worldwide, including Tanzania. In Tanzania, hypertension is present in 25.9% among 25-64 years-old adults [1], and it is an underlying cardiovascular risk factor in 14.6% and 45% of general internal medicine and cardiology patients, respectively [2,3]. Despite this, management of hypertension has been way below optimal, with as low as 5% control rate in the community [1] and 28.3% control in the hospital setting [4]. As a result, there has been an increase in recorded cardiovascular and renal complications including stroke, left ventricular hypertrophy, heart failure, chronic kidney disease and cardiovascular deaths in the country [2,3,5-7]; a trend that has also been seen in other parts of the sub Saharan Africa region [8].
To overcome this trend, better BP control remains one of the most important priorities, as it is the most significant intervention to reduce complications. However, this task is faced with many challenges including lack of simple, cheap and readily available evidence-informed drug combinations to control hypertension in the local setting. Both the Pan African Society of Cardiology and the European Society of Cardiology guidelines recommend 2-drug combinations as a starting regimen for patients with grade 2 or more hypertension; with calcium channel blockers (CCBs), angiotensin converting enzyme inhibitors/angiotensin receptor blockers (ACEIs/ARBs), beta blockers, and diuretics all in the choice list [9,10].
In Tanzania, CCBs, ACEIs/ARBs and thiazide diuretics are most common drugs prescribed as first line for hypertension. The long-acting dihydropyridines CCBs and long acting ACEIs are good choices for once-a-day dosing as they increase adherence and therefore improve patient compliance and control [11]. Both drugs have been shown to reduce systolic BP by a factor of up to -12 mmHg as monotherapy in randomized clinical trials [12-14], but some have found ACEI to be less potent than CCBs in lowering BP, especially among hypertensive blacks [15,16]. In the study by Ojji, et al. perindopril in combination with hydrochlorothiazide reduced systolic BP by a factor of -14.2 mmHg, which was less than the combination of amlodipine with hydrochlorothiazide (-17.1 mmHg) after 6 months of treatment among black hypertensives with mild to severe hypertension [15]. We aimed to study the level of BP reduction of commonly prescribed drugs in Tanzania; Lisinopril (long-acting ACEI) and Amlodipine (long acting dihydropyridine CCB), each in combination with Bendroflumethiazide (thiazide diuretic) in patients with moderate to severe hypertension being followed-up in hypertension clinics in 3 district hospitals in Dar es Salaam. Further, we wanted to compare their effectiveness in hypertension control at 2 and 4-weeks, while assessing their tolerability among patients.
This was an open-label, comparative study. The study was conducted between November 2018 and January 2019.
The study was conducted in 3 district hospitals (Temeke, Amana and Mwananyamala) in Dar es Salaam city. The hospitals serve as referral hospitals for approximately 90 lower-level health centers within Dar es Salaam. The hypertension clinics are conducted once per week in each of the hospitals and are attended by 3-4 physicians and 2 nurses. Each clinic sees an average of 50 patients on a clinic day.
Participants were hypertensive native Tanzanians attending care and treatment at these hospitals during the time of the study, and who had indications for combination therapy for their hypertension treatment. We therefore included patients who were ≥ 18 years and who had BP readings of ≥ 160 mmHg systolic and/or ≥ 100 mmHg diastolic on the day of clinic visit, and agreed to participate in the study. Both newly diagnosed and previously known hypertensives were included. We excluded the following patients; pregnant women, lactating mothers, patients known to be allergic to either of the study medications, patients with absolute contraindications to use either of the study medications, patients who were currently on ≥ 3 antihypertensive drug combinations as well as sick patients who required admission e.g. those with hypertensive urgency or emergency.
The sample size for this study was calculated using the formula for estimating sample sizes for non-inferiority comparative study design comparing two independent group means [17]. With a non-inferiority margin of 7 mmHg, sample size was obtained from the formula; Patients per group = f (α, β) × 2 × (SDP)2/(d)2. Where f (α, β) = 10.5 for 90% power with 5% significance. d = 7 mmHg which is the smallest difference in means that would be clinically meaningful [18]. Pooled standard deviation (SDP) = 15.7 mmHg. Thus, patients per group = 106 patients. Assuming an additional 10% loss to follow-up during the study, at least 234 (117 per group) patients were sufficient to bring about a representative sample. Upon fulfilling the inclusion and exclusion criteria, patients were consecutively enrolled in the study until the required sample size was achieved.
