Intradialysis hypotension (IDH) is the most common complication during hemodialysis procedure. Midodrine, an oral α-1 adrenergic agonist, is commonly used to prevent IDH. However, limited data is available to demonstrate midodrine effectiveness in prevention of IDH in high-risk hemodialysis patients.
To evaluate the effectiveness of using midodrine in patients receiving hemodialysis concerning the incidence of IDH. Also, we aimed to explore the appropriate dose for midodrine use to prevent IDH.
A retrospective cohort of adult with end-stage-renal failure.
Medical and pharmacy data used in this study was retrieved from electronic health records for adult patients with end-stage renal disease on hemodialysis.
Midodrine.
IDH was defined as a decline in systolic blood pressure (SBP) by ≥ 20 mmHg or a decline in mean arterial pressure (MAP) by ≥ 10 mmHg during hemodialysis session. Recurrent IDH was defined as three or more episodes of IDH throughout a year.
A descriptive analysis of the frequency of IDH and recurrent IDH. We also, compared the risk of recurrent IDH across various doses of midodrine use.
From a total of 68-screened patients' charts, 45 patients were included in the final analysis. 41.8% (n = 28) of the study population had an IDH that required additional interventions to restore the SBP and MAP. IDH occurred in 68% (n = 19) of patients with hypoalbuminemia (P = 0.03). Recurrent IDH occurred in 36% (n = 16) of the patients over their hemodialysis procedure. Incidence of IDH (57%, p = 0.02) and recurrent IDH (36%, p = 0.04) were statistically significant in patients who received midodrine three time per week (57%) in comparison to those who received more than three days per week.
This exploratory study shows that a considerable proportion of patients receiving midodrine did not develop IDH or recurrent IDH. A long-term follow-up study with larger number of patients in comparison to the control group would be useful to evaluate the magnitude of efficacy of midodrine in hemodialysis patients with high risk for IDH.
Midodrine, Hemodialysis, Hypotension, Blood pressure, Intradialysis hypotension, Dialysis
IDH: Intradialytic Hypotension; SBP: Systolic Blood Pressure; MAP: Mean Arterial Pressure; BID: Twice a Day; TID: Three Times a Day
Intradialytic hypotension (IDH) is the most common complication that is well recognized during hemodialysis, it occurs in around 15% to 50% of hemodialysis patients [1]. IDH is associated with a negative impact on health-related quality of life: Because it requires an early termination of the hemodialysis session causing insufficient fluid removal, then increasing the cardiovascular morbidity and mortality [2]. The pathogenesis mechanism of IDH is very complex, but mainly results from an excessive rate of fluid removal than that required for achieving a rate for intravascular filling, which ends in causing an intravascular volume depletion [3].
There is no consensus definition of IDH, however, according to the Kidney Disease Outcomes Quality Initiative and European Best Practice Guidelines, IDH is defined as a decline in SBP ≥ 20 mmHg or a decrease in a MAP by 10 mmHg and associated with clinical events like abdominal pain, nausea, vomiting, muscle cramps, dizziness, fatigue, and restlessness [4,5]. Major factors that contribute to IDH are older age ≥ 65 years, female gender, pre-dialysis systolic blood pressure < 100 mmHg, presence of diabetes mellitus, cardiovascular disease, using a peripheral vasodilator or short-acting antihypertensive medication(s), anemia, uremic syndrome, autonomic or neuropathy dysfunction, hypoalbuminemia or poor nutritional status, higher dialysate temperature, or higher ultrafiltration volume [5,6].
There are numerous therapeutic strategies that have been used to manage IDH with varied degrees of success, including placing the patient in the trendelenburg position, decreasing ultrafiltration rate, elevating dialysate calcium level, using bicarbonate-based dialysate, and giving boluses of intravenous fluids like isotonic saline and colloid solutions [4,5,7]. The third-line approach to manage and prevent IDH is using a pharmacological intervention including: Midodrine, Carnitine, or Sertraline [4,5,8].
Midodrine is an oral α-1 adrenergic agonist pro-drug with an active metabolite desglymidodrine that increases arteriolar and venous tone which causes a rise in standing, sitting, and supine systolic and diastolic blood pressure [9]. It is effectively cleared by the hemodialysis with reducing in half-life to 1.4 hour in hemodialysis patient [10].
