Hypertension and diabetes mellitus are chronic medical conditions that frequently coexist. Our objective is to evaluate the effect of Angiotensin converting enzyme inhibitors and Angiotensin II receptor blockers comparatively and in integration with Metformin, dipeptidyl 4 inhibitors and insulin on lipid profile, serum creatinine, liver enzymes and electrolytes in type II diabetic patients.
Data of the study were collected from clinical reports of 100 hypertensive patients with type II diabetes from Taif Diabetic Center. Male and non-pregnant female with an average age (55 ± 10 years) who's treated with ACE Inhibitors and ARBs were our target.
Our results recorded that, ARBs significantly increase AST in compared to ACE inhibitors while chloride level decrease with ACE inhibitors in compared to ARBs.
On other hand, when we compared the effect of ACE/ARBs in combined with antidiabetic agents Significant increase in TC was recorded with ACE inhibitors + Metformin, also LDL was increase with ACE inhibitors + insulin while ARBs + Insulin was increase HDL. Serum creatinine increased in both groups used Insulin. ALT was significantly increases with ARBs + Metformin + DPP-4 inhibitors.
Electrolytes were affected during the combination with antidiabetic agents, Sodium level was increased with ARBs + Metformin + DPP4 inhibitors and potassium was increase with ARBs + Insulin.
There are slight effects on selected biochemical parameters was recorded during the treatment with ACE inhibitors and ARBs separately and when combined with antidiabetic agents.
Anti diabetic agents, Antihypertensive agents, Biochemical parameter, Diabetic patients, Taif city
Hypertension and diabetes mellitus are chronic medical conditions that frequently coexist. Obesity, high sodium diet and inactivity are predisposing factors for both hypertension and non-insulin-dependent diabetes mellitus [1].
The hypertensive patient with type II diabetes is especially at risk of adverse cardiovascular events, because diabetes adversely affects the arteries, predisposing them to atherosclerosis (narrowing of the arteries) [1].
There are many studies conducted to detect the effect of antihypertensive agents on cardiovascular events. The United Kingdom Prospective Diabetes Study (UKPDS) and Hypertension Optimal Treatment (HOT) studies suggested that treatment to a lower target blood pressure resulted in better prevention of clinical disease in these patients [2]. Most trials comparing antihypertensive agents have shown only minimal differences between the various agents. The evidence from the trials suggests that angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers ARB), calcium channel blockers (CCBs), beta-blockers and diuretics will all successfully reduce adverse clinical events. While only limited studies have been reported to detect the effect of antihypertensive on different biochemical parameters in diabetic patients [2]. So our study was designed to detect the effect of antihypertensive agents, separately, comparatively or in integration with antidiabetic agents on some biochemical parameter in type II diabetic patients.
Clinical biostatistical study.
Clinical reports of male and non-pregnant female diabetic patients in Taif Diabetic Center (TDC) which diagnosed with hypertension were investigated by us. Out of 325 clinical reports only 100 reports (49 male and 51 female) were included in our study regarding to the following criteria: 1) Age : our study determine age from 45 to 65 years with average (55 ± 10) as the incidence of diabetes mellitus type II mostly occur in this age [3]. 2) Pregnancy: pregnant female was excluded as pregnancy has some physiological biochemical changes. 3) Patients with nephropathy were excluded from our study as kidney function test was one of our testing parameters. 4) Completed clinical biochemical lab reports for three successive follow ups with (3-4 months) time interval. 5) Drugs: patients only treated with monotherapy antihypertensive drug were involved in our study to prevent factor of drug interaction as it isn't from our aim. Among all hypertensive classes only ACE inhibitors and ARBs mostly prescribed in (TDC), so our study conducted on them. Antidiabetic agents were recorded for detecting the underline effects of combination between antihypertensive drugs and antidiabetics agents on biochemical parameters.
Our study concerned with some clinical parameter as (Lipid profile [LDL, HDL, Total cholesterol], renal function parameter [SrCr], liver function parameters [AST, ALT, Albumin] and electrolytes [Na, K, Cl]).
All our data was collected in data sheet.
All data was represented as mean ± Stander Error (SE). Data was analyzed by using three different methods of statistical analysis:
A) One way ANOVA was used to analyze the effects of ACE inhibitors and ARBs separately on our biochemical parameters for three consecutive follow ups.
B) T-paired test used to compare between the effects of ACE inhibitors and ARBs on biochemical parameters during 3 consecutive follow ups.