Enrolled patients received either Amlodipine/Bendroflumethiazide (5 mg/5 mg) or Lisinopril/Bendroflumethiazide (5 mg/5 mg) drug combinations allocated by means of computer-generated random numbers. After enrollment, patients were required to discontinue any of their previous antihypertensive medications and were started on the combination regime without a wash-out period. All drugs were on separate tablet formulations, stationed at the hospital pharmacy and were given freely to the study participants.
A structured questionnaire was used to record information on patients' socio-demographic and clinical characteristics, including cardiovascular risk factors' history. Information regarding previous and existing cardiovascular diseases like heart failure, chronic kidney disease, etc. was obtained from patients' hospital files.
At baseline, BP was taken by using a mercury sphygmomanometer. This was done when the patient had a 5 minutes' rest and seated comfortably in a chair with the back and left arm supported, legs uncrossed and the upper arm at the level of the right atrium. A proper cuff size was used. The first and fifth Korotkoffs' sounds were taken as systolic and diastolic BP respectively. Three measurements were taken one minute apart in the left arm and the average of the last two readings were recorded as the patient's BP. Hypertension was defined as BP of more than or equal to 140/90 mmHg, or use of antihypertensive medications and was categorized as grade 1 (140-159/90-99 mmHg), grade 2 (160-179/100-109 mmHg) and grade 3 (≥ 180/≥ 110 mmHg) according to European Society of Cardiology guidelines [10]. Only patients who were found to have BP range of grade 2 or more hypertension on the day of clinic visit were included in the study.
Height and weight were measured according to standard techniques. Body mass index (BMI) was calculated as weight in kilogram/height in meter2. Obesity was defined as BMI ≥ 30 kg/m2. Waist circumference was measured using a tape measure at the level of the umbilicus, and abdominal obesity was considered present when the waist circumference was > 102 cm and > 88 cm in men and women respectively [19].
Prescribed medications were to be taken the next morning and patients were instructed to take their medications between 7:00 am to 9:00 am. The importance to adhere to the prescribed medications was explained to patients and their caregivers as appropriate. Patients were asked to contact the investigator if they felt any adverse effects. Patients were followed up at their respective clinics in 2- and 4-weeks after initiation of the study medications. During follow-up visits, assessment of patients' adherence was done while history of any side effect was actively asked and recorded. During each follow-up visit, office BP was measured using same protocol described above, and recorded in patients' data collection forms.
The primary endpoint of this study was the mean change in office systolic and diastolic BP from baseline to 4 weeks of treatment. Secondary endpoints were: proportion of patients who achieved BP control (< 140/90 mmHg) at 2 weeks, proportion of patients who achieved BP control at 4 weeks, proportion of patients who could not achieve BP control at the end of 4 weeks, and proportion of patients who reported adverse events.
Data were analyzed using statistical package for social sciences (SPSS) software, version 23. Data is presented as mean ± SD for continuous variables and as number (%) for categorical variables. Comparison between the two treatment groups was done using χ2 test or Fisher's exact test for categorical variables as appropriate. Unpaired Student's t-test was used to compare differences in continuous variables including mean BP between treatment groups, while a two-tailed paired t-test was used to compare the within group BP change (i.e. within group comparison of baseline vs. post-treatment BP). All significance tests were two-sided, and a p-value of < 0.05 was considered to indicate a significant difference.
This study was done in accordance to the Helsinki Declaration of studies on human subjects. Ethical approvals to conduct the study were obtained from Muhimbili University of Health and Allied Sciences Research and Publications Committee and the Tanzanian National Institute for Medical Research. All participants signed an informed consent before data collection.
