Background: The coronavirus disease 2019 (COVID-19) is a multi-system infection which predominantly affects the respiratory system. Subcutaneous emphysema with or without pneumomediastinum and pneumothorax been recently reported as an unusual complication in cases of severe COVID-19 pneumonia.
Case presentation: We report three cases of COVID-19 pneumonia complicated by subcutaneous emphysema with all cases showed resolution of emphysema with chest tube followed by tracheostomy.
Conclusion: Due to growing number of cases that developed coronavirus infection associated with subcutaneous emphysema, this approach can be considered in treating such condition. However, the timing and efficacy of tracheostomy in COVID-19 patient with subcutaneous emphysema still remain elusive and more studies are needed to confirm the role of tracheostomy in managing subcutaneous emphysema.
Coronavirus, Covid-19, Subcutaneous emphysema, Tracheostomy
COVID-19 caused by infection with severe acute respiratory syndrome coronavirus-2 (SARS- CoV-2), was identified in late 2019 with first case reported in the Chinese province of Wuhan. It has rapidly spread around the world and has become a pandemic [1]. It is a multi-system infection which predominantly affects the respiratory system facilitated by Angiotensin-converting enzyme 2 (ACE2) receptor [1].
Significant research efforts are taking place around the world for a better understanding of the transmission dynamics, spectrum of clinical disease, complications, possible treatment options and prevention measures. There are numerous cases of subcutaneous emphysema reported in Covid 19 patients. However, there are hardly any data or research in the current literature to study in depth the relationship between SARS-CoV-2 infection and subcutaneous emphysema and its management.
Herein, we describe three cases of SARS-CoV-2 pneumonia who were admitted to the intensive care unit and developed spontaneous subcutaneous emphysema with and without concomitant pneumothorax, which resolved completely after tracheostomy.
