Obstructed Hemivagina with Ipsilateral Renal Anomaly (OHVIRA) is a rare Mullerian anomaly of the female reproductive tract. This case presents a 12-year-old postmenarchal female who presented to the emergency department with abdominal pain for five days. On transvaginal ultrasound and pelvic computed tomography, she was found to have hematometrocolpos, uterine didelphys, complete right renal agenesis, and a right adnexal mass on imaging. Subsequent pelvic MRI confirmed the diagnosis of obstructed hemivagina and uterine didelphys, consistent with OHVIRA syndrome. Patient underwent a diagnostic vaginoscopy/hysteroscopy and vaginal septum resection using a LigaSure. This was followed by a diagnostic laparoscopy, and a left salpingo-oophorectomy was next performed for coinciding ovarian torsion. The patient was healing well without complaints by post-op day 12 and again during a phone call five months later. This case presents laparoscopic LigaSure as an option for gynecologists to manage and treat OHVIRA syndrome.
OHVIRA: Obstructed Hemivagina with Ipsilateral Renal Anomaly; IP Ligament: Infundibulopelvic Ligament; GIA Surgical Stapler: Gastrointestinal Anastomosis Surgical Stapler
Mullerian duct anomalies occur in approximately 5.5% of uterus-possessing people in the general population, with Obstructed Hemivagina with Ipsilateral Renal Anomaly (OHVIRA) syndrome accounting for 0.16-10% of these anomalies [1,2]. OHVIRA syndrome, also known as Herlyn-Werner-Wunderlich syndrome, is a rare Mullerian anomaly of the female reproductive tract first described in 1922 [3,4]. It has since been reported in literature mostly as case reports and retrospective case series, and no consistent management approach has been described [3,5,6]. It classically presents as uterine didelphys with concurrent unilateral vaginal obstruction and ipsilateral renal agenesis [6]. Definitive surgical management is necessary to relieve symptoms of dysmenorrhea and pelvic pain from resulting hematocolpos and/or hematometra, as well as to prevent adverse fertility outcomes from possible hematosalpinx, endometriosis, pelvic infection, and pelvic adhesions [2-8]. Recent case reports mostly describe minimally invasive surgical approaches involving either single-stage or two-stage vaginoplasties, with subsequent laparoscopy mostly falling out of favor (unless indicated for other reasons) [3-5]. Hematocolpos drainage and vaginal septum resection have been described using a variety of methods including sharp dissection followed by marsupialization of the septum edges, unipolar needle electrodes, spinal needle aspiration, Seldinger technique, aspiration via suprapubic catheter, hysteroscopic resectoscopes, surgical staplers, bipolar energy devices, and even hemihysterectomy with vaginectomy in rare cases of cervical atresia [1-5,7,8]. In this case, LigaSure was used in a single-stage procedure for vaginal septum resection in OHVIRA syndrome.
This case involves a 12-year-old postmenarchal, virginal female who presented to the emergency department with five days of abdominal pain as well as emesis that occured with initial symptom onset. She first presented to an outside emergency department, from which she was discharged home after an abdominal radiograph was reportedly negative. At her second hospital presentation, she had continued pain with nausea and normal bowel movements. The patient was also menstruating at this time. She reported menarche at age 10 with regular monthly menstrual cycles since that time, and she denied previous dysmenorrhea. According to her guardian, the patient had a known diagnosis of right renal agenesis, which was initially identified on fetal ultrasound in utero. All other medical, surgical, and social history was negative.
Labratory values were significant for a negavite urine pregnancy test, white blood cell count of 14.4 k/mm 3 , CRP elevated to 187.82 mg/L, and a non-elevated lactate. The patient was tachycardic on initial presentation, but vital signs were otherwise stable. On physical exam, the patient was noted to have right and left lower quadrant abdominal tenderness with guarding. There was no rebound tenderness, and abdominal exam was overall benign. Pelvic exam was deferred due to the patient’s age.