In total 1,100 hypertensive patients were screened, of whom 266 were found to be eligible and gave consent to participate in the study. Among these, 133 patients received Amlodipine/Bendroflumethiazide treatment (Amlodipine group) and similar number (133) received Lisinopril/Bendroflumethiazide treatment (Lisinopril group). At the end of 4 weeks 27 (10.2%) patients (12 in the Amlodipine group, 15 in the Lisinopril group) were lost to follow-up. Patients that were lost to follow up did not differ with the rest of the study patients in terms of age (mean age 61 ± 11 versus 60 ± 12 years), gender distribution, co-morbid conditions as well as mean BP level at baseline (mean Systolic BP 168 ± 17 versus 171 ± 17 mmHg), all p > 0.05.
The baseline characteristics of the study population are shown in Table 1. Patients in the two treatment groups did not significantly differ in terms of their baseline characteristics including gender distribution, age, cardiovascular risk profile, co-morbid conditions as well as baseline BP levels, all p > 0.05.
Table 1: Baseline characteristics of study patients (N = 239). View Table 1
Table 2 shows BP changes after 2 weeks of treatment. The mean systolic and diastolic BP for the Amlodipine group dropped by 29 mmHg and 16 mmHg respectively, while for Lisinopril group the corresponding drops were 27 mmHg and 16 mmHg respectively. Furthermore, after 2 weeks of treatment respectively, 37.2% and 39.8% of the patients in the Amlodipine and Lisinopril groups had their BP controlled (i.e. BP levels < 140/90 mmHg). The mean BP reductions as well as proportions of patients with controlled BP did not statistically differ between the two treatment groups, p > 0.05 for both (Table 2).
Table 2: Blood Pressure reduction and control after 2 weeks of treatment. View Table 2
Table 3 shows BP changes after 4 weeks of treatment. The mean BP continued to drop over time, and after 4 weeks the systolic BP dropped by a mean of 43 mmHg (from baseline systolic BP) in the Amlodipine group and by 40 mmHg in the Lisinopril group. The mean diastolic BP reduction was 22 mmHg for Amlodipine group and 22 mmHg in the Lisinopril group. Furthermore, after 4 weeks of treatment majority of study participants in both groups achieved BP control. BP was controlled in 104 (86.0%) patients in the Amlodipine group and in 100 (84.7%) patients in the Lisinopril group, Table 3. There were no statistically significant differences between the two treatment groups in neither the BP reduction levels nor the proportion of patients that achieved BP control at 4 weeks, all p > 0.05 (Table 3).
Table 3: Blood Pressure reduction and control after 4 weeks of treatment. View Table 3
Figure 1 shows the trends in BP reductions in the total population in comparison with the two treatment groups. In the total study population as well as in both treatment groups, the within group mean BP reductions after 4 weeks of treatment (compared to baseline) were statistically significant. For systolic BP, the mean BP in the total study population dropped from 171 mmHg to 129 at the end of 4 weeks, i.e. mean (95% CI) systolic BP reduction of 42 (40-44) mmHg, p < 0.0001. Again, in the total study population diastolic BP dropped by 22 (21-23) mmHg after 4 weeks of treatment, p < 0.0001.
By comparison, after 4 weeks of treatment, Amlodipine lowered systolic BP by 43 mmHg while Lisinopril lowered by 40 mmHg, i.e. between groups mean (95% CI) difference of 3 (1-6) mmHg, p = 0.093. Amlodipine and Lisinopril had similar reductions in diastolic BP of 22 mmHg, with a mean difference of 0.4 mmHg, p = 0.772 (Table 3 and Figure 1).