A 58-year-old, male, a non-smoker with no co-morbid presented to emergency department (ED) with fever associated with shortness of breath and productive cough for 1 week. The diagnosis of COVID-19 was confirmed by reverse transcription polymerase chain reaction (RT-PCR). He was admitted to the intensive care unit and intubated in view of respiratory distress. Chest x-ray following intubation revealed moderate subcutaneous emphysema but no pneumothorax (Figure 1). The subcutaneous emphysema was initially managed conservatively. However, despite the support measures, his subsequent chest x-ray 4 days later demonstrated extensive pneumothorax. Chest tube was inserted, only slight improvement of subcutaneous emphysema observed clinically. Tracheostomy was performed one day after chest tube insertion for anticipating prolonged ventilation. Complete resolution of subcutaneous emphysema seen one day after tracheostomy was performed and subsequently the chest drain was removed.
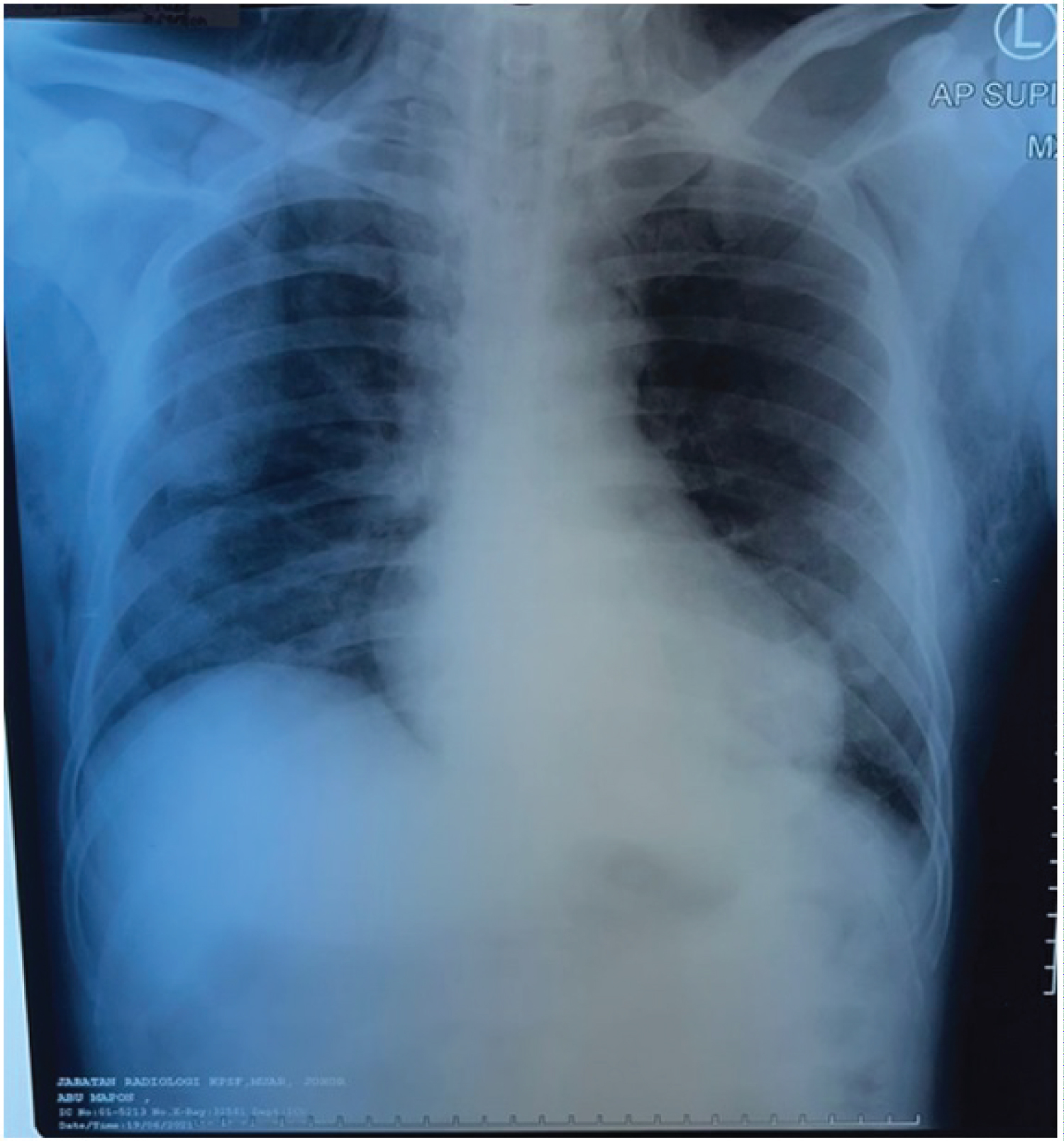 Figure 1: Chest x-ray showing perihilar opacities and left lower lobe opacity with subcutaneous emphysema.
View Figure 1
Figure 1: Chest x-ray showing perihilar opacities and left lower lobe opacity with subcutaneous emphysema.
View Figure 1
A 62-year-old female with a past medical history of diabetes mellitus and hypertension presented to ED with lethargy and fever for 5 days. The initial chest x-ray revealed perihilar opacification. The diagnosis of COVID-19 was confirmed by RT-PCR. She developed dyspnoea one day later and was subsequently admitted to the ICU for management acute respiratory distress syndrome (ARDS) and COVID-19. The patient was intubated shortly thereafter due to increasing oxygen requirement. Few days later, chest x-ray showed minimal pneumothorax with subcutaneous emphysema (Figure 2), and were managed conservatively. Tracheostomy was done 3 days later and subcutaneous emphysema rapidly resolved after the surgery.