C) Two way ANOVA was used to estimate the effects of both antihypertensive and antidiabetic agents on our biochemical parameters during three consecutive follow ups. One and two way ANOVA followed by Least Significance Difference (LSD) as a multiple comparison. Differences in one and two way ANOVA were considered significant at P < 0.05, while paired t-test differences were considered significant at P < 0.025. All statistical analysis were done using statistical package for social science software (SPSS 22) [4].
Different biochemical parameters (Lipid profile, renal function parameter, liver function parameters and electrolytes) were reported from patients records to evaluate the effect of antihypertensive agents ACE inhibitors and ARBs in type II diabetic patients.
Our result recorded that ACE inhibitors and ARBs separately have not any effect on TC, TG, LDL and HDL during the three follow ups.
Our result recoded that, ACE inhibitors + Biguanide significant increase (P < 0.05) TC in compared with ACE inhibitors + Insulin only. And it significantly increases (P < 0.05) LDL level in compared to other groups (in second follow up) (Table 1).
Table 1: Effect of ACE inhibitors and antidiabetic agents on lipid profile during 3 consecutive follow ups. View Table 1
On other side, we recorded significant increase in ARBs+ Insulin when it compared with ARBs + Biguanide (in first follow up) (Table 2).
Table 2: Effect of ARBs and antidiabetic agents on lipid profile during 3 consecutive follow ups. View Table 2
ACE inhibitors and ARBs have no any effect on renal function (SrCr) was recorded between the two different classes and even by time in each one separately.
Our result recorded that the ACE inhibitors + Insulin significantly increase SrCr (P < 0.05) in compared to the other groups (in first and second follow up) (Table 3).
Table 3: Effect of ACEI and antidiabetic agents on SrCr during 3 consecutive follow ups. View Table 3
On other side, ARBs + Insulin recorded significant increase in SrCr in compared to both groups (in second follow up). While it was increase in compared to ARBs + Bigunaide + DPP-4 inhibitors only in third follow up. (Table 4).
Table 4: Effect of ARB and antidiabetic agents on SrCr during 3 consecutive follow up. View Table 4
Our result showed that liver enzymes Alanine transaminase (ALT), Aspartate transaminase (AST) and serum albumin were not affected by ACE inhibitors and ARBs by time separately during 3 consecutive follow ups.
While significant increase in AST level in first follow up (p < 0.02) was detected in ARBs compared to ACE inhibitor (Figure 1).
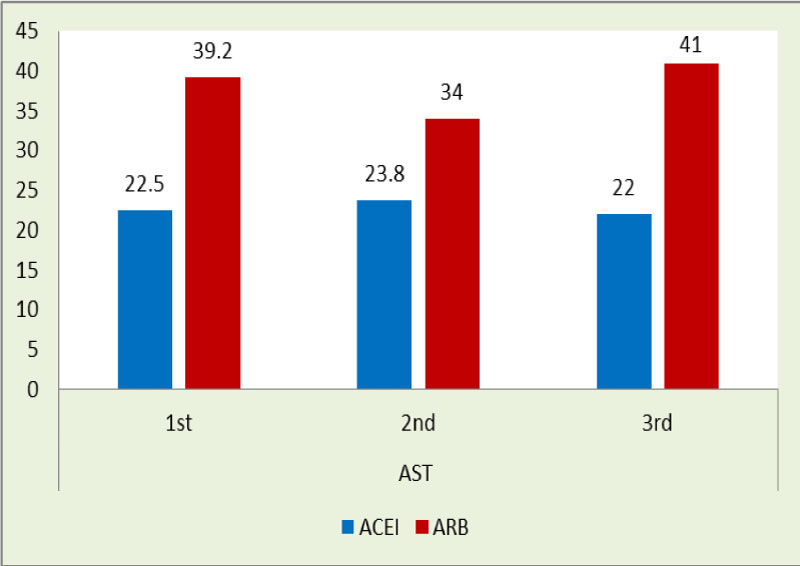 Figure 1: Effect of ACEI and ARB on AST enzymes during 3 consecutive follow ups.
View Figure 1
Figure 1: Effect of ACEI and ARB on AST enzymes during 3 consecutive follow ups.
View Figure 1
In our study we recorded that the combination between ACE inhibitors and antidiabetic agents had no significant effect on liver function.
On other side ARBs + Bigaunide + DPP-4 inhibitors had significant increase on ALT in second follow in compared to the ARBs+ Insulin (Table 5). Also albumin level was significantly increase in ARBs + Bigaunide + DPP-4 inhibitors in compared to both groups in first follow up. While it was significantly increase in compared to ARBs + Insulin only in second and third follow up.
