We report two cases of a usual saccular cerebral aneurysm with an iatrogenic lacerated aneurysmal neck during surgical clipping. In both cases, the aneurysmal neck was lacerated iatrogenically, and the aneurysm was clipped safely after suturing the lacerated portion. In treatment of a lacerated aneurysmal neck during surgical clipping of usual saccular cerebral aneurysms, the aneurysm may be considered to be clipped after suturing the lacerated portion. However, trapping and/or bypass surgery become necessary, depending on the characteristics of the aneurysm or the degree of neck laceration. Though surgical clipping of usual saccular cerebral aneurysms is known to be an established treatment method, various treatments should be prepared for unexpected situations to avoid catastrophic cerebral ischemia.
Cerebral aneurysm, Surgical clipping, Aneurysmal neck, Laceration
Most usual saccular cerebral aneurysms can be cured with surgical clipping or coil embolization [1-4]. Surgical clipping of usual saccular cerebral aneurysms is an established treatment method with a long history, and intraoperative aneurysmal neck laceration is a well-known complication [5-10].
In this article, we report two cases of a usual saccular cerebral aneurysm with an iatrogenic lacerated aneurysmal neck during surgical clipping and discuss appropriate treatment for this medical emergency.
A 72-year-old woman with hypertension was admitted to our hospital for consciousness disturbance following a sudden severe headache and vomiting. On admission, the Glasgow Coma Scale (GCS) was 13, and no apparent hemiparesis was observed. Brain computed tomography (CT) showed diffuse subarachnoid hemorrhage (SAH), mainly in the interhemispheric cisterns with mild ventricular dilatation (Figure 1A). Three-dimensional computed tomography angiography (3DCTA) revealed a saccular aneurysm on the distal portion of the left anterior cerebral artery (Figure 1B). The diagnosis was of SAH due to a ruptured cerebral aneurysm (Hunt and Kosnik grade (H-K) Ⅲ). Surgical clipping via the anterior interhemispheric approach was performed on Day 0. The aneurysmal neck was lacerated iatrogenically during detachment of the aneurysm (Figure 1D). Under 30 minutes of blood flow blocking, the lacerated portion was sutured with four stitches of 10-0 nylon threads (Figure 1E) and the aneurysm was clipped completely with one titanium clip (Figure 1F). The postoperative course was uneventful, and postoperative 3DCTA showed complete clipping of the aneurysm (Figure 1C). The patient was discharged without any neurological deficit on Day 30, and she currently lives normally (modified Rankin Scale (mRS) 0). The aneurysm had no relapse for 8 years.