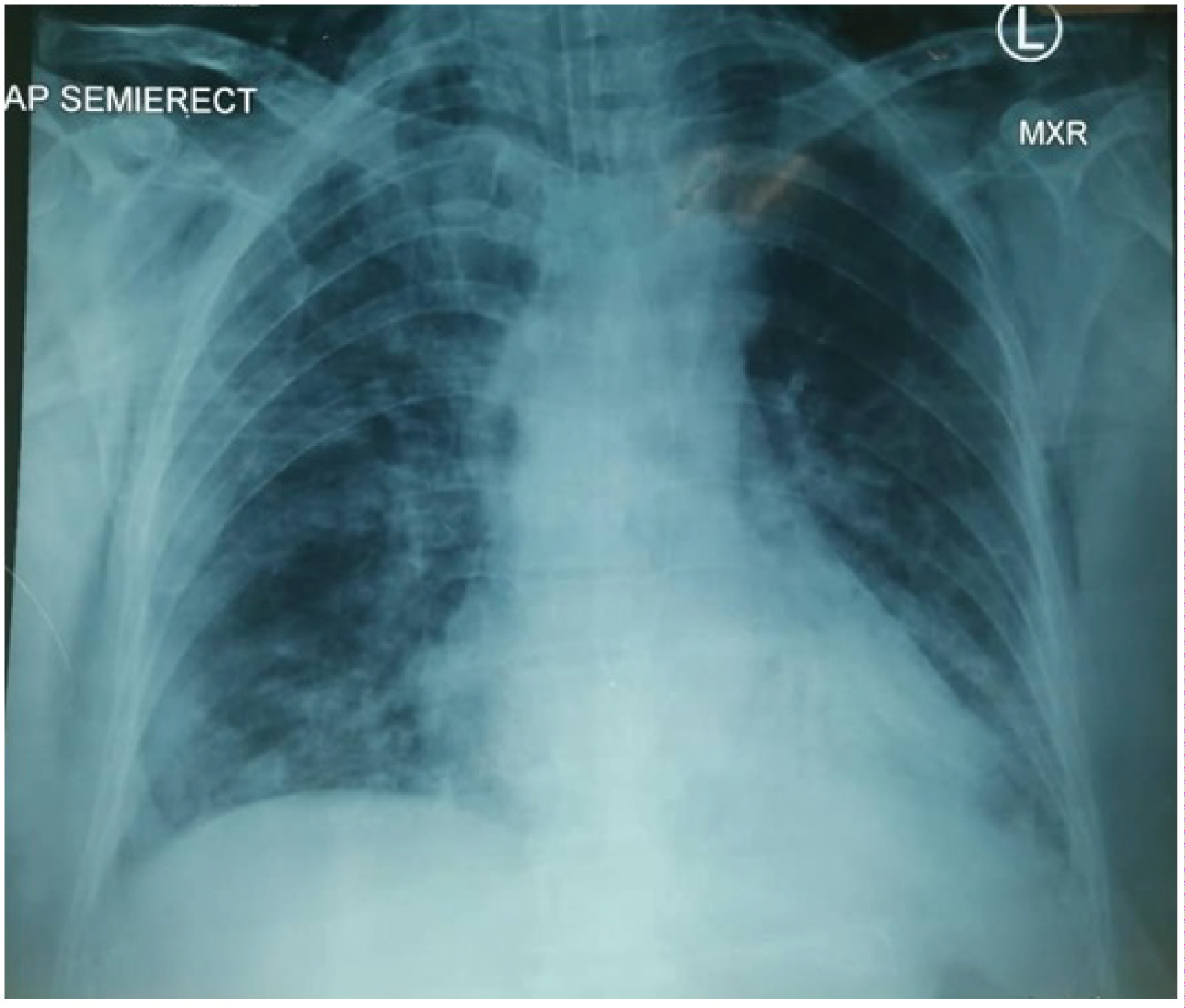 Figure 2: Chest x-ray showing lung parenchymal opacities over bilateral middle and lower lobes with minimal pneumothorax and subcutaneous emphysema.
View Figure 2
Figure 2: Chest x-ray showing lung parenchymal opacities over bilateral middle and lower lobes with minimal pneumothorax and subcutaneous emphysema.
View Figure 2
A 56-years-old male with background of diabetes mellitus, hypertension, and history of cerebrovascular accident presented with sudden onset of shortness of breath. He had fever and cough 3 days prior. He was admitted tohospital with suspicion of COVID-19. Supplementary oxygen was given via venturi mask. He progressed to severe dyspnoeaa day later and subsequently was transferred to the ICU. A SARS-CoV-2 test was positive. He developed subcutaneous emphysema 4 days later (Figure 3) and a chest tube was inserted. Tracheostomy with indication of prolonged ventilation was done on day 11 of intubation. On post op day 2, subcutaneous emphysema was completely resolved and chest tube was then removed.
