We describe a case of sudden complete urinary incontinence 20 days after pelvic floor surgery and mid-urethral sling operation.
An 81-year-old woman presented herself with disturbing stress urinary incontinence and symptomatic pelvic organ prolapse. 30 years before she had had an abdominal hysterectomy and presumably a colposuspension. To repair the symptomatic pelvic floor disorder the patient needed an anterior and posterior colporrhaphy, vaginal repair of enterocele and anterior rectocele. Additionally, a tension-free midurethral sling (retropubic tension-free vaginal tape) was implanted because of stress urinary incontinence. Seven days postoperatively she resumed the prophylactic intake of acetylsalicylic acid. The first follow-up 14 days after surgery showed a correct position of the sling and the patient was continent. 20 days later an acute vaginal vault hematoma and complete urinary incontinence occurred.
With insertion of a second sling the patient's urinary incontinence resolved. A late onset vaginal vault hematoma causing sling dislocation 20 days after surgery is extremely unusual.
The volume of the hematoma caused the dislocation of the retropubic tension-free vaginal tape, which resulted in complete urinary incontinence.
Once the retropubic tension-free vaginal tape is dislocated by hematoma, it might not be correctly placed anymore after its absorption.
Acute complete urinary incontinence, Dislocated tension-free vaginal tape by hematoma
Stress urinary incontinence is the involuntary leakage of urine during physical exertion, such as physical exercise, coughing or laughing [1]. Female stress urinary incontinence is either caused by urethral hyper mobility, intrinsic sphincter deficiency or the combination of both [2]. In the treatment of stress urinary incontinence, pelvic floor education is often not successful enough and surgical treatment may be required. Tension-free midurethral synthetic slings are a minimal invasive treatment of female stress urinary incontinence and the gold standard for surgical treatment of stress urinary incontinence. About 2000 sling procedures are performed in the USA every year [3]. This method has many advantages compared to other surgical techniques, in particular shorter operative and hospitalization times, reduced postoperative pain and less voiding dysfunction [4].The sling is placed under the middle portion of the urethra and on both sides retropubically, leading up to the abdominal skin above the pubis [4]. This technique was first described by Petros and Ulmsten in 1996 [5,6]. The success rate of the mid-urethral sling procedure is very high but the reported complication rates of up to 10% are significant [7]. Complications may occur immediately after surgery or at a later time point. Immediate complications may be incurred during surgery, such as injury of blood vessels, bowel, bladder, urethra or nerves. Subsequent postoperative complications may include urine retention, hematomas or infections. Late complications can occur weeks or months after surgery, such as urgency with or without incontinence, bladder outlet obstruction with recurrent urinary infections or mesh erosion [4]. A modification of the surgical technique is to place the mesh transobturator ally [8]. If urinary incontinence occurs in combination with a pelvic floor disorder, a combined treatment with pelvic floor surgery must be considered.
We present the case of acute complete urinary incontinence 20 days after pelvic floor surgery and mid-urethral sling operation. An informed consent of the patient has been obtained.
An 81-year-old woman presented at our clinic complaining of stress urinary incontinence and symptomatic pelvic organ prolapse. In the past, her stress urinary incontinence had been treated with a pessary until the pelvic organ prolapse increased to such an extent that the pessary dislocated repeatedly. Thirty years before presentation she had had an abdominal hysterectomy, presumably combined with a colposuspension. Clinical examination revealed vaginal vault prolapse, cystocele, enterocele and anterior rectocele with stool-outlet-obstruction. Urodynamic examination confirmed the severe stress urinary incontinence. Due to the combined pelvic floor disorders and stress urinary incontinence, the patient required a tension-free midurethral sling in the form of a retropubic tension-free vaginal tape, an anterior and posterior colporrhaphy as well as vaginal repair of the enterocele.