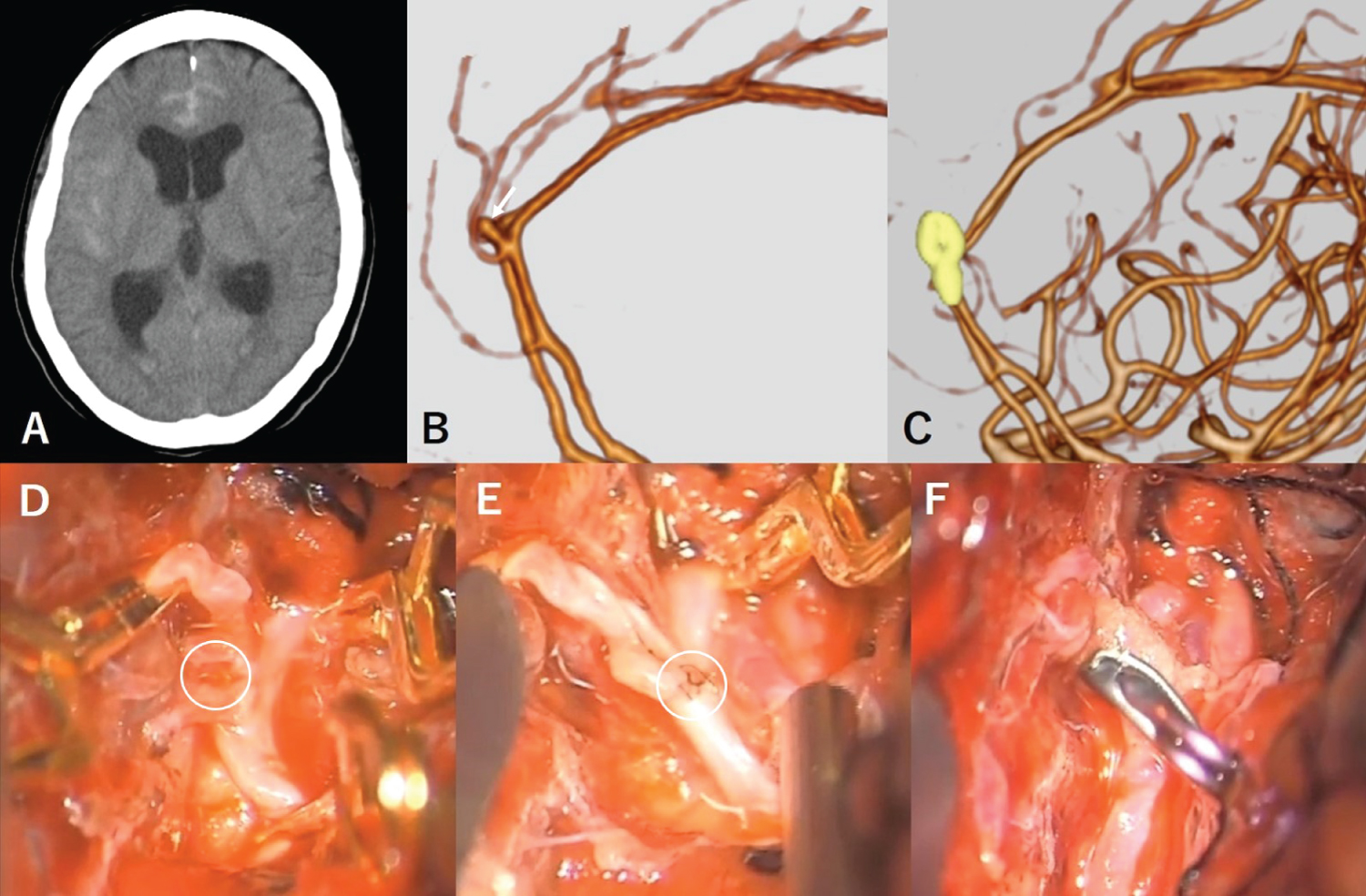 Figure 1: Brain computed tomography (A) showing diffuse subarachnoid hemorrhage mainly in the interhemispheric cisterns with mild ventricular dilatation. Three-dimensional computed tomography angiography (3DCTA) (B) revealing a saccular aneurysm on the distal portion of the left anterior cerebral artery (white arrow). Postoperative 3DCTA (C) shows complete clipping of the aneurysm. Intraoperative photographs showing a lacerated aneurysmal neck portion (white circle) (D), a sutured lacerated neck portion (white circle) (E), and complete clipping (F).
View Figure 1
Figure 1: Brain computed tomography (A) showing diffuse subarachnoid hemorrhage mainly in the interhemispheric cisterns with mild ventricular dilatation. Three-dimensional computed tomography angiography (3DCTA) (B) revealing a saccular aneurysm on the distal portion of the left anterior cerebral artery (white arrow). Postoperative 3DCTA (C) shows complete clipping of the aneurysm. Intraoperative photographs showing a lacerated aneurysmal neck portion (white circle) (D), a sutured lacerated neck portion (white circle) (E), and complete clipping (F).
View Figure 1
A 62-year-old man with hypertension was admitted to our hospital for a restless confusion following sudden severe headache and vomiting. On admission, the GCS was 12, and no apparent hemiparesis was observed. Brain CT showed diffuse SAH, mainly in the basal and interhemispheric cisterns with mild ventricular dilatation (Figure 2A). Cerebral angiography revealed a saccular aneurysm on the anterior communicating artery (Figure 2B). The diagnosis was of SAH due to a ruptured cerebral aneurysm (H-K Ⅳ). Coil embolization was tried, but it was discontinued because of catheter access difficulty on Day 0. Surgical clipping via the anterior and basal interhemispheric approach was performed on Day 1. The aneurysmal neck was lacerated iatrogenically during exploration of the residual neck after tentative clipping (Figure 2D). Under 28 minutes of blood flow blocking, the lacerated portion was sutured with two stitches of 10-0 nylon threads (Figure 2E) and the aneurysm was clipped incompletely with a residual part including the sutured lacerated portion to preserve a hypothalamic artery (Figure 2F). Intraoperative indocyanine green video angiography described the hypothalamic artery, while the residual part was not described (Figure 2G). Postoperative magnetic resonance imaging showed right Heubner artery territory ischemia, and the patient had moderate left hemiparesis. However, hemiparesis resolved completely following rehabilitation. Postoperative cerebral angiography showed no apparent residual neck portion of the aneurysm (Figure 2C). The patient was discharged with moderate cognitive dysfunction on Day 60 after ventriculoperitoneal shunt surgery for chronic hydrocephalus, and he currently lives normally with light assistance (mRS 3). The aneurysm had no relapse for 3 years.