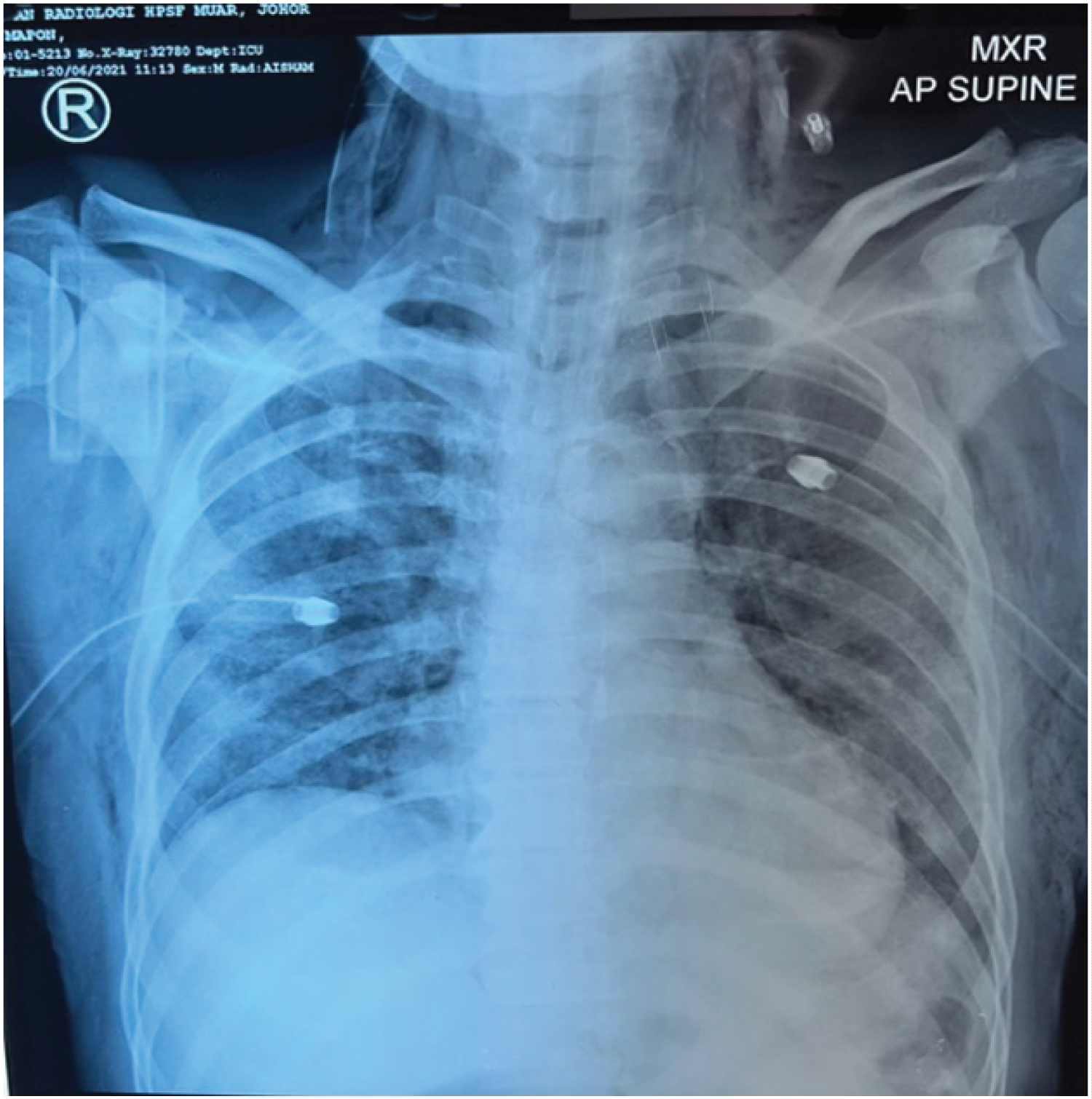 Figure 3: Chest x-ray of post chest tube insertion in Covid-19 pneumonia showing bilateral ground glass appearance with subcutaneous emphysema up to neck.
View Figure 3
Figure 3: Chest x-ray of post chest tube insertion in Covid-19 pneumonia showing bilateral ground glass appearance with subcutaneous emphysema up to neck.
View Figure 3
Subcutaneous emphysema describes the presence of gas in tissues beneath the skin. Possible causes of subcutaneous emphysema include blunt or penetrating trauma to the respiratory and gastrointestinal tract, infection, pneumothorax, barotrauma, malignancy, and even spontaneous [2]. It usually occurs in the soft tissues of the neck or chest wall but can also occur in the other parts of the body [3].