An ultrasound of the right lower quadrant was unremarkable and did not visualize the appendix. Pelvic Ultrasound was significant for a complex collection of fluid in the lower uterine segment measuring 9.7 × 5.8 × 6.7 cm. Additionally, a 7.3 × 2.9 × 6.9 cm complex cystic structure with multiple small septations was noted anterior to the uterus. These studies were followed by a CT Abdomen/Pelvis with IV contrast, which revealed a didelphys uterus with severe dilation of the cervix and vaginal canal with direct communication to the right uterine horn, a complex cystic and solid right adnexal mass with thick rim enhancement anterior to the uterus, mild left hydronephrosis, and congenital right renal agenesis. Finally, MR Pelvis with and without contrast was obtained for surgical planning. This confirmed uterine horn separation with duplication of the cervix and vagina-consistent with uterine didelphys-with severe dilation of the right cervix and vaginal canal suggestive of right hemivagina obstruction and resulting hematometrocolpos (Figure 1). Dilation of the cervix and vaginal canal measured 13.1 × 5.6 × 5.9 cm. The cystic structure was again noted in the right lower abdomen measuring 7.7 × 3.3 × 6.2 cm. It appeared to abut the left ovary, however the exact origin of the structure was unclear.
 Figure 1: MR pelvis demonstrating uterine didelphys with severe dilation of the right cervix due to right hemivaginal obstruction and resulting hematometrocolpos.
View Figure 1
Figure 1: MR pelvis demonstrating uterine didelphys with severe dilation of the right cervix due to right hemivaginal obstruction and resulting hematometrocolpos.
View Figure 1
The suspicion for appendicitis was low given the patient’s benign abdomen and largely unremarkable appendiceal findings on imaging. The combination of uterine didelphys and hematometrocolpos with confirmed congential renal agenesis was highly suspicious of OHVIRA syndrome. The differentials for the adnexal mass included ovarian torsion, hydrosalpinx/tubo-ovarian abscess (possible ascending infection secondary to hematometrocolpos), and malignancy.
The patient was admitted to pediatrics for pain control and consented for examination under anesthesia, hysteroscopic vaginoplasty, and diagnostic laparoscopy with likely robotic ovarian cystectomy. Procedure was performed under general endotracheal anesthesia. The patient was prepped and draped in the usual fashion and positioned in dorsal lithotomy position. Hematocolpos could be palpated along the right vaginal wall on initial bimanual exam. Diagnostic hysteroscopy of the presumed left uterine horn was performed with a 5 mm rigid hysteroscope. The left external cervical os (Figure 2) and the left uterine cavity appeared normal, and a single tubal ostium was visualized in the left superolateral aspect of the cavity. An incision was then made along the longitudinal vaginal septum using an electrosurgical pen, and the accumulated blood was evacuated. It was noted to be brown and thick in consistency. Breisky retractors were used to retract the vaginal side walls, and the septum was next excised along the anterior and posterior vaginal walls using a laparoscopic LigaSure. The septum was transected at the level of the cervix. After evacuation of the hematocolpos, a second cervical os could be seen on vaginoscopy (Figure 3). A diagnostic hysteroscopy of the right uterine horn was then performed: the right uterine cavity appeared normal with a single tubal ostium well-visualized at the right superolateral aspect of the cavity. Finally, cystoscopy and a rectal exam were performed, and no bladder or rectal injury could be appreciated.
