Percutaneous nephrolithotomy, Rare complications of PCNL, Stripped glide wire
The prevalence of nephrolithiasis has been on rise worldwide and the Percutaneous Nephrolithotomy (PCNL) has offered solution to any type of kidney stone [1]. Although less invasive procedure, complications are known to occur during PCNL. Most of urologists are well versed with the predictable complications of PCNL like bleeding, surrounding organ injury, collecting system injury, sepsis, stricture formation and nephrocutaneous fistula [2]. Many unusual complications can occur during procedure that can test the intellect and patience of the surgeon. We report stripping of glide wire during PCNL, a rare complication, and procedure to remove it percutaneously.
A 32-year-old male underwent PCNL for renal pelvic calculus extending into the middle calyx. A middle calyceal puncture was made but glide wire could not be safely parked into the Pelvicalyceal system (PCS). After repeated attempts to pass the guide wire into the collecting system, guide wire was removed with puncture needle in place. During removal the jacket of the glide wire got stripped and lost into the renal parenchyma. Another calyceal puncture was made and tract dilated and stone was removed. There was no endoscopic trace of the stripped glide wire in the PCS, though it was visible in fluoroscopy. Every calyx was searched but the stripped wire could not be seen. A DJ stent and nephrostomy tube was placed and procedure abandoned. Postoperative X-ray was showing the stripped glide wire coiled in the renal area (Figure 1). After two days patient was again taken to Operation Theater after proper planning to remove the