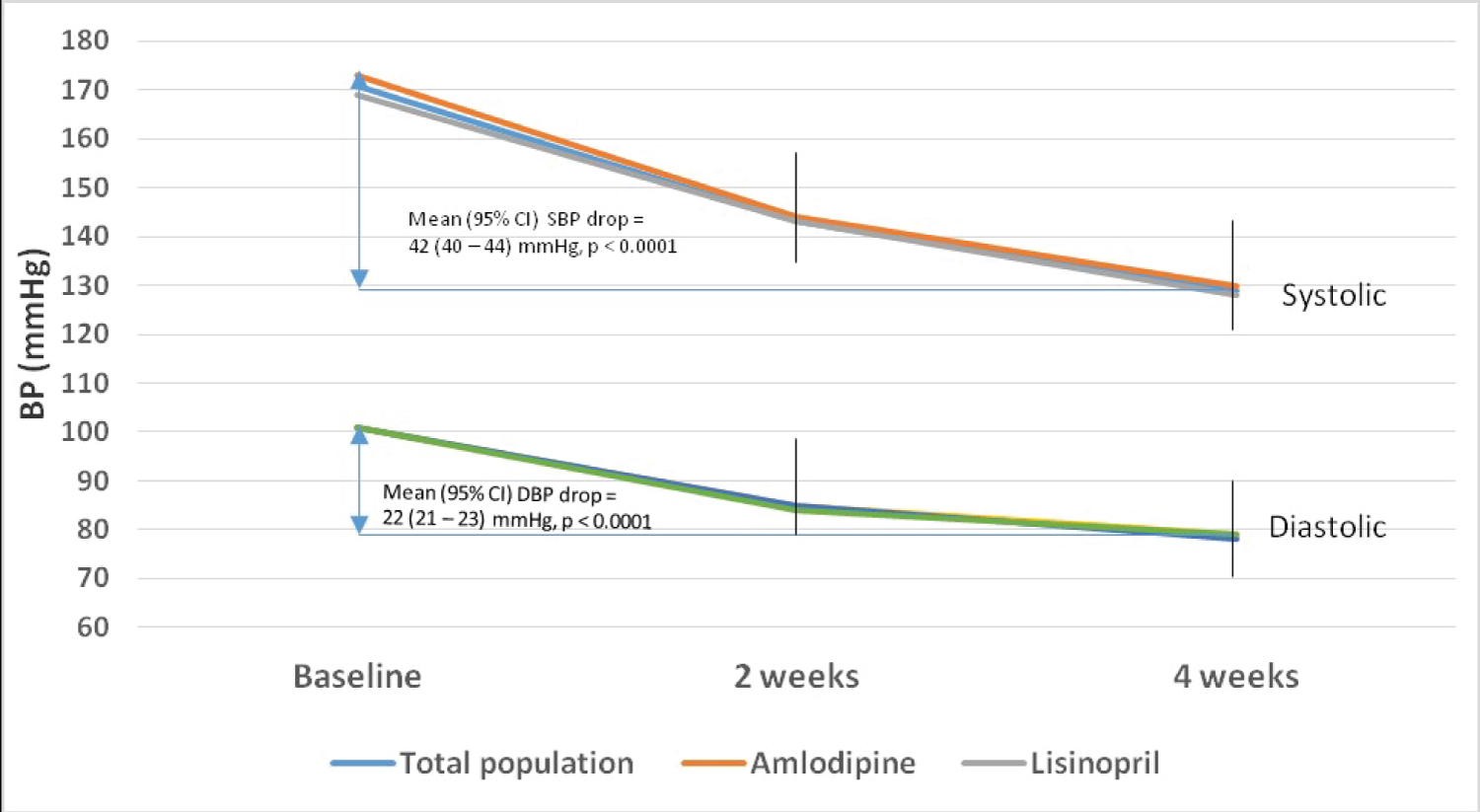 Figure 1: Trends of blood pressure reduction in the total study population and in Amlodipine and Lisinopril groups.
View Figure 1
Figure 1: Trends of blood pressure reduction in the total study population and in Amlodipine and Lisinopril groups.
View Figure 1
Figure 2 shows the proportion of patients with un-controlled hypertension during the 4 weeks of treatment. At baseline, all 239 (100%) patients had un-controlled BP. After 2 weeks of treatment, 144 (61.0%) patients were still having uncontrolled levels, i.e. BP ≥ 140/90 mmHg. In comparison, 62.8% of patients in the Amlodipine group and 59.1% of patients in the Lisinopril group had un-controlled BP at 2 weeks, an insignificant difference, p = 0.562. After 4 weeks of treatment, there were still 17 (14.0%) and 18 (15.3%) patients in the Amlodipine and Lisinopril treatment groups, respectively who continued to have uncontrolled BP levels, p = 0.792, (Figure 2).