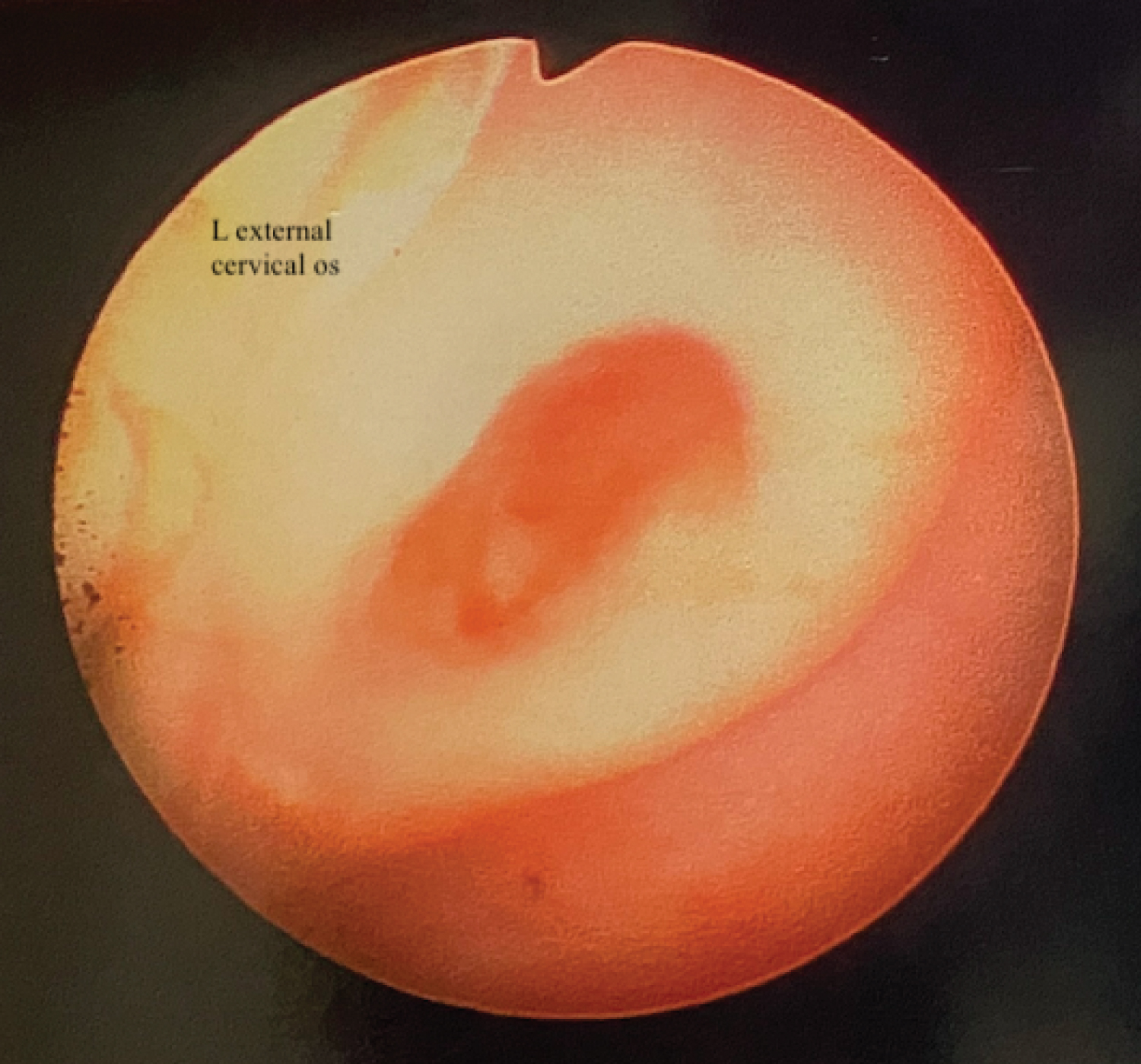 Figure 2: Vaginoscopic view of left external cervical os.
View Figure 2
Figure 2: Vaginoscopic view of left external cervical os.