Seven days after the operation the patient resumed her usual intake of acetylsalicylic acid (100 mg) for prophylaxis against cardiac events. After an uneventful first follow-up examination 14 days after the surgery which included an unremarkable ultrasound examination demonstrating the correct position of the showing retropubic tension-free vaginal tape and a normal clinical examination, the patient reported back 20 days after the surgery with acute complete urinary incontinence. The clinical and sonographic examinations showed a newly developed hematoma of the vaginal vault and the anterior vaginal wall with dislocation of the retropubic tension-free vaginal tape (Figure 1). The hematoma and the tension free vaginal tape were clearly seen by transperineal and translabial ultrasound. Sonography allows dynamic imaging and the sling implants are highly echogenic [9]. In MR scan they are not clearly visible, except for MR-visible Fe3O4-mesh implants [10]. Four months later the hematoma had partially resorbed but the urinary incontinence was basically unchanged. The mid-urethral sling dislocation persisted (Figure 2). After seven months of persistent stress urinary incontinence and following the complete resorption of the hematoma a second retropubic tension-free vaginal tape was implanted (Figure 3). Before the second surgery a haematological examination for coagulation disorders was performed which showed minimally reduced thrombocyte aggregation function and the patient was instructed to stop taking the acetylsalicylic acid. The implantation of the second sling and the postoperative period were uneventful, resulting in complete resolution of her stress urinary incontinence without any further complications.
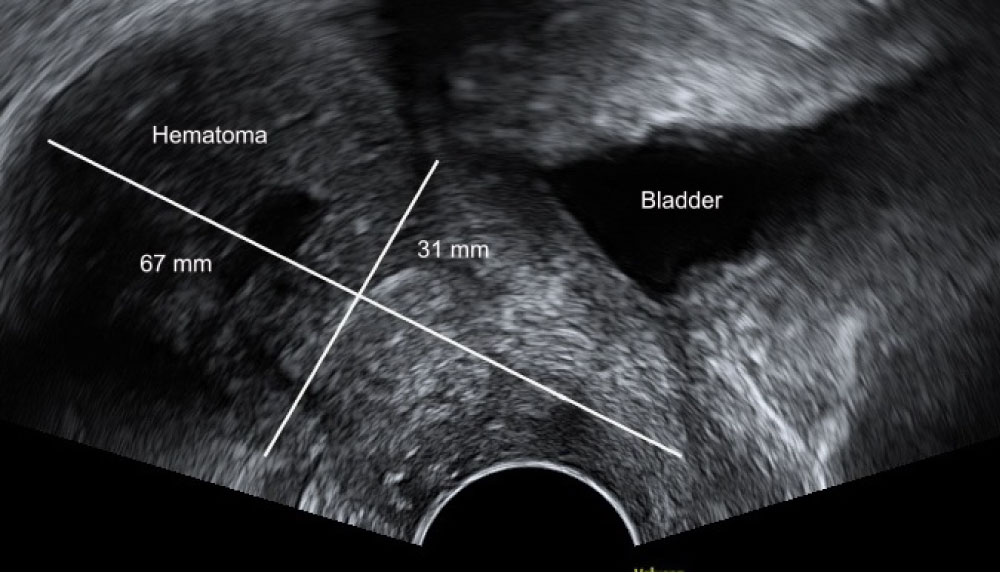 Figure 1: Hematoma 20 days after surgery.
View Figure 1
Figure 1: Hematoma 20 days after surgery.
View Figure 1
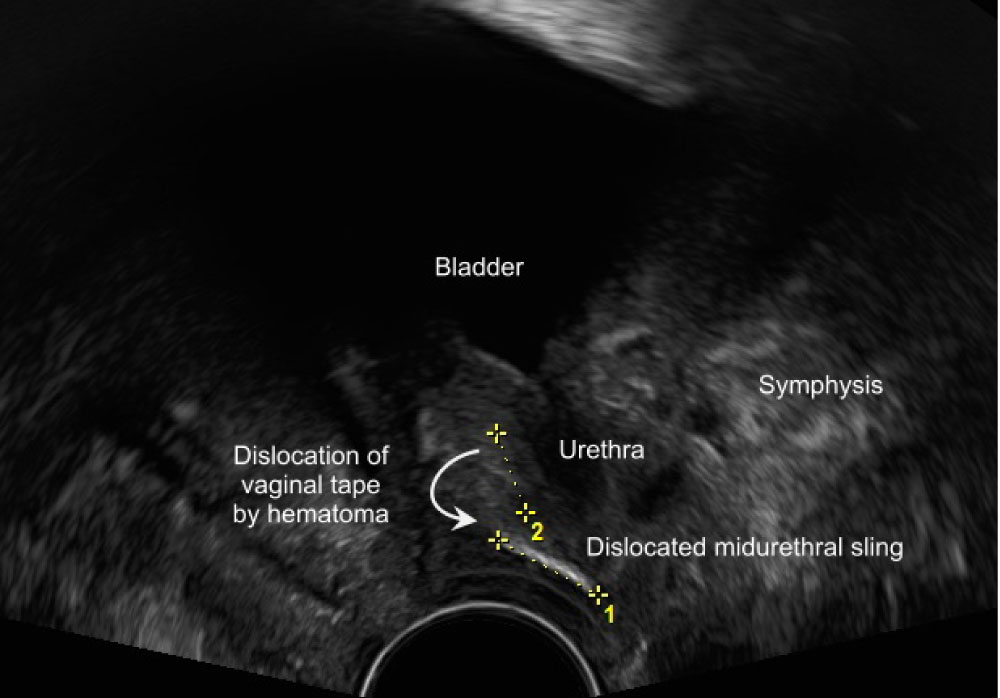 Figure 2: Dislocated tension-free vaginal tape.
