Objective: Descriptive study focused on SARS-COV-2 exposed neonates admitted to a tertiary center Neonatal Intensive Care Unit (NICU).
Study design: Longitudinal cohort retrospective study of neonates admitted to a tertiary center NICU during March to August 2020. Key indices (risk factors) are described for exposed neonates in order to draw conclusions for preventive strategies.
Findings: There were 459 deliveries during the study period. 177(12%) mothers tested positive for SARS-CoV-2 with 184 SARS-COV-2 exposed (exposed) neonates born to these mothers. Sixty exposed neonates (33%) were admitted to the NICU. Exposure was associated with prematurity (55%) and Low birth weight (40%). There were a high proportion of twin births in the cohort (23%). In comparison to exposed neonates who roomed in with their mothers, NICU neonates were four times (3.3% versus 0.8% respectively) more likely to test positive for SARS-COV-2. Exposed neonates were more likely to be born to women on public insurance, a measure of low socio-economic status.
Conclusion: Maternal COVID-19, is associated with preterm births, and low birth weight. Infants of women on public insurance were more likely to be exposed. COVID preventive measures targeting pregnant women including vaccination will help protect newborns. Women on public insurance may require targeted outreach efforts to promote equitable uptake of preventive measures including COVID-19 vaccine. More studies are needed to define long term effect on exposed infants especially those with potentially synergistic risk factors like prematurity and low birth weight.
Maternal COVID, COVID-19, Neonates, Newborn, SARS-COV-2 newborn exposure
Corona virus disease (COVID-19) that is caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused a global pandemic affecting all age groups [1]. Data and outcomes regarding neonates are variable and constantly evolving. Though SARS-CoV-2 primarily affects the adult population, as seen by numbers and severity, neonates form a highly vulnerable group due to potential synergistic effects of the immature immune system as well as disruption of bonding and maternal adjustments to post-delivery life [2]. Our study's uniqueness is its focus on neonates admitted to the NICU, a highly vulnerable population at risks for potential synergistic effects of exposure to serious viral diseases during pregnancy [3]. Our study highlights some of the complications of SARS-COV-2 on newborns and agrees with other studies that pregnant women could benefit from targeted preventive policies and programs with specific focus on low-income women.
We identified all neonates born between March 15 and August 31, 2020. The period was selected because it represented the first period (first surge) for our healthcare system SARS-COV-2 testing positivity rates from a high of 75.5% (March) to a nadir of < 5% (August), indicating the end of the first surge period.
We reviewed demographic and clinical information for all neonates and medical records information for those neonates born to mothers who tested positive for SARS-CoV-2 from a nasopharyngeal swab sample at the time of delivery. Universal screening of all pregnant women in labor began on April 11, 2020 at our institution to identify symptomatic and asymptomatic maternal COVID, in order to guide infection control processes and procedures during labor and to protect the newborn from infection. Prior to this time, testing was only done on women who were symptomatic.
Demographic, epidemiologic, and clinical data were reviewed as well as maternal delivery history and SARS-COV-2 status at delivery.
Testing for SARS-CoV-2 was done by use of real-time reverse transcription polymerase chain reaction (rt-PCR; BioGX SARS-CoV-2 BD MAX™ kit [Becton, Dickinson, MD, USA]. Testing for SARS-CoV-2 by rtPCR was done on 2 [nasopharyngeal and oro-pharyngeal] swab samples at 24 hours for 11 neonates and 2 or more samples > 24 hours apart for 44 neonates. Differences in sampling trends reflected change in testing protocol for de-isolation considerations, since initially all exposed neonates were isolated until discharge. This study was approved by our institutional review board as exempt from consent.
During our study period, there were 1459 deliveries with 177 (12%) maternal COVID. One hundred and eighty-four neonates were born to these mothers (including 7 set of twins). Of these, 60 (32.4%) exposed neonates were admitted to the NICU. Table 1 shows selected demographic and clinical characteristics of exposed neonates during the study period. In comparison to exposed neonates who roomed in with their mothers, NICU neonates were four times (3.3% versus 0.8% respectively) more likely to test positive for SARS-COV-2 (Figure 1).