View Figure 2
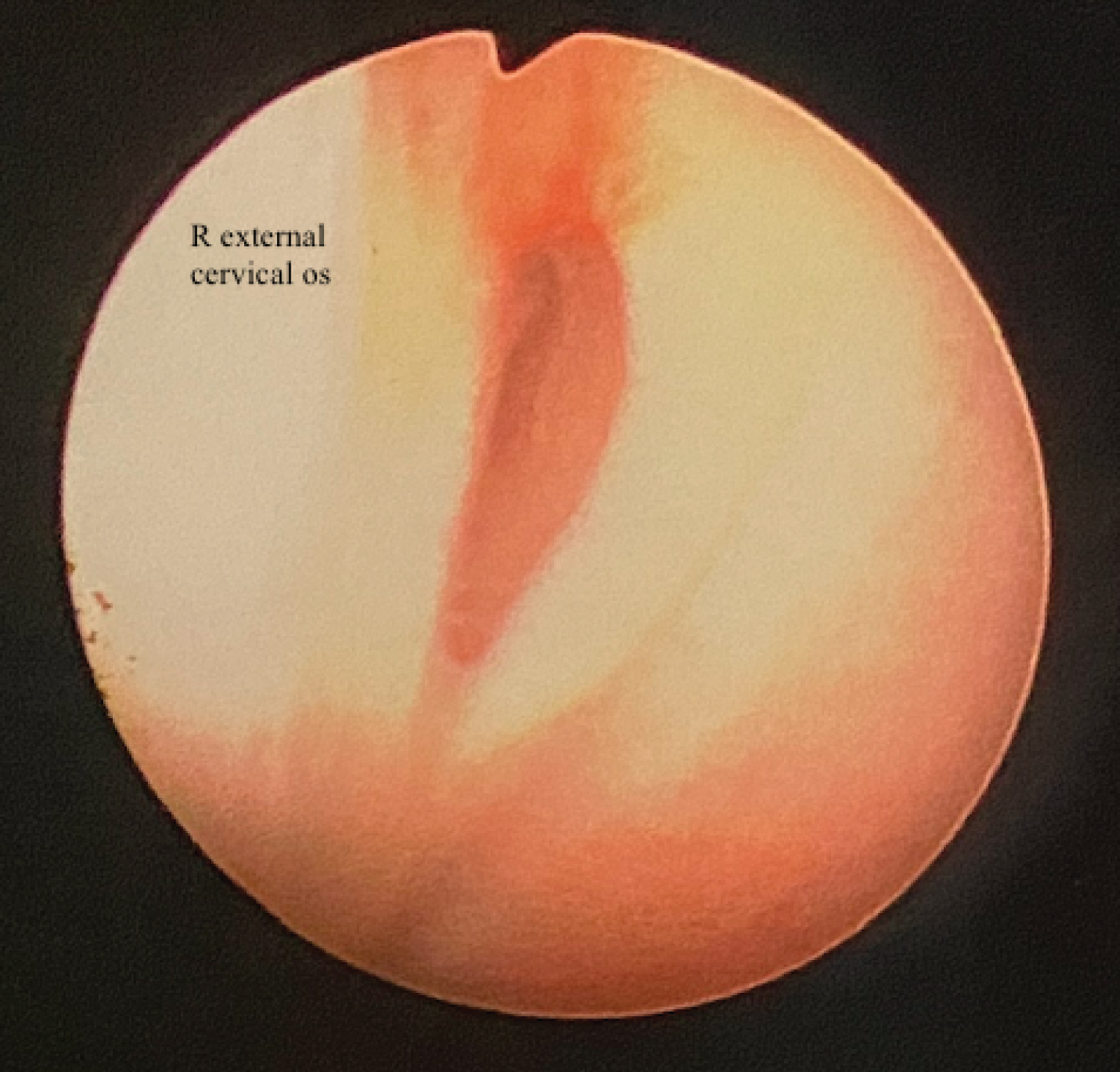 Figure 3: Vaginoscopic view of right external cervical os status-post vaginoplasty.
View Figure 3
Figure 3: Vaginoscopic view of right external cervical os status-post vaginoplasty.
View Figure 3
Attention was then turned to the abdomen. The abdomen was entered by Veress needle at Palmer’s point and subsequently insufflated to 20 mmHg using CO 2 . A 5 mm trocar was then inserted. Survey of the abdomen and pelvis confirmed two distinct uterine horns and a large, purple adnexal mass (Figure 4 and Figure 5). Aside from hemoperitoneum, there were no other significant abdominal or pelvic findings. Three 5 mm robotic ports were then inserted at Palmer’s point, superior to the umbilicus, and in the right upper abdominal quadrant, and the patient was positioned in 20 degrees of Trendelenburg. A 30-degree camera, robotic suction, fenestrated bipolar forceps, a robotic vessel sealer, and monopolar scissors were all used in this procedure. The right ovary and fallopian tube appeared normal. The left adnexa was found to be torsed multiple times at the level of the infundibulopelvic (IP) ligament. After detorsion, it remained enlarged and purple even after 15 minutes of attempted reperfusion. Left salpingo-oophorectomy was then performed as the ovary did not appear to be salvageable. After identifying the left ureter, the left IP ligament was coagulated and cut. The specimen was cut in half with cold scissors. The robot was undocked and the supraumbilical incision was extended to 12 mm. A balloon trocar was inserted through the extended port site, and the specimens were removed using Endo Catch bags. Hemoperitoneum was suctioned and the surgical sites were found to be hemostatic. After removal of the ports and desufflation of the abdomen, the 12 mm port site was closed at the fascial incision using a single 0-Vicryl suture and a fascial closure device. The abdominal skin incisions were closed using 4-0 Monocryl and subsequently covered in Dermabond. Marcaine was injected at the port sites for local anesthesia.