View Figure 2
Figure 2: Dislocated tension-free vaginal tape.
View Figure 2
 Figure 3: 1) Dislocated tension-free vaginal tape; 2) Correctly placed second tension-free vaginal tape.
View Figure 3
Figure 3: 1) Dislocated tension-free vaginal tape; 2) Correctly placed second tension-free vaginal tape.
View Figure 3
The occurrence of vaginal vault hematoma 20 days after pelvic floor repair is extremely unusual even in combination with the intake of acetylsalicylic acid. The isolated hematological abnormality of slightly reduced thrombocyte aggregation is unlikely to be the only cause of the hematoma of the vaginal vault and the anterior vaginal wall. However, this disturbance, in combination with the intake of acetylsalicylic acid, could have favored the formation of the hematoma. The preoperative blood count and standard coagulation parameters were normal and she did not complain about having had any hemorrhagic diathesis even during the intake of acetylsalicylic acid in the past. Further on she had no committed medication which could have impaired the platelet function. In absence of any history of hemorrhagic diathesis like prolongation of bleeding time, extended haemostasis screening is not urgently recommended. Even after the unusual hematoma the hematological examination for coagulation disorders was not conclusive. The detected slightly reduced thrombocyte aggregation had no clinical significance [11]. Nevertheless there remains, in a similar case like ours, the possibility to verify the indication for prophylactic acetylsalic acid intake. For it is proved that the intake of low-dose acetylsalic acid does not significantly decrease the cardiovascular risk in elderly people but increases the risk of hemorrhage [12].
The volume of the hematoma caused the subsequent dislocation of the retropubic tension-free vaginal tape, which then resulted in acute complete urinary incontinence. Nevertheless, even after resolution of the hematoma, the stress urinary incontinence persisted.
Mid-urethral sling procedures are the gold standard to treat stress urinary incontinence. The cumulative cure rates of the transobturator tape and retropubic vaginal tape are higher than 60% [13]. Recurrent or persistent stress urinary incontinence occurs due to suboptimal vaginal tape placement, especially when the mid-urethral sling is placed too close to the bladder neck [14]. In case of persistent stress urinary incontinence the recommended therapeutic procedure is a second implantation of a retropubic tension-free vaginal tape with or without excision of the first mid-urethral sling. In the literature a success rate of more than 70% after the implantation of a second tension-free vaginal tape has been reported [15,16].
Postoperative hematomas occur frequently after retropubic tension-free vaginal tape placement. They are rarely symptomatic if the volume of the hematoma is less than 100 ml. In contrast, large hematomas often need surgical evacuation [4,17,18]. The chance of damaging a blood vessel, in particular the perivesical venous plexus, in the space of Retzius exists due to the blind procedure of passing the trocar through this area to the abdominal wall. Life-threatening consequences may even occur in the rare case of massive hematoma [18].
Tension-free midurethral synthetic slings are a minimally invasive and the gold standard for surgical treatment of female stress urinary incontinence. The success rate is very high but the reported complication rates of up to 10% are significant [7]. The presented case is special because it is the first to describe the occurrence of a vaginal vault hematoma 20 days after surgery, resulting in the dislocation of the retropubic tension-free vaginal tape and the development of acute urinary incontinence.
Once a retropubic tension-free vaginal tape has been dislocated by an adjacent hematoma, it may not return to its original location even after complete resorption. If the stress urinary incontinence persists, the placement of a new retropubic tension-free vaginal tape should be considered. The success rate of a second mid-urethral sling procedure is more than 70% [15,16].
We thank Dorothy Huang for her critical assessment and proofreading of this manuscript. The contents of the manuscript have been presented at the 25th World Congress on Controversies in Obstetrics, Gynaecology and Infertility (COGI) in Vienna in 2017 as an e-poster without presentation. The authors report no conflict of interest.