The best data are from systematic review of 10 literatures revealing that using 2.5 to 10 mg of midodrine given 15-30 minutes before the dialysis was elevated the post-dialysis SBP and DBP by 12.4 mmHg and 7.3 mmHg above the values in controls, respectively, and the nadir SBP and DBP were higher by 13.3 mmHg and 5.9 mmHg compared with the control group, respectively [11]. Midodrine (5 mg twice daily) showed a significant increase in MAP among hemodialysis patients with chronic hypotension secondary to autonomic dysfunction as well [12].
Management of patients with high risk of IDH usually requires several of modalities to prevent IDH. However, more clinical studies are needed to validate the efficacy of one approach over any other. [5]. The objective of this study is to evaluate the effectiveness of midodrine for prevention of IDH in high-risk hemodialysis patients.
A descriptive retrospective cohort study was approved by the Institutional Review Board in January 2018. It was conducted at a tertiary care center in Riyadh.
The medical and pharmacy data used in this study was retrieved from electronic health records for adult patients with end-stage renal disease on hemodialysis who were placed on midodrine for at least one month. Patients were excluded if they were on peritoneal dialysis or if they were on hemodialysis for less than three months. Moreover, patients were excluded if they had begun midodrine in the first 90 days of dialysis.
IDH was defined as a decline in SBP by ≥ 20 mmHg or a decline in MAP by ≥ 10 mmHg [5]. Recurrent IDH was defined as three or more episodes of IDH [6]. The risk factors that contributed to IDH were identified through the following variables: patient's age, gender, body mass index (BMI) [13], presence of diabetes mellitus, cardiovascular disease, iron deficiency anemia [14], hypoalbuminemia [8], neuropathy dysfunction, and uremic syndrome which is defined as a presence of nausea, vomiting, volume overload, hyperkalemia, severe acidosis and altered in mental status. Anti-hypertension (Anti-HTN) medications were discontinued 24 hours before the hemodialysis session in patients with regular used of them. Dose and frequency of midodrine were recorded for each hemodialysis session. For the statistical purpose and due to small number of sample size, midoddrine doses were classified into three groups, 19 patients were received 2.5 mg to < 5 mg, 37 patients were received 5 mg, and 38 patients were received > 5 mg of midodrine. For the midodrine frequency, it was classified into two groups. First group included patients who received midodrine for only 3 days per week, and the second group of patients administered midodrine in daily basic. Eligible patients were followed up for at least one year.
Statistical analyses were performed by using SPSS 19.0 software (IBM, NY, USA). Categorical data was expressed as percentage and analyzed with chi-square test. Continuous data was expressed as mean ± SD and compared by the Student's t-test. All statistical assessments was 2-tailed and the level of significance was set to be at p = 0.05. Multiple logistic regressions were applied to find the association between using midodrine with the multiple independent variables such as SBP and DBP, IDH, and IDH recurrence.
From a total 68 patients' charts were screened, 23 were excluded due to insufficient patients information (n = 7), patients were on peritoneal dialysis (n = 2), and 14 patients were excluded due to loss of follow up. The remaining 45 patients were eligible for the final analysis (Figure 1).