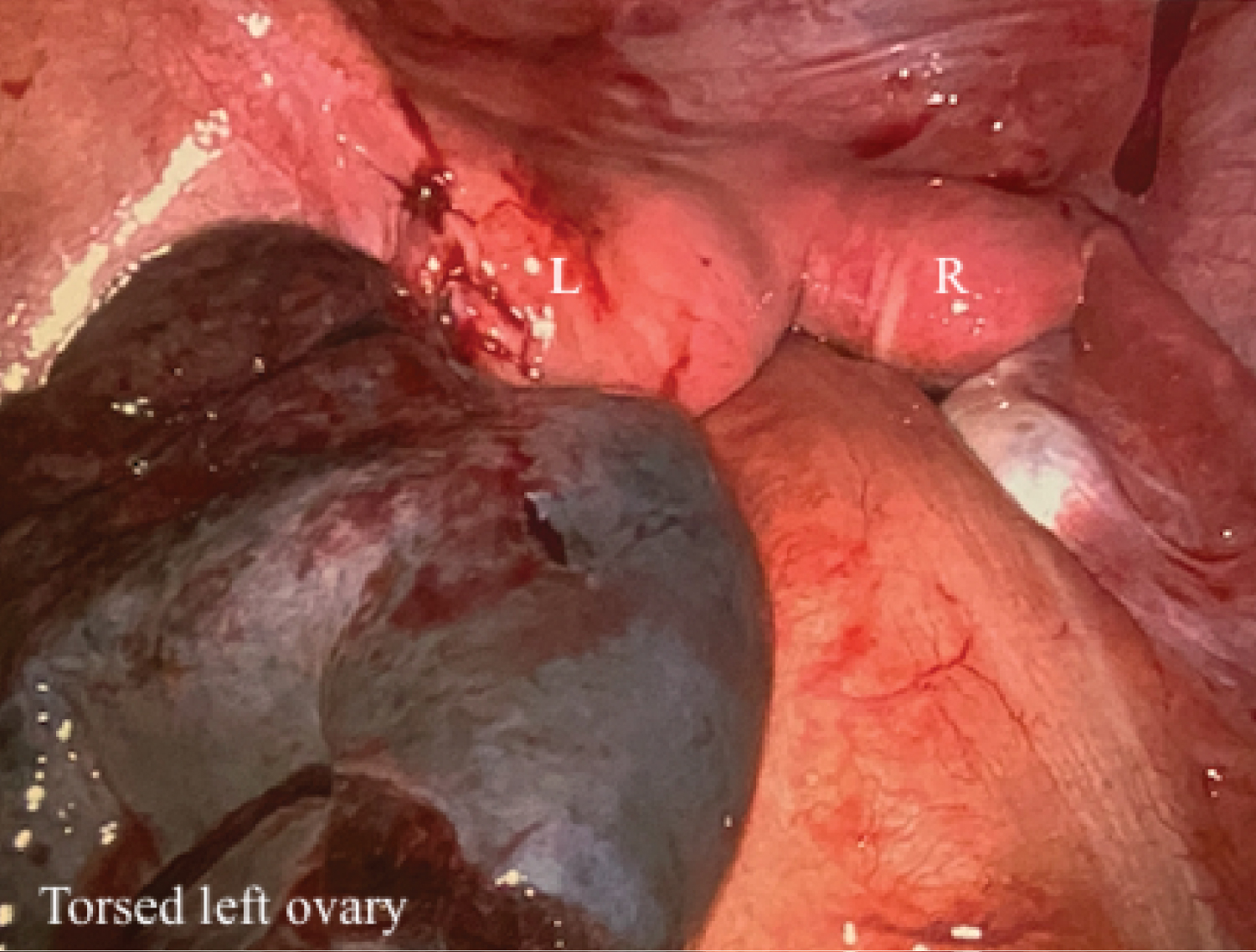 Figure 4: Laparoscopic view of uterine didelphys with left and right uterine horns; left ovarian torsion.