Table 5: Effect of ARBs and antidiabetic agents on liver functions during 3 consecutive follow up. View Table 5
Our result recorded that there was a significant increase in chloride level (Cl) only was found in first follow up in compared to second and third follow ups during the treatment with ACE inhibitors (Figure 2). While electrolytes (sodium Na, Chloride Cl and potassium K) were not affected by time during the treatment with ARBs. On other hand significant decreased (P < 0.003) in chloride level only in second follow up in patient who are treated with ACE inhibitor in compared to ARB (Figure 2).
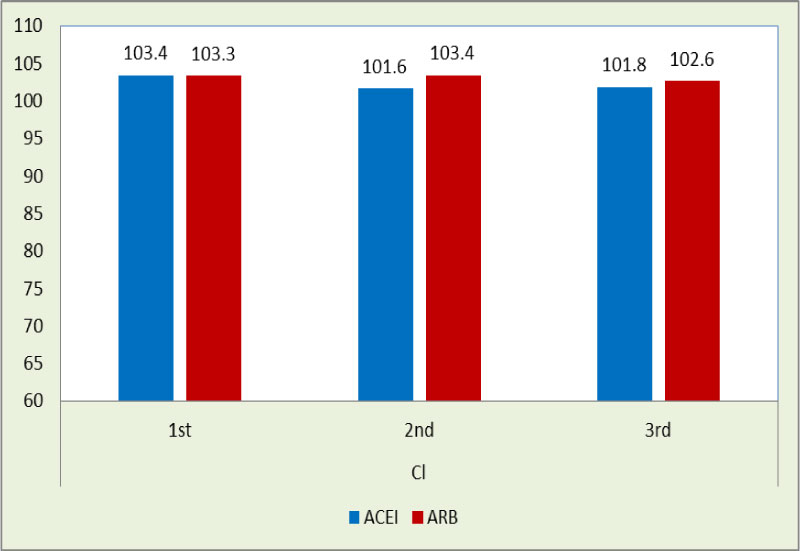 Figure 2: Effect of ACEI on Cl during follow up during 3 consecutive follow ups.
View Figure 2
Figure 2: Effect of ACEI on Cl during follow up during 3 consecutive follow ups.
View Figure 2
Our result documented that there is no any effect on electrolytes when we combined the ACE inhibitors with antidiabetic agents.
While sodium level was significantly increase in ARBs + Biguanide + DPP-4 inhibitors in compared to ARBs + insulin in first follow up (Table 6 and Figure 3).
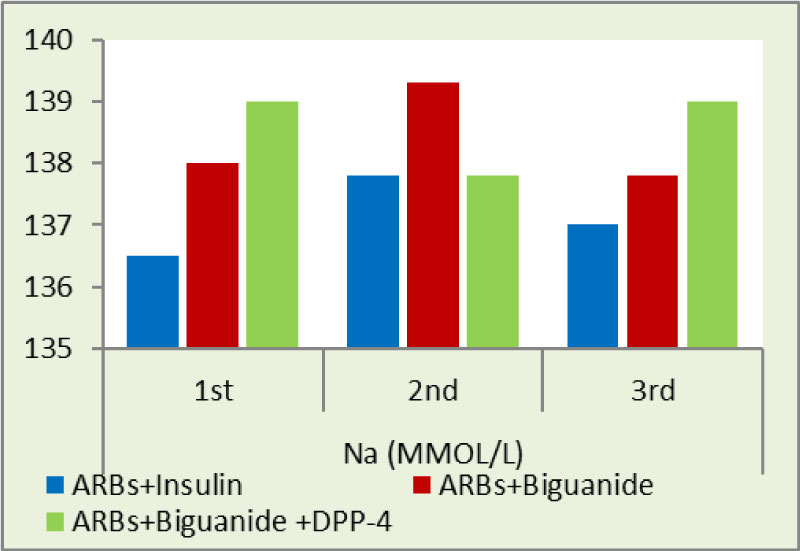 Figure 3: Effect of ARB and antidiabetic agents Na during 3 consecutive follow ups.
View Figure 3
Figure 3: Effect of ARB and antidiabetic agents Na during 3 consecutive follow ups.
View Figure 3
Table 6: Effect of ARBs and antidiabetic agents on electrolytes during 3 consecutive follow ups. View Table 6
Also potassium level was significantly increase in ARBs + Insulin in compared ARBs + Biguanide in second and third follow ups (Figure 4).
