Background: Early research and data on Coronavirus disease 2019 (COVID-19) have proven that pediatric clinical forms are not serious in many cases. However, the disease can progress to acute respiratory distress syndrome (ARDS) and multi-organ dysfunction and lead to death. In the present paper, we report one of the first Tunisian critical pediatric cases, a 6-year-old girl with an atypical ARDS secondary to severe acute respiratory syndrome coronavirus 2 (SARS-CoV2) that was supported by non invasive ventilation (NIV) and high flow oxygenation without the use of mechanical ventilation.
Observation: The patient presented with a five-day history of coughing and fever. The examination revealed marked inter and subcostal airflow, an Oxygen Saturation (O2 Sat) of 86% on room air, and 60 cycles per minute respiratory rate. She presented with some wheezing and cyanogenic coughing fits and her temperature was 38.6°C. Laboratory evaluation revealed elevated markers of inflammation. The patient progressed to respiratory failure and testing results for ARDS. The reverse transcriptase for SARS-CoV2 (RT-PCR SARS-CoV2) was positive. A thoracic computed tomography scan first suggested SARS-CoV2 infectious lung disease affecting almost half of the lungs associated with atelectasis in the bilateral inferior bases. The patient's ARDS was managed with non-invasive ventilation and after high flow oxygenation.
Conclusions: Given that severe pediatric COVID-19 is rare, this case report can guide pediatricians in the clinical course and management considerations as this pandemic continues to spread.
Severe acute respiratory syndrome, SARS-CoV2, COVID-19, Child, Pediatric intensive care, Critical, Acute respiratory distress syndrome
ALT: Alanine Aminotransferase; ARDS: Acute Respiratory Distress Syndrome; AST: Aspartate Aminotransferase; BMI: Body Mass Index; COVID-19: Coronavirus Disease 2019; CPK: Creatine Kinase; CRP: C-Reactive Protein; FiO2: Fraction of Inspired Oxygen; HCM: High Concentration Oxygen Mask; HFO: High Flow Oxygenation; IOTF: International Obesity Task Force; LDH: Lactate Dehydrogenase; NIV: Non-Invasive Ventilation; O2 Sat: Oxygen Saturation; PCT: Procalcitonin; PEEP: Positive End Expiratory Pressure; Pro-BNP: Pro Brain Natriuretic Peptide; PTT: Prothrombin Time; RT-PCR SARS-CoV2: Reverse Transcriptase for SARS-CoV2; SARS-CoV2: Severe Acute Respiratory Syndrome Coronavirus 2; SaO2: Arterial Oxygen Saturation
The whole world is facing a pandemic of new coronavirus infection, SARS-CoV2, named COVID-19. This has resulted in a significant increase in the number of hospitalizations, especially in intensive care units, with many deaths, mainly among the elderly population. Early data from the global COVID-19 pandemic revealed that children accounted for less than 5% of detected cases [1], and the clinical forms of pediatric cases were mostly minor, moderate, or even asymptomatic. Those findings created a sense of complacency about the impact of COVID-19 on the health status of children. Nevertheless, rare severe (less than 6%) and critical (less than 1%) pediatric cases have been reported since then [2] and paediatricians need data and sharing of experience regarding the management of these patients.
In the present paper, we report one of the first Tunisian critical pediatric cases, a 6-year-old girl with an atypical ARDS secondary to SARS-CoV2 to inform pediatric providers on the clinical course and management considerations as this pandemic continues to spread.
This female patient, aged 6 years and 5 months, was admitted to a tertiary hospital on October 18, 2020, for acute dyspnea with fever. She was from non-consanguineous parents and without a family medical history. She was a first-grade basic education pupil. The parents reported they had used oral corticosteroids for coughing episodes with fever, but she was not considered an asthmatic child. In addition, the child did not give a history of contact with a person with confirmed SARS-CoV2 infection. On examination, the child presented with a five-day history of coughing and fever. The patient was hospitalized in a pediatric intensive care unit.
The initial examination revealed a Body mass Index (BMI) of 23 kg/m2. Therefore, she was classified as obese: BMI ≥ L'International Obesity Task Force (IOTF)-30 threshold for her age. She was restless. The capillary blood glucose was 0.9 g/l and her temperature was 38.6°C. The tonsils were enlarged, blood pressure was 100/60 mmHg, heart rate was 120 beats per minute and the respiratory rate was 60 cycles per minute. She presented with some wheezing and cyanogenic coughing fits.