View Figure 4
Figure 4: Laparoscopic view of uterine didelphys with left and right uterine horns; left ovarian torsion.
View Figure 4
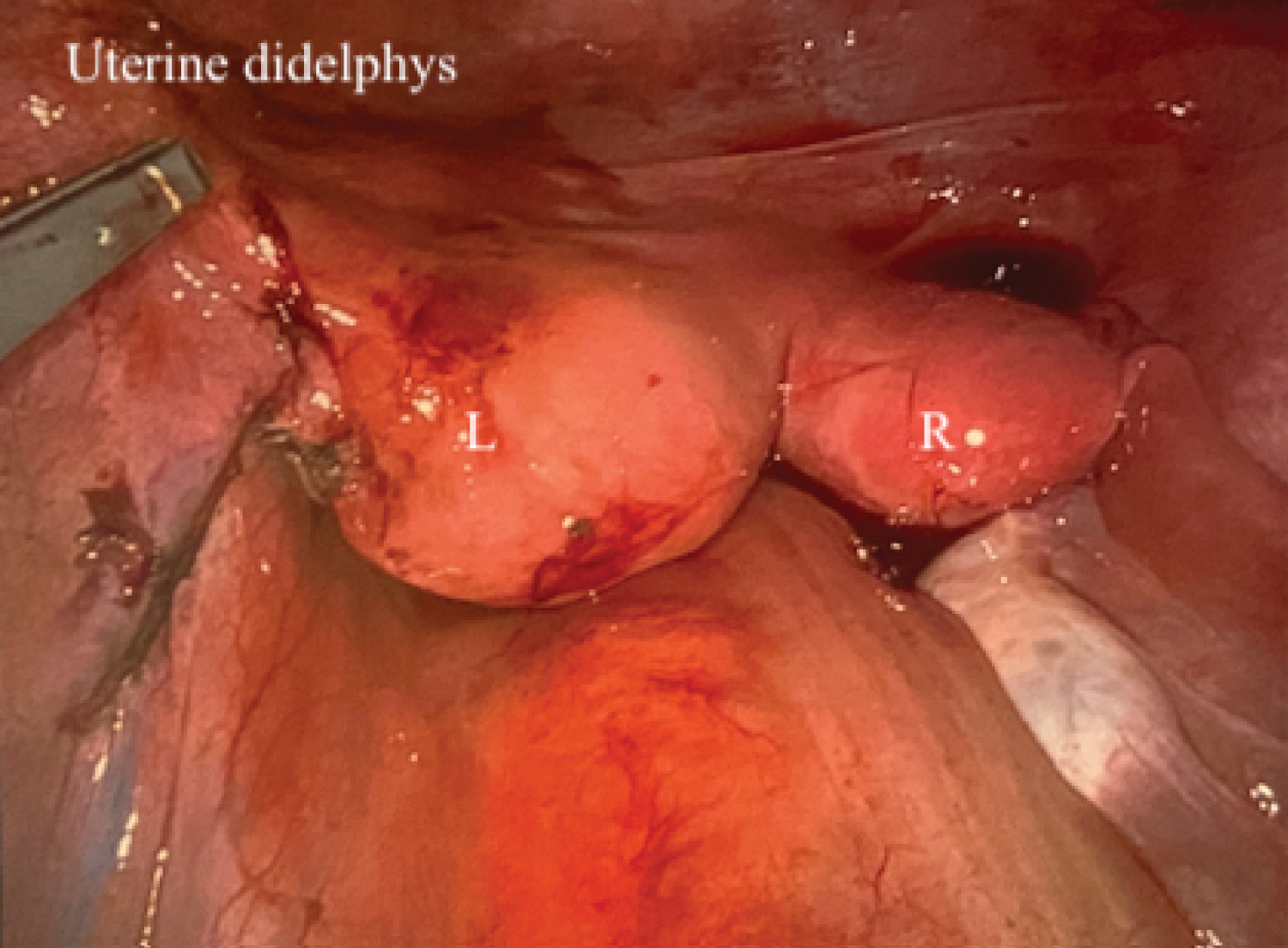 Figure 5: Laparoscopic view of didelphys uterus with left and right uterine horns.