There is limited article about classification and management of subcutaneous emphysema especially subcutaneous emphysema that complicate COVID-19 infection. But there are large number of case reports and case series of subcutaneous emphysema related to COVID-19 in the literature with different causes and management. Our case illustrates subcutaneous emphysema that are managed with tracheostomy with and without chest tube prior to it. All of these patients showed rapid resolution following tracheostomy.
The exact pathogenesis of subcutaneous emphysema in COVID-19 still remains unclear. Nowadays, the occurrence of barotrauma such as pneumothorax, pneumomediastinum and subcutaneous emphysema had been rarely seen in ICU patient with acute respiratory distress syndrome due to the use of protective ventilation. However, during this COVID-19 pandemic there is noticeable increase of patient with pneumothorax, pneumomediastinum and subcutaneous emphysema despite the use of the similar unchanged protective mechanical ventilation approach. Lemmers, et al. reported pneumomediastinum/ subcutaneous emphysema occurred in 23 out of 169 (13.6%) patients with acute respiratory syndrome and COVID-19 (CoV-ARDS) and in three out of 163 (1.9%) patients with no CoV-ARDS (p < 0.001). This shows that CoV-ARDS patients had a high incidence of developing pneumomediastinum/subcutaneous emphysema despite theuse of low tidal volume and low airway pressure. It has been postulated that an increased lung frailty in CoV-ARDS could explain this finding more than barotrauma [4].
Most subcutaneous emphysema is self-limiting and resolves spontaneously without intervention. However, massive or extensive subcutaneous emphysema that extending beyond the trunk into the neck and head should be managed to prevent the complications such as tension phenomenon leading to dysphagia, dysphonia, palpebral closure, compartment syndrome, and intracranial hypertension [5]. It can also be complicated by restriction of full lung expansion and can lead to high airway pressure causing airway compromise, ventilator failure, severe respiratory acidosis, ventilator failure and pacemaker malfunction [2,6].
Aghajanzadeh M, et al. had come out with classification of severity of subcutaneous emphysema based on anatomical extension into five grades including the 1) Base of the neck, 2) All of the neck area, 3) Subpectoralis major area, 4) Chest wall and all of the neck area, and 5) Chest wall, neck, orbit, scalp, abdominal wall, upper limbs, and scrotum [2]. In general, there is no guidelines on the management of subcutaneous emphysema exist. There are a variety of case-based recommendations in the literature, but no controlled trial has been conducted to date [5]. Various approaches used to manage subcutaneous emphysema include subcutaneous incisions, needles, drains and cervical mediastinotomy [2] and the superiority of each technique is debatable.
Yeoh, Christopher SN, et al. [7] reported a case of a gentleman who developed massive subcutaneous emphysema post laparoscopic abdominal surgery and an exploratory laparotomy which was successfully managed with a surgical tracheostomy. The patient showed significant resolution of the subcutaneous emphysema on the second postoperative day. Surgical tracheostomyaids to promote the resolution of the massive subcutaneous emphysema as performing a wide incision along with loose closure of the tracheostomy wound assists the dissipation of air from the fascial planes and deep neck spaces.A tracheostomy also helps to reduce the airway pressure within the trachea.
The high incidence of subcutaneous emphysema related to COVID-19 deserves a careful assessment. The timing and efficacy of tracheostomy in COVID-19 patient with subcutaneous emphysema still remain elusive and more studies are needed to confirm the role of tracheostomy in managing subcutaneous emphysema.
Not applicable.
Appropriate verbal informed consent was obtained for publication of this case report and accompanying images.
All data underlying the results are available as part of the article and no additional source data are required.
No conflict of interest declared.
We declare that this study has received no financial support.
Dayang Anis Asyikin: Writing original draft; Athira Farasyafiqa: Data collection and case interpretation; Siti Halimahtun Sahab: Literature search and case illustration; Noorizan Yahya and Mohamad Khir Abdullah: Review and editing manuscript.
We thank the patients for allowing us to share their details. The completion of this manuscript could not have been possible without the participation and assistance of so many people whose names may not all be enumerate.