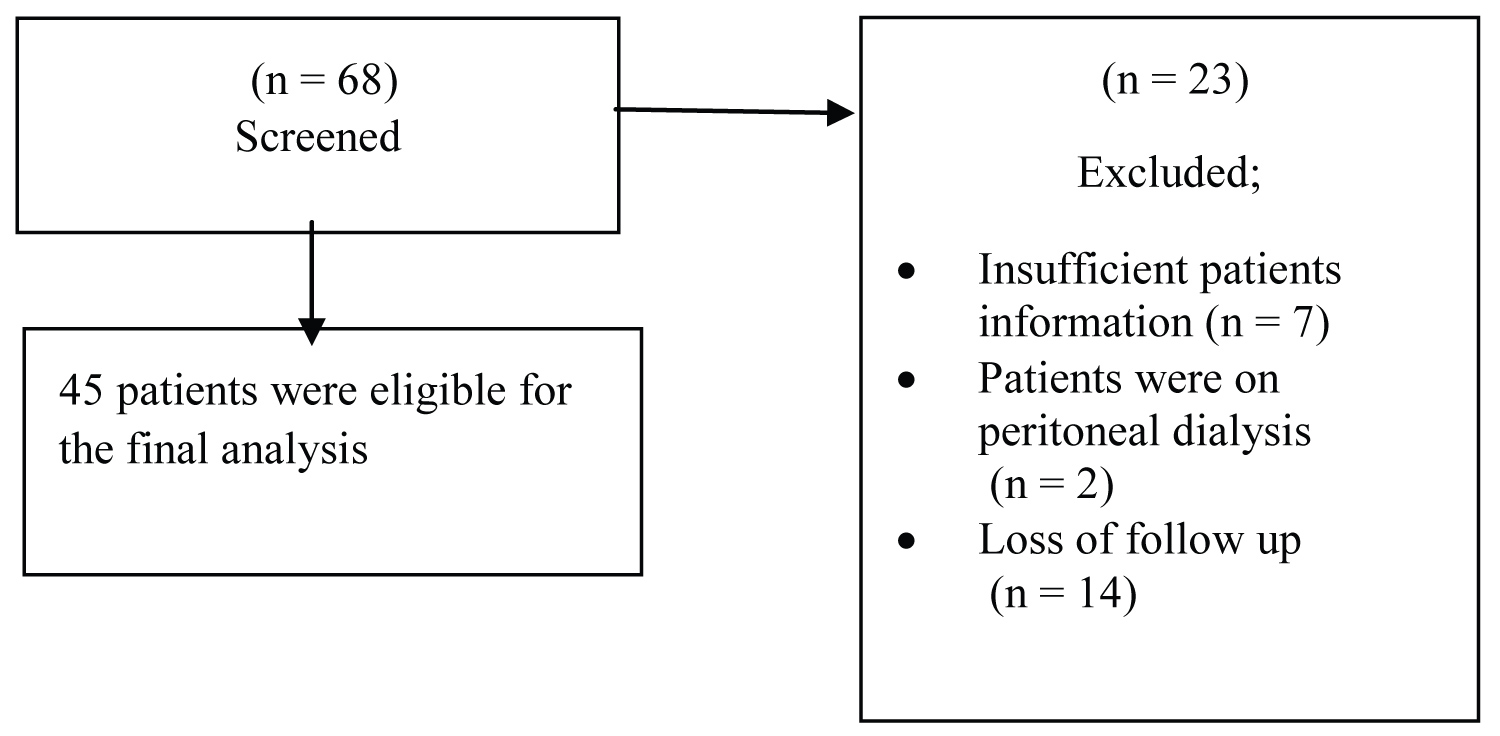 Figure 1: Flow chart of profile of patients enrolled in the study cohort.
View Figure 1
Figure 1: Flow chart of profile of patients enrolled in the study cohort.
View Figure 1
All the enrolled patients were on chronic hemodialysis for more than three months and they received a conventional hemodialysis treatment with an average time three to four hours per session, three times a week on a fixed schedule, except in three patients were received an extended-hours hemodialysis with an average treatment time per session seven to eight hours, three times a week on a fixed schedule. The hemodialysis sessions were carried on in outpatient and inpatient setting, and the maximum ultrafiltration rate was 10 ml/kg/hour and the total volume of fluid removed was 0.5 to 3 litters. The majority of the included patients had combined risk factors of IDH (Table 1); the mean age of included patients was 63-years-old, 51% of them had an age > 65-years-old (n = 23), and 53.3% were female (n = 24). Around 40% of them had normal BMI (n = 18), and 16 patients were on anti-HTN medications that were discontinued 24 hours before the hemodialysis session (35.6%). The mean pre-dialysis blood pressure reading was 112 for the SBP, 54 for the DBP, and 74 of MAP. Pre-dialysis SBP < 100 mmHg was recorded in 37 patients (82.2%). About 27 patients had diabetes mellitus (60%), 30 patients had cardiovascular diseases (66.7%), and 41 patients had an anemia disease (91.1%).