View Figure 5
Figure 5: Laparoscopic view of didelphys uterus with left and right uterine horns.
View Figure 5
By post-operative day two, the patient met all post-operative milestones and was able to be discharged home. She had no complaints at her follow up appointment on post-operative day 12. She denied fevers, chills, nausea, emesis, abdominal pain, dysuria, urinary retention, constipation, or use of medications for pain control. She reported daily use of an abdominal binder for comfort, and the port sites were well-healed with Dermabond still in place. Pelvic exam was again deferred due to her age, but she denied pelvic pain. She had not yet had another menstrual cycle. Pathology results were reviewed with the patient: The vaginal septal tissue showed evidence of chronic inflammation without dysplasia or malignancy, and the necrotic ovarian tissue and fallopian tube were consistent with ovarian torsion. Oral contraceptive pills were offered to help regulate menstrual cycles and treat future dysmenorrhea, but the patient and her guardian declined. A phone call with the patient’s guardian five months later revealed that she continued to recover well and had no pelvic pain or gynecologic concerns at that time.
Mullerian, also called paramesonephric, ducts are responsible for the formation of the fallopian tubes, uterus, cervix, and upper two thirds of the vagina [2,3]. Anomalies arise from abnormal formation, fusion, or resorption of the these ducts during early embryogenesis (around week eight) [3,7]. The American Society of Reproductive Medicine classifies these defects based on uterine anatomy; uterine didelphys, a part of the classic presentation of OHVIRA syndrome, is a Class III fusion defect in which there are two non-communicating uterine cavities and two cervices [3,9,10]. This can occur as an isolated defect without concurrent vaginal septum or renal agenesis.
OHVIRA syndrome additionally involves defects of the Wolffian duct; ductal agenesis leading to unilateral renal agenesis is the most common of Wolffian defects in this syndrome [5]. The ipsilateral Mullerian duct then fails to fuse with the contralateral Mullerian duct, resulting in uterus didelphys; the ipsilateral Mullerian duct also becomes laterally displaced, which leads to an obstructed hemivagina [5]. OHVIRA syndrome can be further classified based on uterine and vaginal anatomy: Class 1 describes complete hemivaginal obstruction with (Class 1.2) or without (Class 1.1) cervical aplasia, and Class 2 describes this condition albeit with partial resorption of the septum, forming a fistula between the two vaginas (Class 2.1) or the two cervices (Class 2.2), allowing for drainage of menstrual blood [3,11].
Like the patient described in this case, most patients present after menarche with cyclic abdominal and/or pelvic pain, dysmenorrhea, and a pelvic mass and/or vaginal bulge [4-8]. Diagnosis can be delayed months or years if the treating provider has a low suspicion for OHVIRA syndrome and if the symptoms are relieved by NSAIDs or oral contraceptive pills [2,3,5]. This patient had been menstruating for two years due to a single unobstructed cervix/vagina. Untreated OHVIRA syndrome can have detrimental outcomes such as dysmenorrhea, chronic or cyclic pelvic pain, hematosalpinx, endometriosis secondary to retrograde menstruation, pelvic infection, pelvic adhesions, and subsequent infertility [2-8]. The definitive management is surgical and requires vaginal septum resection and drainage of any present hematocolpos or hematometra [3]. Some cases also report use of laparoscopy to confirm the diagnosis or to treat resulting endometriosis and adhesions, however this is not routinely performed and is not necessary for adequate treatment [3].