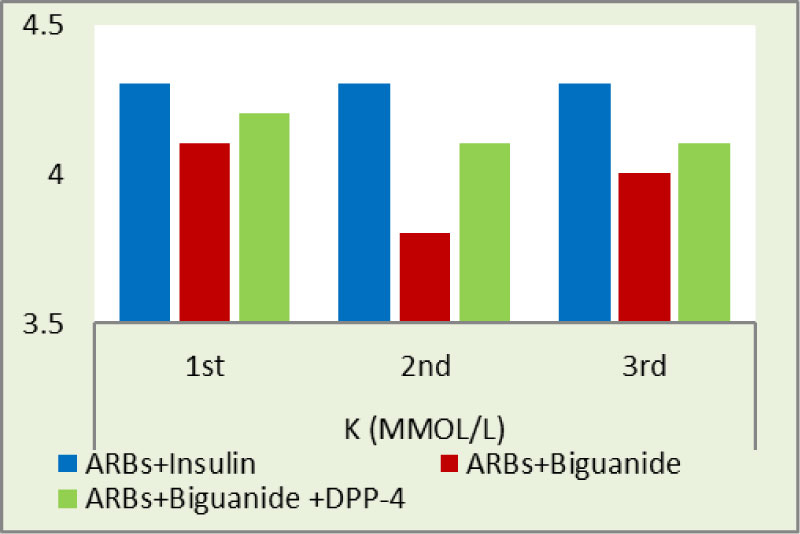 Figure 4: Effect of ARB and antidiabetic agents K during 3 consecutive follow ups.
View Figure 4
Figure 4: Effect of ARB and antidiabetic agents K during 3 consecutive follow ups.
View Figure 4
Our study is one of novel studies that concern with the effects of mono antihypertensive agents (ACE inhibitors and ARBs) during 3 consecutive follow ups (3-4 months interval) in hypertensive type II diabetic patients. As well as Their underline effects (ACE inhibitors and ARB) in a combination with antidiabetics agents (insulin or Biguanide or Biguanide plus DPP-4 inhibitors) on the biochemical parameters (lipid profile, renal function parameter ,liver function parameters and electrolytes electrolytes) in three consecutive follow ups.
Regarding lipid profile, our result noticed that, there is no significance on TC, TG, LDL and HDL levels during the treatment with ACE inhibitors and ARBs. This disagree with Mohamad Alblihed and Husni Farah [5,6] which reported significant increase in TC and TG levels in post-treated patients with captopril (ACE inhibitors) compared with the control subjects.
On other side when we compared the effect of ACE inhibitors in combination with antidiabetic agents we recorded significant increase (P < 0.05) in TC with ACE inhibitors + Biguanide (208.8 ± 20.2) in compared with ACE inhibitors + insulin (157.2 ± 7.9) in second follow up. Also LDL level was significantly increase in ACE inhibitors + Biguanide (141.4 ± 21.6) in compared to ACE inhibitors + Insulin and ACE inhibitors + Biguanide + DPP-4 inhibitors (96.5 ± 6.9), (104.3 ± 6.9) respectively in second follow up. While HDL level was significantly increase in ARBs + Insulin (46.2 ± 3.5) in compared to ARBs+ Biguanide (36.5 ± 2.2) in first follow up.
Our result recorded that, the mean Serum creatinine levels were almost stable during the 3 consecutive follow ups. Jahnavi and Ervilla [7] partially agree with us as they reported that, ARBs stabilized serum creatinine during the treatment (1.97 ± 1.19), (1.96 ± 1.15), (1.97 ± 1.32) for three months respectively. Our result disagree with Mohamad Alblihed and Husni Farah [5,6] which founded significant increase in Serum Creatinine (1.33 ± 0.13) in patient treated with ACE inhibitors in comparison to control group. They were refer the increase in SrCr to the biological effects.
On other hand our result was supported by peter [8] as they recommended for using ACE inhibitors and ARBs in diabetic patients as they offer a protection against nephropathy through a specific effect on the renal microcirculation by reducing intraglomerular pressure.
The combination between ACE inhibitors and antidiabetic agents recorded a significant increase (p < 0.05) of serum creatinine in ACE inhibitors + Insulin (1.0 ± 0.0) in compared to both groups (0.8 ± 0.0) in first follow up and (0.7 ± 0.0) in second follow up.
Also significant increase in SrCr in second follow up was documented with ARBs + Insulin (1.0 ± 0.0) in comparison to both groups (0.8 ± 0.0). While in third follow up ARBs + Insulin significantly increase (1.0 ± 0.1) in compare to ARBs + Biguanide + DPP-4 inhibitors (0.8 ± 0.0).