Table 1: Patient demographics data. View Table 1
Overall, IDH was recorded in 28 hemodialysis patients (41.8%) and they were required an additional interventions to restore SBP and MAP, such as placing the patient in trendelenburg position, decreasing the hemodialysis ultrafiltration rate, giving boluses of intravenous 0.9% normal saline or 20% Human albumin solutions, or they were needed an early termination of hemodialysis session. In term of recurrent IDH, it was occurred in 16 hemodialysis patients (36%). The incidence of IDH and recurrent IDH were significant in patients who had hypoalbuminemia [P = 0.03, P = 0.01] respectively. Other risk factors had an impact on SBP and MAP during the hemodialysis session. However, their effects were insignificant (Table 2).
Table 2: Relationship between IDH, recurrent IDH, and presence of IDH risk factors. View Table 2
The incidence of IDH and recurrent IDH were statistically significant in patients who received midodrine three time per week in comparison to those who received midodrine in a daily basic (57%, p = 0.02) for IDH; and (36%, p = 0.04) for recurrent IDH, (Figure 2A and Figure 2B).
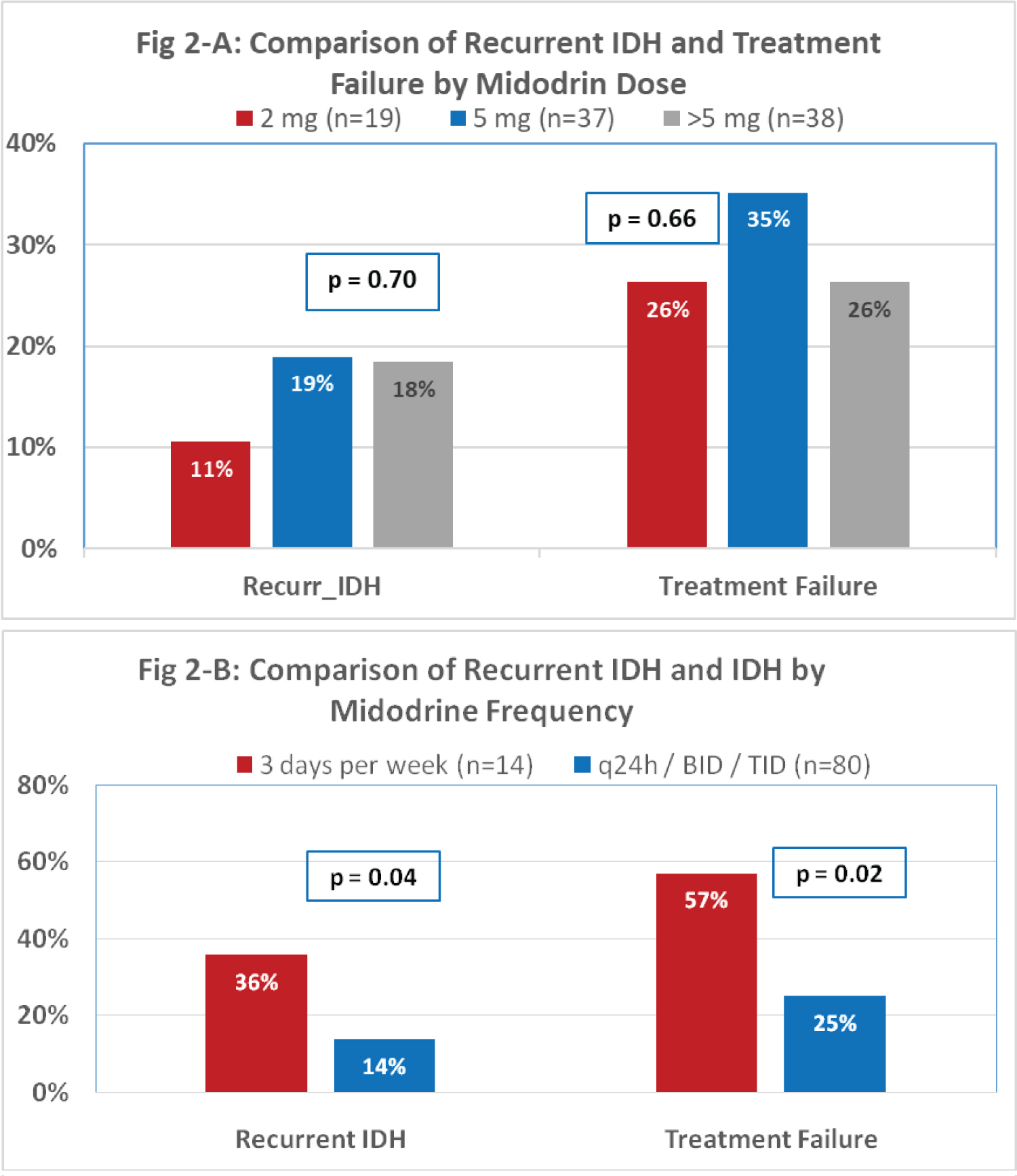 Figure 2: (A) Comparison of recurrent IDH and treatement failure by midodrine dose; (2B) Comparison of recurrent IDH and IDH by midodrine frequency.