residual glide wire. Under fluoroscopic guidance the puncture was made directly on the stripped wire (Figure 2). A new glide wire was into the PCS under fluoroscopic guidance. Tract was dilated to 12 Fr and 8.5 Fr ureteroscope was passed through the sheath. The stripped wire was identified (Figure 3) and removed intact (Figure 4). Postoperative period was uneventful.
 Figure 1: X-ray KUB showing coiled stripped glide wire fragment (white circle).
View Figure 1
Figure 1: X-ray KUB showing coiled stripped glide wire fragment (white circle).
View Figure 1
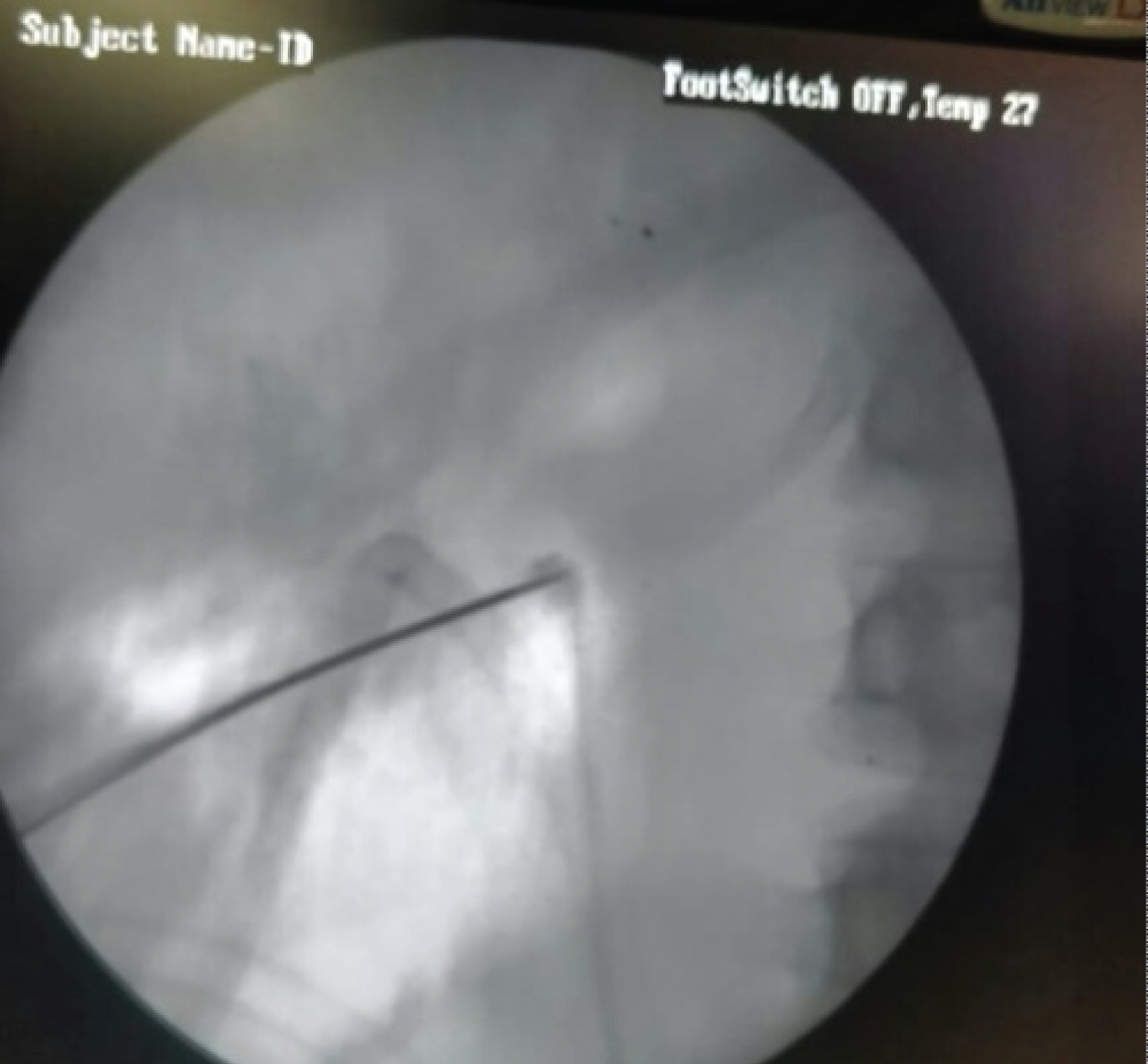 Figure 2: Fluoroscopic puncture made directly on the glide wire fragment.
View Figure 2
Figure 2: Fluoroscopic puncture made directly on the glide wire fragment.
View Figure 2
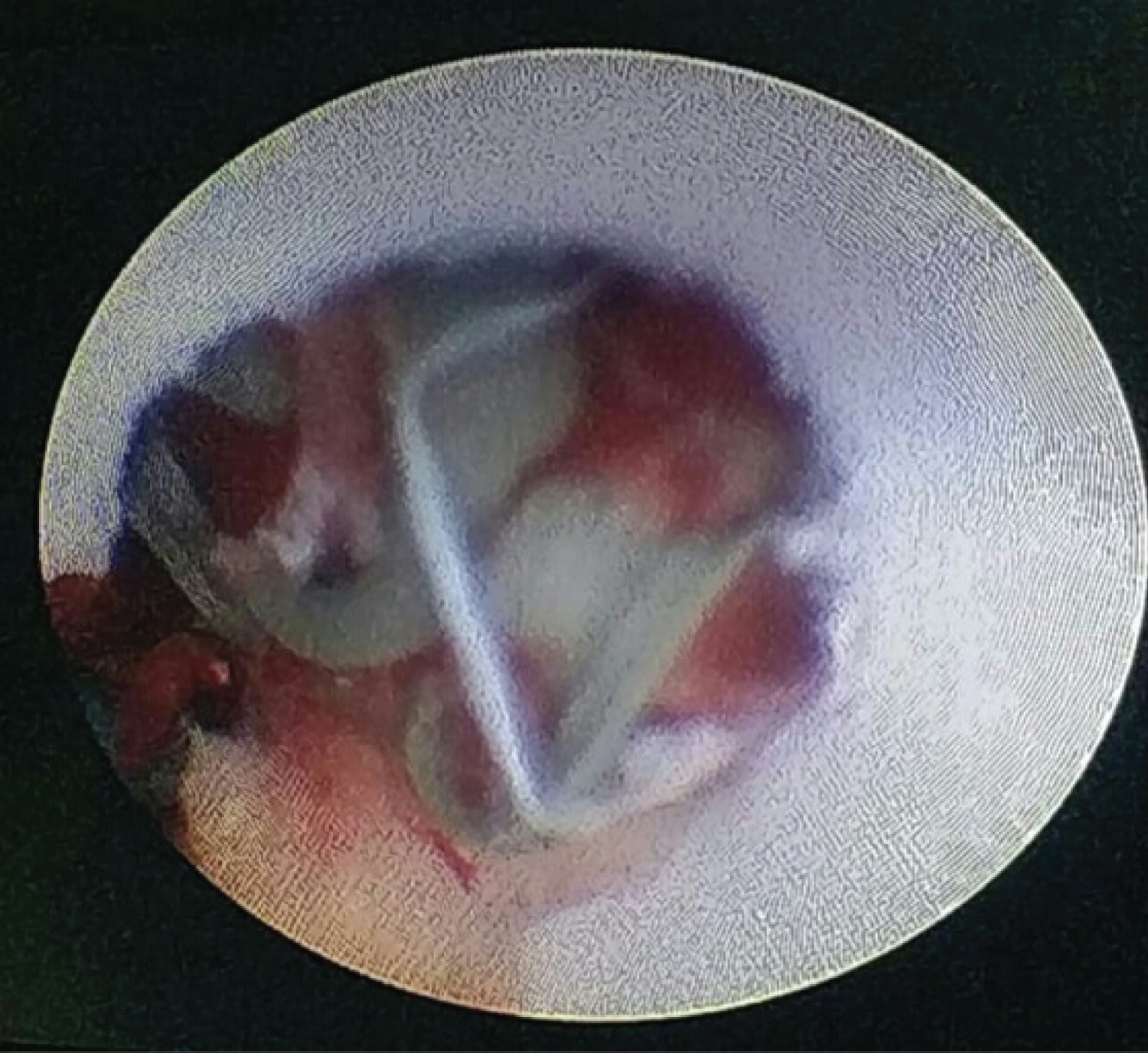 Figure 3: Endoscopic view of glide wire jacket.
View Figure 3
Figure 3: Endoscopic view of glide wire jacket.
View Figure 3
 Figure 4: Glide wire jacket removed intact.
View Figure 4
Figure 4: Glide wire jacket removed intact.
View Figure 4
PCNL being standard treatment for large size renal calculi also promises the ultimate solution to renal calculi refractory to other treatment modalities like hard stones, lower pole stones with non feasible calyceal anatomy and stones in anatomically abnormal kidneys.
Although being less invasive procedure, complications do occur in PCNL. The commonly occurring complications of PCNL are bleeding, surrounding organ injury Pelvicalyceal system perforation, sepsis, etc [3]. Most of the urologists who perform PCNL routinely are familiar with these complications. They are mostly easy to recognize and have defined management