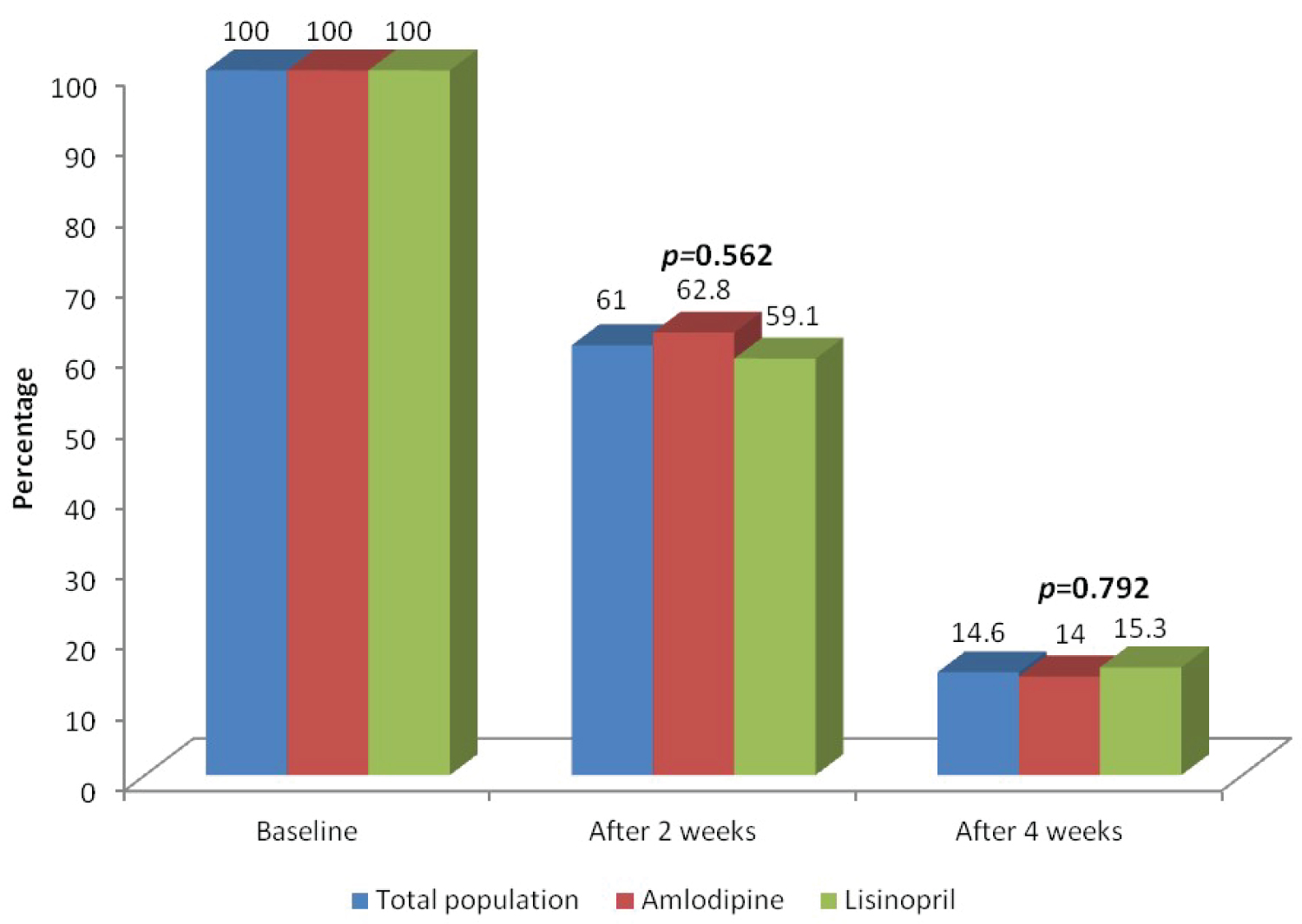 Figure 2: Proportion of patients with un-controlled BP at 2- and 4-weeks of treatment in the total study population and in Amlodipine and Lisinopril groups.
View Figure 2
Figure 2: Proportion of patients with un-controlled BP at 2- and 4-weeks of treatment in the total study population and in Amlodipine and Lisinopril groups.