Most surgical repairs are now attempted with a single-stage rather than two-stage procedure [5]. In rare cases, patients were taken to the operating room a second time after a single-stage surgery due to incomplete resection of the vagina or stenosis of the upper vagina following initial resection [4]. Planned two-stage procedures are sometimes still performed in cases where the anatomy is extremely distorted or difficult to visualize due to hematocolpos [5]. Chronic inflammation and narrow vaginas in adolescents can further decrease visibility, leading some to advocate for the two-stage procedure [4]. In this method, the hematocolpos is drained in the initial surgery, and the remaining vaginal septum is only excised after a period of wound healing [4,5].
The exact method of hematocolpos drainage and vaginal septum resection is often not described in case reports and case series, but the classic method of vaginal septum resection is by sharp dissection followed by marsupialization of the cut edges [2,7]. However, with advancing surgical technology, various other techniques have since been introduced: unipolar needle electrodes, spinal needle aspiration, Seldinger technique, aspiration via suprapubic catheter, hysteroscopic resectoscopes, surgical staplers, bipolar energy devices, and hemihysterectomy with vaginectomy in rare cases of cervical atresia [3,5,8]. When the septum is resected using only sharp dissection, the septal edges can be either sutured together over the defect or marsupialized [2]. Using unipolar or bipolar energy devices for resection has the benefit of concomitant resection and hemostasis, but risks thermal injury to the vaginal tissue, the urethra, and potentially the bowel or bladder in the event of vaginal wall perforation. One case series describes a "No-Touch" technique for adolescent females with immature vaginal tissue. In this technique, vaginoscopy is employed, rather than vaginal retractors, in order to minimize trauma to the vaginal walls and limit postoperative pain [8]. Another case report describes the use of a gastrointestinal anastomosis (GIA) surgical stapler for the resection of a vaginal septum; this method achieved hemostasis during resection, and the staples were left in situ . The vaginal tissue was re-epithelialized over the staples at postoperative and longterm follow-ups [1]. The use of stents have also been described in order to decrease postoperative adhesions and septum reformation [8]. A 16 Fr Foley catheter has been used for this purpose in several cases; the Foley balloon was placed between the edges of the incised septum, inflated up to 80 ml of air, and then left in place for two days immediately postoperatively [8]. Similar positive outcomes have been noted with each of these methods [1-8]. With this information in mind, the decision was made to use LigaSure in the presented patient due to its ease of operation and ease of achieving hemostasis. Adequate visualization was obtained throughout the entirety of the septum excision, allowing for reasonable confidence that the vaginal sidewalls were not perforated, thereby avoiding thermal injury to the bowel and bladder.
Laparoscopy is considered the “gold standard” for diagnosis of OHVIRA syndrome, however it is no longer routinely performed in addition to vaginoplasty. In most cases, the diagnosis can be reached by history, physcial exam, and imaging; pelvic MRI has been particularly useful in confirming the diagnosis [1-8]. Endometriotic implants are visuallized in about 23% of OHVIRA syndrome patients, compared to 10-50% of the general population, however no clear association has been made between OHVIRA syndrome and endometriosis [2,4]. In the presented case, diagnostic laparoscopy was performed secondary to an adnexal mass demonstrated on imaging, and subsequent salpingo-oophorectomy became necessary for treatment of ovarian torsion. No endometriotic implants were noted at that time.
Postoperative complications are uncommon, but longterm follow-up of these patients is necessary to screen for complications such as dyspareunia, vaginal stenosis, and recurrence of obstruction [4,5]. Endometriosis that may have resulted from retrograde menstruation should also be addressed and treated appropriately. Infertility is overall rare in this patient population, with a pregnancy rate of approximately 80% [2,5,7]. However, obstetric complications can include premature birth, spontaneous abortion, fetal growth restriction, or fetal malpresentation [2,5,7]. Overall, most cases report favorable longterm outcomes without dyspareunia, dysmenorrhea, pelvic pain, or re-formation of the vaginal septum [1-8].
Consent to publish this case report was obtained by the patient’s legal guardian. This report does not contain any personal information that could lead to the identification of the patient.
The authors declare that there is no conflict of interest regarding the publication of this article.
The authors declare that there is no funding for this article. Case was performed as part of the employment of the authors by the University of Nevada Las Vegas and the U.S. Air Force.
All authors have contributed equally.