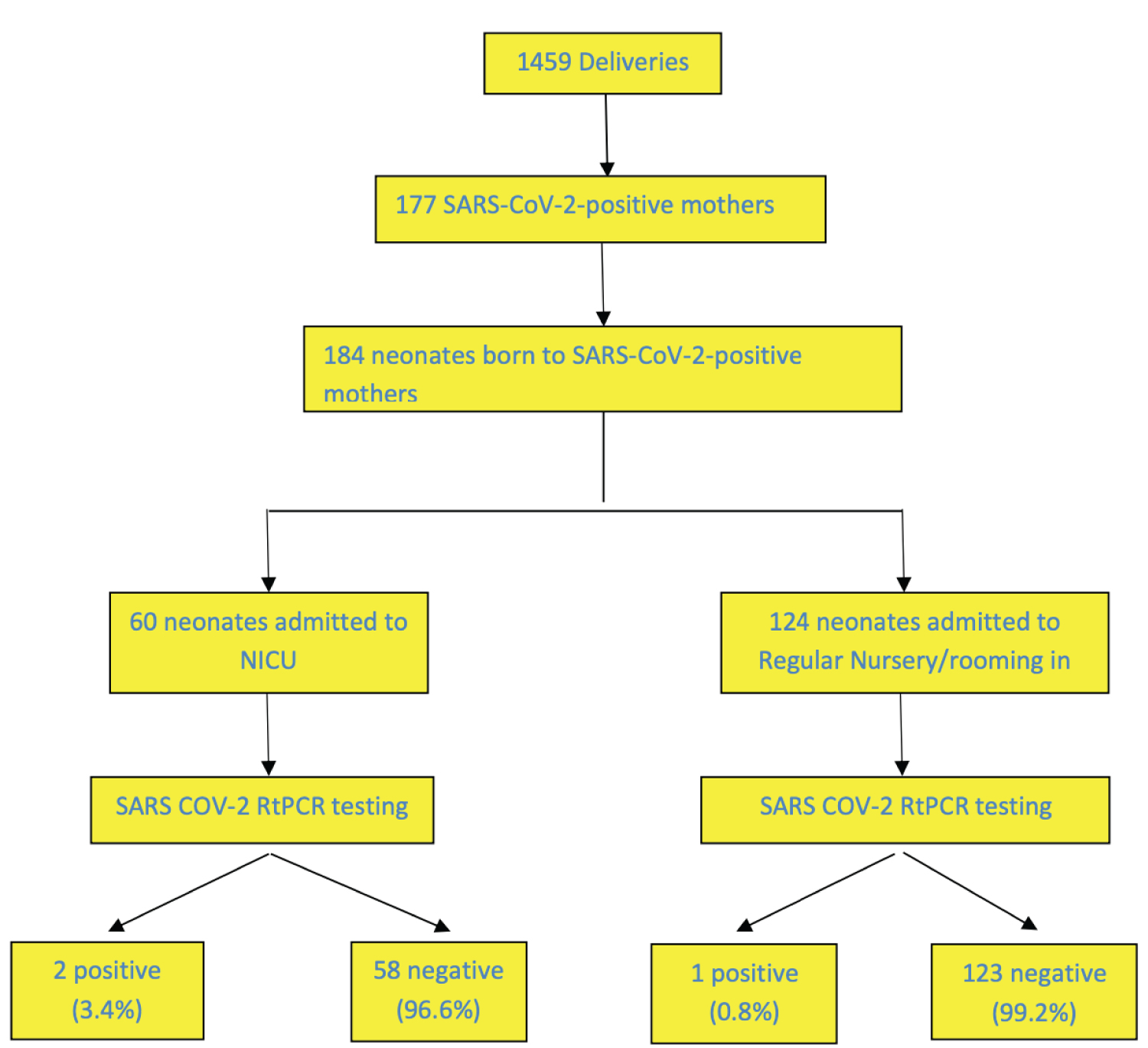 Figure 1: SARS COV-2 RtPCR exposure status in cohort of deliveries (March 15 to August 31, 2020).
View Figure 1
Figure 1: SARS COV-2 RtPCR exposure status in cohort of deliveries (March 15 to August 31, 2020).
View Figure 1
Table 1: Selected demographic and clinical characteristics of exposed neonates. View Table 1
One hundred and twenty-four neonates born to mothers with COVID were admitted to regular nursery and allowed to room in with their mothers. Of these, on neonate (0.8%) born to an asymptomatic mother, tested positive for SARS-COV-2, the infant was discharged with mother and did well.
There were more Hispanic mothers with maternal COVID but the significance of this is unclear as it also closely reflects our service area population. Fourteen (23%) of the exposed neonates were twin gestation. Table 2 shows selected gestational age and birth weight data for the twin cohort. All twins born to mothers with COVID were born preterm with 13 of 14 (93%) with low birth weight.
Table 2: Selected data for twins exposed to SARS-COV-2. View Table 2
There was a high rate of Caesarian section among the exposed groups; 32 (53%) of neonates were born via C/S. Both neonates with COVID were born by C/S.
Maternal COVID was more likely in women on public insurance. There was one maternal death in the cohort.
Exposure was associated with preterm birth (55%) and low birth weight (40%). There were 2 SARS-COV-2 infected neonates including 1 exposed to HIV/SARS-COV-2 co-infection. Eight (14%) mothers had fevers. The two neonates with COVID-19 were born to symptomatic mothers with fever and cough; one mother had febrile illness with cough and signs of lower respiratory tract disease. Table 3 shows clinical characteristics of neonates born to mothers with COVID-19 admitted to NICU.