View Figure 2
Table 4 shows the characteristics of patients with un-controlled BP in comparison to those who achieved control after 4 weeks of treatment. Patients whose BP was not controlled after 4 weeks of treatment had significantly higher mean systolic (189 versus 168 mmHg) and diastolic (108 versus 99 mmHg) BP at baseline when compared to patients whose BP was controlled, (p < 0.0001 for both). Furthermore, patients with un-controlled BP at 4 weeks of treatment were more likely to have previous history of heart failure (37.1%) when compared to those whose BP was controlled after treatment (14.2%), p = 0.001, (Table 4).
Table 4: Characteristics of patients with and without BP control after 4 weeks of treatment. View Table 4
Figure 3 shows the side effects reported in the two treatment groups. In total, 40 (33.9%) patients in the Lisinopril group and 10 (8.3%) in the Amlodipine group reported side effects, p < 0.0001. Headache was the most frequently experienced side effect in the Amlodipine group (5%), while dry cough was more experienced in the Lisinopril group (16.9%). All side effects were mild and did not cause withdrawal from the study or stopping taking the medications.
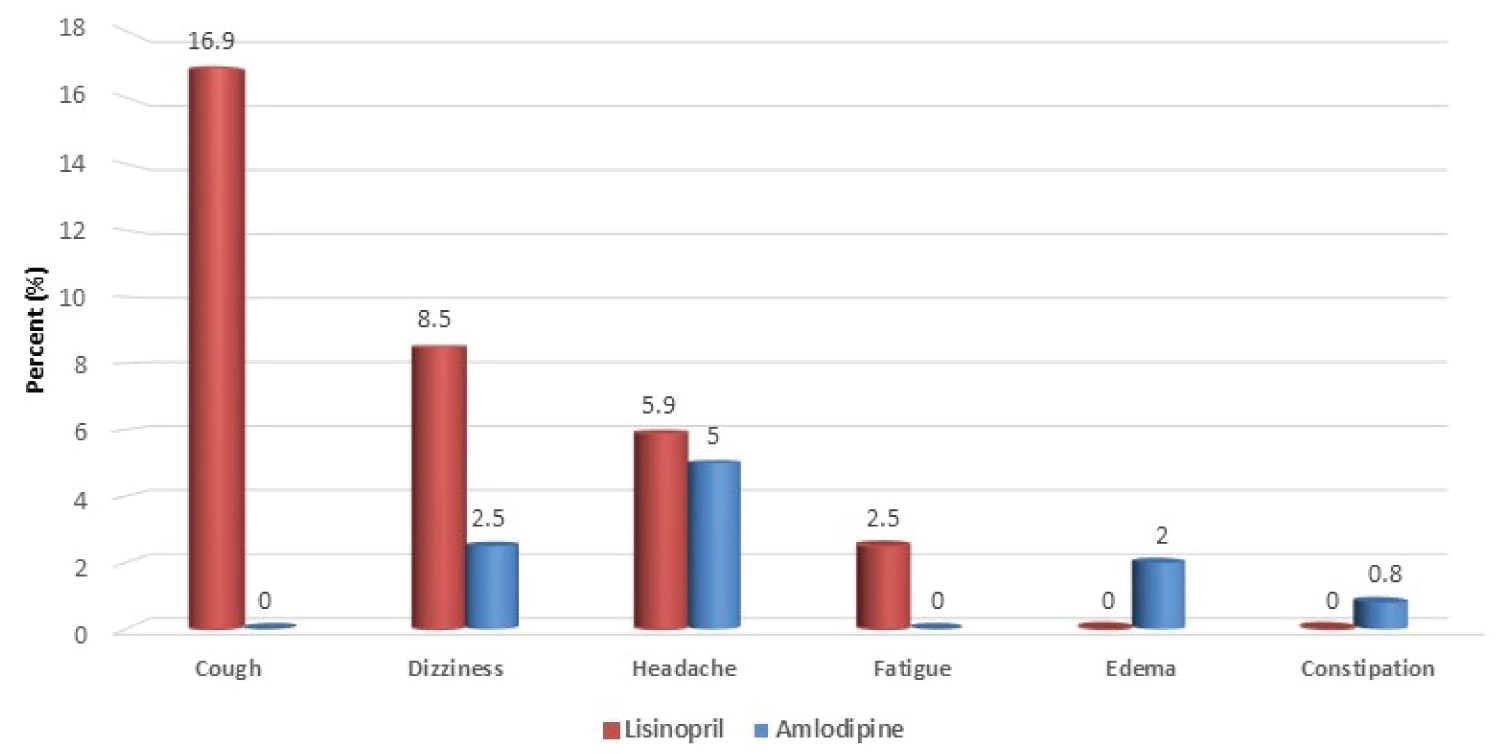 Figure 3: Side effects experienced by study patients.