 Figure 2: Brain computed tomography (A) shows diffuse subarachnoid hemorrhage mainly in the basal and interhemispheric cisterns with mild ventricular dilatation. Three-dimensional digital subtraction angiography (3DDSA) of the right internal carotid artery (R.ICA) (B) reveals a saccular aneurysm on the anterior communicating artery (white arrow). Postoperative 3DDSA of R.ICA (C) shows no apparent residual neck portion of the aneurysm. Intraoperative photographs show a lacerated aneurysmal neck portion (white circle) D), a sutured lacerated neck portion (white circle) (E), and incomplete clipping with a residual part including the sutured lacerated neck portion (white circle) (F). Intraoperative indocyanine green video angiography (G) describes a hypothalamic artery (white arrow), while the residual part of the aneurysm is not described.
View Figure 2
Figure 2: Brain computed tomography (A) shows diffuse subarachnoid hemorrhage mainly in the basal and interhemispheric cisterns with mild ventricular dilatation. Three-dimensional digital subtraction angiography (3DDSA) of the right internal carotid artery (R.ICA) (B) reveals a saccular aneurysm on the anterior communicating artery (white arrow). Postoperative 3DDSA of R.ICA (C) shows no apparent residual neck portion of the aneurysm. Intraoperative photographs show a lacerated aneurysmal neck portion (white circle) D), a sutured lacerated neck portion (white circle) (E), and incomplete clipping with a residual part including the sutured lacerated neck portion (white circle) (F). Intraoperative indocyanine green video angiography (G) describes a hypothalamic artery (white arrow), while the residual part of the aneurysm is not described.
View Figure 2
Various complications occur in surgical clipping of usual saccular cerebral aneurysms, including bleeding from the aneurysm [5-10]. An aneurysm can be clipped usually when bleeding is controlled from the aneurysmal body. However, treatment of an aneurysm is very difficult when there is bleeding from the lacerated aneurysmal neck. A few reports have been published on how to treat the aneurysm in such medical emergency [6-8,10]. Barrow and Spetzler reported cotton-clipping technique to repair intraoperative aneurysmal neck tear [6]. Their technique may be useful, but we doubt whether the technique can prevent rebleeding or occurrence of a pseudo-aneurysm in such all cases. In case 1, the lacerated neck portion was too large to perform the cotton-clipping technique. In case 2, the cotton-clipping technique must have caused a hypothalamic artery territory ischemia. On the other hand, Saito, et al. recommended that the aneurysm with a lacerated aneurysmal neck should be clipped after suturing the lacerated portion under blood flow blocking [10]. They emphasized that the lacerated aneurysmal neck portion should be sutured with thicker pieces than usual in a right angle direction to the presumed clip blade to avoid enlargement of the lacerated neck portion. We believe that the aneurysm may be considered to be clipped after suturing the lacerated portion when there is bleeding the lacerated aneurysmal neck. However, trapping and/or bypass surgery become necessary depending on the characteristics of the aneurysm or the degree of neck laceration [7,8]. Fukuda, et al. reported two cases of a ruptured anterior communicating artery aneurysm with a lacerated aneurysmal neck during surgical clipping [7]. In both cases, trapping could not be avoided because the lacerated neck portion was too fragile to suture, and one case required an A3-A3 bypass for blood flow preservation. Jung, et al. reported a case of an unruptured middle cerebral artery aneurysm with a lacerated aneurysmal neck during surgical clipping [8]. In their case, middle cerebral artery-superficial temporal artery interposition graft-middle cerebral artery anastomosis was performed because stenosis due to the sutured lacerated neck portion caused blood flow disorder.
We report two cases of a usual saccular cerebral aneurysm with a lacerated aneurysmal neck during surgical clipping. In both cases, the aneurysmal neck was lacerated iatrogenically, and the aneurysm was clipped safely after suturing the lacerated portion. The aneurysm with a lacerated aneurysmal neck may be considered to be clipped after suturing the lacerated portion under blood flow blocking, and the lacerated aneurysmal neck portion should be sutured with thicker pieces than usual in a right angle direction to the presumed clip blade to avoid enlargement of the lacerated neck portion. However, trapping and/or bypass surgery become necessary depending on the characteristics of the aneurysm or the degree of neck laceration. Though surgical clipping of the usual saccular cerebral aneurysms is known to be an established treatment method, various treatments should be prepared for unexpected situations to avoid catastrophic cerebral ischemia.
None.
These authors contributed equally to this work.