protocol. Difficulty arises when an unusual complication occurs because the surgeon is not prepared for the same. These rare complications are difficult to recognize and manage. They usually test the patience and intellect of the surgeon. We faced a rare complication of stripping of glide wire during PCNL. Although it was easily recognized but we were not prepared to rectify it instantly and procedure was already prolonged.
The Terumo hydrophilic Glide wire we use consists of super-elastic nitinol alloy core for optimal performance and kink resistance. Tungsten-infused polyurethane jacket provides superior tip and wire radiopacity [4]. When coiled guide wire is pulled forcibly the jacket may get stripped from the nitinol core by the edge of the puncture needle. Attempts to localize the stripped glide wire failed endoscopically since the fragment was lost in the renal parenchyma. Such a fragment may even be difficult to identify in open surgery. Already exhausted by the attempts to identify the lost glide wire and prolonged operative time, procedure was abandoned with the aim of coming back after proper planning. The stripped glide wire was targeted under fluoroscopic guidance and small tract was carefully dilated up to the coiled jacket and removed intact under vision.
Glide wires and all accessories should be carefully used during endourologic procedures. Glide wire should not be removed forcibly through the puncture needle to avoid stripping. All accessories should be properly examined before and after the procedure to recognize any lost part. Stripped glide wire fragments can be safely removed percutaneously under fluoroscopic guidance.
None.
None.