View Figure 3
Figure 3: Side effects experienced by study patients.
View Figure 3
This study is among the few [15,20] to compare the efficacy of commonly prescribed antihypertensives in the sub Saharan Africa region and to the best of our knowledge, the first in Tanzania. As efforts continue to increase the performance to control BP, and within the context of many infectious and poverty-related diseases that demand priority, simple hypertension treatment protocols are highly needed in Tanzania and the sub Saharan Africa region. Our findings are therefore very important and we present a number of interesting observations, adding to the existing knowledge. Firstly, both Amlodipine and Lisinopril in combination with Bendroflumethiazide reduced the mean systolic BP by > 40 mmHg and mean diastolic BP by > 22 mmHg after 4 weeks of treatment, and there was no difference between the two drugs. Secondly, after 4 weeks of treatment both Amlodipine and Lisinopril in combination with Bendroflumethiazide resulted in BP control in > 80% of patients, and thirdly, higher baseline BP levels and pre-existing heart failure are associated with inability to control BP after 4 weeks of treatment.
We found the combination of only small and single doses of Amlodipine or Lisinopril in combination with Bendroflumethiazide to impressively lower the clinic BP in this otherwise unselected native hypertensive black population in sub Saharan Africa. The finding that both these drugs lowered BP in hypertensive patients has been well documented by previous researchers [11,12,14]. Our findings confirm the well-known observation that when combined with a diuretic, the BP lowering effect of both drugs becomes much more pronounced [21,22], even in this all-black hypertensive population. This finding underscores the importance of dual antihypertensives in patients with grade 2 or more hypertension, as recommended by guidelines [9,10]. The finding that Amlodipine and Lisinopril showed no difference in their efficacy in BP reduction is similar to findings from several studies [13,16], including the large ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial) study which involved > 30,000 hypertensives in North America [14], as well as in a sub analysis that included only black hypertensives in the same cohort [23]. In sub Saharan Africa where majority of patients are black, our findings are clinically important, as several previous studies have reported low efficacy of ACEIs in BP reduction among black hypertensives [15,24,25]. However, our findings suggest that when the target is to lower the BP, both Lisinopril and Amlodipine in combination with Bendroflumethiazide are similar, at least in the first 4 weeks of treatment. In addition to lowering BP, ACEIs or ARBs are recommended by different treatment guidelines and algorithms such as those for BP control in patients with chronic kidney disease and diabetes [26,27], therefore these drugs are still indicated as first line among hypertensive blacks with such conditions. Although the treatment time was shorter in our study, the resulted mean BP reductions were more than that reported by Ojji, et al. in hypertensive blacks in sub Saharan Africa [15]. The difference is likely due to the fact that they included any patient with uncontrolled hypertension including those with mild hypertension, which could have resulted in less drop of BP, as the higher the baseline BP the more likely the higher the drop in BP. All in all, guidelines recommend 2-drug combinations in patients with grade 2 or more hypertension and our study is more relevant in this context.