Table 3: Clinical characteristics of neonates born to mothers with COVID-19 admitted to NICU N = 60 neonates born to 53 mothers. View Table 3
Exposed neonates also had other related complications due to prematurity like respiratory syndrome, transient tachypnea of the newborn. Neonates with COVID as well as 17% of exposed neonates needed phototherapy for hyperbilirubinemia (Table 3). Antibiotic use for presumed sepsis was also high among the cohort: 35 out of 58 (60%) neonates received a course of IV antibiotics.
There were total of 4 term neonates who developed fever (temp range = 38.2 °C to 38.8 °C) in the exposed group but tested negative for SARS-COV-2. Three (75%) of these 4 infants were born to mothers with fever. Two were born by emergency C/S for fetal distress and needed respiratory support (NCPAP) for =< 24 hours. The other two infants were born vaginally with no need for respiratory support. All infants were treated empirically for sepsis as per our NICU protocol and did well. 34 (59%) of exposed neonates needed positive pressure ventilation (mostly NCPAP use) and antibiotics respectively. Use of NCPAP was mostly related to prematurity.
Patient A was born at term to a mother with fever and cough. The infant was admitted to NICU for evaluation due to maternal fever. Summary characteristics are presented in Table 4. The infant remained stable in room air. The infant was treated for sepsis until blood cultures were negative. SARS-COV-2 rtPCR was positive at 32 hours of life, repeat was not done. COVID-19 specific treatment was not performed.
Table 4: Summary clinical characteristics of 2 neonates infected with SARS-COV-2. View Table 4
Patient B was born at 32 weeks to a HIV positive mother with maternal COVID who presented 3 days before delivery with febrile illness, cough, and shortness of breath, malaise and body aches. Her CXR showed nonspecific bilateral basal pneumonia. Infant's SARS-COV-2 was positive at 24 hours, 48 hours and 7 days of life. Infant remained stable in room air and was treated for hyperbilirubinemia (24 hours on phototherapy). Infant was not infected with HIV (RNA PCR testing was negative at > 1 and >= 4-months.
Both infants were discharged after completing sepsis protocol treatment in good and stable condition.
Our study shows consistency with other published studies in that a small proportion of SARS-COV-2 exposed neonates develop disease [4-7] and that disease is typically mild with good outcomes [8]. Our study highlights other secondary costs of neonatal exposure to maternal COVID including preterm births, [9] neonatal fever, and higher risk for infants born to mothers on public insurance.
Our study showed a high proportion of preterm births to the maternal COVID cohort. Prematurity on its own is associated with short and long-term complications. Synergistic effect of COVID-19 intrauterine exposure for infant health and development is an emerging field; since maternal COVID is a relatively new and evolving disease, it would take several years to grasp the full effect on exposed. For example, epidemiologic studies have shown a link between prenatal infection and enhanced expression of cytokines which acts as "neurodevelopmental disease primer" that may increase expression of a range of neurological disorders [10-12] later in life. Translation of these findings is an emerging field that will benefit from critical research and insight.
Our findings on increased risks of SARS-COV-2 exposure in newborns for those on public as compared to private insurance has implications on health policy and spending. Low socioeconomic status is associated with high COVID disease burden and low vaccination rate, creating a double-whammy effect and opportunities for tailored public health programs [13]. Strategic prevention efforts uniquely designed to engage this group should be key priority. Additionally, the reduced health care expenditure during COVID-19 has contributed to excess earnings for insurers and these earnings represent an opportunity to effectively tackle the pandemic by redirecting spending on tailored preventive programs for low-income pregnant women [14]. These services may include action to address disparities during pregnancy, effective primary and secondary preventive strategies that include additional support systems and follow up for preterm SARS-COV-2 exposures.
Our study has some limitations. Due to retrospective nature of the study, we may not have captured some other significant effects of SARS-COV-2 exposure. In addition, SARS-COV-2 delivery testing status may have limited our ability to capture other interesting but impactful findings for earlier exposure. The maternal death in the cohort reminds us that COVID-19 during pregnancy is not a benign occurrence and highlights the high health and human cost of maternal COVID.
Finally, pregnant women should be considered high risk with tailored policies and public health strategies focusing on prevention of disease, transmission and management. We recommend that preventive education and targeted prophylaxis during pregnancy should become routine and that pregnant women should be prioritized for COVID-vaccination strategies. Women on public insurance may require targeted outreach efforts to promote equitable uptake of preventive of COVID-19 vaccine.
The IRB at the St Joseph's Health approved the study and waived the need for individual consent.
Not applicable.
The authors have no financial relationships relevant to this article to disclose.
The authors have no conflicts of interest relevant to this article to disclose.
There was no funding source for this study.
Data used for analysis is included in publication.
All authors are responsible for reported findings and all authors have participated in the concept and design, drafting and revising of the manuscript, and have approved the manuscript as submitted.