The high SrCr level in patients treated with insulin who is resistant to oral antidiabetic agents in both groups can be referred to long term uncontrolled diabetes. Which can lead to the complication of microvascular disease (nephropathy) [9].
Regarding liver function test; liver enzyme AST was significantly increased in patients who is treated with ARBs (43.9 ± 6.1) in compared to ACE inhibitors (23.4 ± 2.5) in first follow up while ALT and Albumin were not affected. This result was supported by Kim and Douglas [10] reported that the ARBs have been associated with a minimal rate of serum enzyme elevations during therapy which are usually mild-to-moderate in severity, self-limited, and rarely require dose modification or discontinuation. In contrast to our study; Lina, et al. [11] recorded that, the use of ACE inhibitors lead to moderate increase in the liver enzymes in some patients, ALT and AST were increase by (11.18%) without any symptom of hepatotoxicity.
By studying the effect of combination between ACE inhibitors and antidiabetic agents on liver function test we noticed that ALT, AST and albumin didn't affect. While significant increase in ALT level was recorded in ARBs + Biguanide + DPP-4 inhibitors (72.1 ± 14.1) in compared to ARBs+ Insulin (37.7 ± 10.1) in second follow up. Also albumin level was significantly increase in ARBs + Biguanide + DPP-4 inhibitors (4.1 ± 0.1) in compared to both groups (3.5 ± 0.2) in first follow up. While in second and third follow up recorded significant increase in ARBs + Biguanide + DPP-4 inhibitors (3.8 ± 0.1) when compared to ARBs+ Insulin (3.4 ± 0.1) (3.3 ± 0.2) respectively. Really by condensed research we didn't stop for any research can explain this result which may be due to the effect of antidiabetic agent, but why this effect not appear with ACE inhibitors? We can't explain that in this moment as we need further supporting pharmacokinetic and clinical studies to help us.
To study the effect of electrolytes we were select sodium (Na), chloride (Cl) and potassium (K) in our study because those are the most common macro electrolytes and correlated with diabetes mellitus.
When we compared the effect of ACE inhibitors and ARBs on electrolytes we founded that Chloride level was affected by time. It is significantly decrease in second (101.6 ± 0.5) and third (101.8 ± 0.5) follow ups with ACE inhibitors in compared to first follow up (103.4 ± 6) while ARBs not affected. However by comparison between ACE inhibitors and ARB significance decreased (p < 0.03) in second follow up was detected in ACE inhibitor (101.6 ± 0.5 vs. 103.4 ± 0.3). While Na and K were not affected.
Some study report that diabetic patients may have hyperkalemia when ACE inhibitors or ARBs are started. This is particularly likely in diabetic patients with baseline renal insufficiency and estimated glomerular filtration rate < 30 ml/minute .This explain why the K level was not affected in our result because patients with CKD were excluded from our study [12]. Also Seyed, et al. [13] recorded that Hyperkalemia is more common with ARBs than ACE inhibitors.
By combination of ACE inhibitors and antidiabetics agents; electrolytes level have not reported any significance. While sodium level was significantly increase in ARBs + Biguanide + DPP-4 inhibitors (139 ± 0.8) in compared to ARBs + Insulin (136.5 ± 0.7) in first follow up. Also significant increase in K level was detected with ARBs + Insulin (4.3 ± 0.1) in compared to ARBs + Biguanide in second and third follow ups (3.8 ± 0.1), (4.0 ± 0.1) respectively. The increase in K level in patients treated with Insulin + ARBs can be due to the deterioration in renal function as in our result the same group record increase in serum creatinine. This explanation was supported by other previous study [14].
First, Small samples size refer to incomplete data in patient records due to absence of patient in the appointment or in complete laboratory results.
Second, Some results may be affected by patients adherence to the medications, uncontrolled factors as diet and Body mass index (BMI). Although BMI was collected in our data sheet but we can't use it as a factor as it will highly restricted our samples number.
Third, Newly patients files: As Taif Diabetic Center was opened from one and half year only; our biochemical interval period was limited (3-4 months interval).
Our results clarified slight effect of ACE inhibitors and ARBs on selected biochemical parameters during 3 consecutive follow ups. While heterogeneous effect was noticed in some biochemical parameters levels by combination between antihypertensive and antidiabetics agents, which may be depend on some physiological, nutritional, medications adherence or other factors related to patients them self which not under our control. So more pharmacokinetic and clinical studies needed to support and explain this heterogeneity.