One of the major challenges facing hypertension management globally, and particularly in low and middle income countries of sub Saharan Africa is lack of effective and long-term control of BP to prevent complications [28]. We found in this study that majority (> 80%) of previously stage 2 or more hypertensives achieved BP control after a simple, low dose and readily available drug combination. This is clinically very relevant as it means without selection, if any of these regimes is given to patients with hypertension stage 2 or more, > 80% would be controlled at 4 weeks, provided that they regularly take their medications. In public health perspective, ideally BP can be controlled in most people, and improving hypertension treatment can be achieved by existing health systems through the use of inexpensive, once daily medications [29]. Of note, both Amlodipine and Lisinopril are available as generic medications in Tanzania and each cost around 3 USD for 30-day prescription, while Bendroflumethiazide is the cheapest (3USD per 3-months' prescription) and the first recommended thiazide diuretic in the Tanzania drug list [30]. The control rate seen in this study is much more than that reported by investigators in the ALLHAT study as well as in the study of Africans in 6 sub Saharan African countries by Ojji, et al. [14,15]. In the ALLHAT study, the control rate was 50% in year 1 and 60% in year 5, with even lesser BP control among black hypertensives in that study [14]. Although the study by Ojji, et al. had many similarities with ours, BP control after 2 months of treatment was present in around 50% of the patients; less than what was found after 1 month in this study. Several factors including level of co-morbidities could have played a role in the differences seen. The achieved control rate in this study is however very similar to the study by Weinberger, et al. which demonstrated an 80% BP control among mild to moderate hypertensive patients in the US [31]. Due to the high achieved control rate in our study participants, the current findings could be revealing an obscured reason for uncontrolled hypertension in clinics within Tanzania and maybe many other sub Saharan African countries; a reason that is not related to the types or dose of drugs being prescribed, but rather due to lack of consistent and regular medications intake. Further research is needed to understand the underlying reasons for the reported high rates of uncontrolled hypertension in our settings, looking at our health care delivery systems, the prescribers as well as issues to do with patients themselves.
When treating patients with hypertension it is important to note the hard-to-control patients, including identifying patients likely to have resistant hypertension. In our study, patients with pre-existing heart failure and those with baseline severe hypertension were unlikely to be controlled at 4 weeks of treatment. This finding has been reported by previous investigators [32-34]. In the study by Smith, et al. [34] heart failure and black race had 73% and 63% more likelihood to have resistant hypertension, and patients with resistant hypertension had higher risk of adverse outcomes including all-cause death. In our cohort, it is likely that stepping up the dose of amlodipine and lisinopril would further increase the number of patients that will achieve BP control, as found from previous research [35,36]. Of note, there was room to step up both drugs as both were started at low doses. The overall reported side effects seen in this study is slightly higher (20.9%) than that reported by Ojji, et al. (14.6%) [15], possibly due to the active inquiring for this information on our side. However, unlike in the study by Ojji, et al. there was no any drug discontinuation as a result of side effects in our study patients, indicating mild side effects. Although our prevalence of dry cough of 16.9% is within the reported prevalence in literature [37], this effect is relatively high and may offset the benefits obtained in lowering BP, since if the cough becomes persistent, lisinopril has to be stopped and changed to an ARB or another drug class.
Both Amlodipine/Bendroflumethiazide (5/5 mg) and Lisinopril/Bendroflumethiazide (5/5 mg) drug combinations are effective in lowering BP to control levels in over 80% of hypertensives in this cohort of native Tanzanian patients with ≥ stage 2 hypertension, and there was an insignificant difference between them. Both drugs can be used in the initial treatment plan when the priority is to reduce one's BP. Further studies are needed to repeat and observe these findings in a longer follow-up, especially in relation to patients' compliance.
This study is limited in a number of ways, including that we did not perform laboratory investigations as part of the study and we therefore cannot comment on the effect of the medications on patients' electrolytes, cholesterol or blood glucose levels. Also, the follow-up time was short and we cannot comment on the levels of BP or unwanted effects after 4 weeks of treatment. Although the doses of patients with uncontrolled BP at 4 weeks were increased by the attending Physicians, this was outside the study and we did not include the effect of this dose increase on BP response beyond 4 weeks of treatment.
We would like to thank Management and Staff at Temeke, Amana and Mwananyamala Hospitals for their permission, cooperation and assistance in conducting this study. Our sincere appreciation goes to all participants for agreeing to take part in this study.
All three authors (RA, PC and AK) conceived and designed the study, and participated in data analysis. RA conducted data collection. All authors participated in developing the manuscript and approved the final version.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interests.