Figure 2: (A) Comparison of recurrent IDH and treatement failure by midodrine dose; (2B) Comparison of recurrent IDH and IDH by midodrine frequency.
BID: Twice a day; TID: Three times a day
View Figure 2
The death event was reported in 23 patients (51.1%), however, the cause of death most likely related to the patient's condition like septic shock (n = 9), respiratory distress syndrome (n = 1), cardiac arrest (n = 2), septic shock with hypotension (n = 9), distress syndrome with cardiac arrest (n = 1), and septic shock with heart failure (n = 1).
IDH is the most frequently adverse event that reported during hemodialysis procedure. In recent meta-analysis was published in 2019, that included 4 studies, showed the prevalence of IDH was 10.1% based on the European Best Practice Guideline (EBPG) definition, and 11.6% based on the Nadir < 90 mmHg definition [15].
Midodrine seems to be gaining favor as a strategy to aid in management and prevention of IDH [9,10]. Midodrine and cool dialysate therapies are the most approaches that have been used [16-19]. It is worth remark the beneficial effects of midodrine in the treatment and prevention of recurrent IDH by adjusting the dialysate composition and reducing the ultrafiltration rate continuously throughout the procedure to assist the vascular refilling. In addition to the correction of the modifiable risk factors of IDH [20-24]. Serum albumin is a marker of nutrition, inflammation, and prediction of mortality. In our study, the majority of patients had hypoalbuminemia which is could be attributed to the combined effects of insufficient dietary protein intake, and co-morbid conditions like cardiovascular disease [25].
Pharmacokinetics of midodrine is changing in hemodialysis patients. Reducing half-life of midodrine in hemodialysis patients could be given a plausible explanation about the significant IDH in patients who received midodrine 3 days per week in comparison to patients administered midodrine in a daily basis.
Interestingly, in 2010 the U.S. Food and Drug Administration proposed to withdrawal approval of midodrine due to lack of post-marketing studies to predict the clinical outcome of midodrine rather than just improved the hemodynamic parameters. The proposed withdrawal attained disagreement from the American Society of Nephrology, then FDA came to an agreement to remain FDA-approved on the market in the meantime until pharmaceutical company would conduct two clinical trials to verify a clinical benefit of midodrine [26,27].
In 2018, there is a published cohort interventional study that assessed the associations between midodrine use and a variety of clinical outcomes, midodrine use was associated with the higher rates of death, adjusted incidence rate ratio IRR (95% CI) 1.37 (1.15-1.62), all-cause hospitalization 1.31 (1.19-1.43) and cardiovascular hospitalization 1.41 (1.17-1.71) in comparison to the control group. Although the results influenced by confounders, it might support FDA argument about the clinical outcome of midodrine [28].
The strength of our study that we included larger sample sizes in comparison to the previous studies were they ranged from 6 to 21 patients. The limitation of our study is that we did not have a comparison group.
Our results suggest that receiving of midodrine is significantly decreasing the IDH episode. Well randomized controlled trial that focus on important clinical outcomes such as cardiovascular events and mortality with midodrine is warranted.
The authors declare that they have no competing interests.
The study protocol was approved by the King Abdullah International Medical Research Center.
Not applicable.
The dataset used for the study is available without patient identifiers from the corresponding author on reasonable request.
The authors declare that they have no competing interests.
This study was not supported any funding.
SH, ME, MA, YR, & RB conceived and designed the study, supervised the overall execution of the study. SH & MD collected the data, cleaned the database. SH analyzed and interpreted the data. SH & MD wrote the manuscript.
The authors would like to thank Dr. Aamir Omair from the College of Medicine in King Saud bin Abdulaziz University for Health Sciences for his invaluable help in doing the analysis.