The examination revealed marked inter and subcostal airflow, an O2 Sat of 86% on room air, and 94% on HCM at 8 L/min and diffuse sibilant rales in both lung fields on auscultation. The rest of the examination was normal. Severe exacerbation of asthma was suspected. Chest radiography showed chest distension with diffuse bilateral alveolar opacities, the cardio thoracic index was 0.56 (Figure 1). The blood count showed a hyperleucocytosis of 14800/mm3 with neutrophils = 11600/mm3, lymphocytes = 2300/mm3, eosinophils = 1000/mm3, hemoglobin = 13.3 g/dL and platelets = 324000/mm3, C-reactive protein (CRP) = 45 mg/L; procalcitonin = 0.55 ng/mL. The initial arterial blood gas test under 8 liters oxygen by HCM yielded the followings: pH = 7.42; pO2 = 69 mmHg, pCO2 = 32 mmHg, HCO3- = 22.6 mmol/L and SaO2 = 94%. Initially, the child was treated for severe asthma exacerbation. She received oxygen by HCM at 8 L/min, methylprednisolone 2 mg/kg then 1 mg/kg/6 hours; nebulizations of Terbutaline and Ipratropuim bromide. Given the severity of the picture and the epidemiological context, a SARS-CoV2 infection was suspected at the very beginning of her care. Therefore, a diagnostic RT-PCR Covid-19 test was performed and it was strongly positive with low cycle threshold (Ct) value. A second biological checkup was ordered. It revealed the following findings: a prothrombine time (PTT) = 52%, TCK = 26 seconds, Ferritinemia = 149 ng/mL, Creatine kinase (CPK) = 27 IU/L, Lactate dehydrogenase (LDH) = 169 IU/L, Aspartate aminotransferase (AST) = 15 IU/L, Alanine aminotransferase (ALT) = 25 IU/L, Troponin = 21.99 pg/mL, pro Brain Natriuretic Peptide (Pro BNP) = 467 pg/mL, D-Dimer > 10000 ng/mL, blood glucose = 5.8 mmol/L, natremia = 136 mmol/L, kalemia = 3.6 mmol/L, urea = 2.49 mmol/L and creatinine at 27 µmol/L. The patient was placed on fluid restriction; methylprednisolone was stopped and replaced with dexamethasone at 0.6 mg/kg a day. She was prescribed Salbutamol aerosol 10 puffs*4/day with Azithromycin 20 mg/kg twice a day the first day then 20 mg/kg a day for 4 days, Amoxicillin-clavulanic acid at a dose of 150 mg/kg a day; Vitamin D at 2000 ui/day, Vitamin C 250 mg*2/day and low molecular weight heparin at a curative dose of 100 UI/kg/12 hours subcutaneously. A thoracic computed tomography scan first suggested SARS-CoV2 infectious lung disease affecting almost half of the lungs associated with atelectasis in the bilateral inferior bases (Figure 2). The cardiac ultrasound was normal. After 48 hours of hospitalization, on the seventh day of the evolution of the symptoms, the respiratory distress worsened. The respiratory rate was 80 cycles/min, and the child had an O2 Sat under HCM at 8 L/min at 88% and 78% at room air, which required non-invasive ventilation (NIV) with an Inspiratory Support at 12 cm H2O, Positive End Expiratory Pressure (PEEP) at +6 cm H2O, FiO2 = 100% with prescription of Atarax 25: 1/2 tab*2/day because of the patient's restlessness. On NIV, there was a decrease in the signs of struggle, but the child remained restless. The arterial gas checks revealed the following findings: pH = 7.39, pO2 = 47, pCO2 = 36, HCO3 = 22.4 and a SaO2 = 82%. Given these clinical, radiological, and gasometric findings under a PEEP at 6 and the fraction of inspired oxygen (FiO2) at 100%, the patient was diagnosed with ARDS. The PaO2/FiO2 was at 47 (< 300). After 24 hours of NIV, the patient was put on high flow oxygenation (HFO), with a 25 L/min flow rate, FiO2 100% alternating body positioning between prone and supine position. The patient improved progressively. She became calm, less polypnic with a decrease in the signs of struggle, but hypoxia persisted in the blood gas. The FiO2 was lowered from day 4 of HFO. After 8 days of HFO, and 11 days of hospitalization, oxygen therapy was stopped. The arterial blood gas showed: pH = 7.35, paO2 = 88, paCO2 = 30 Bicar = 19, SaO2 = 96%.
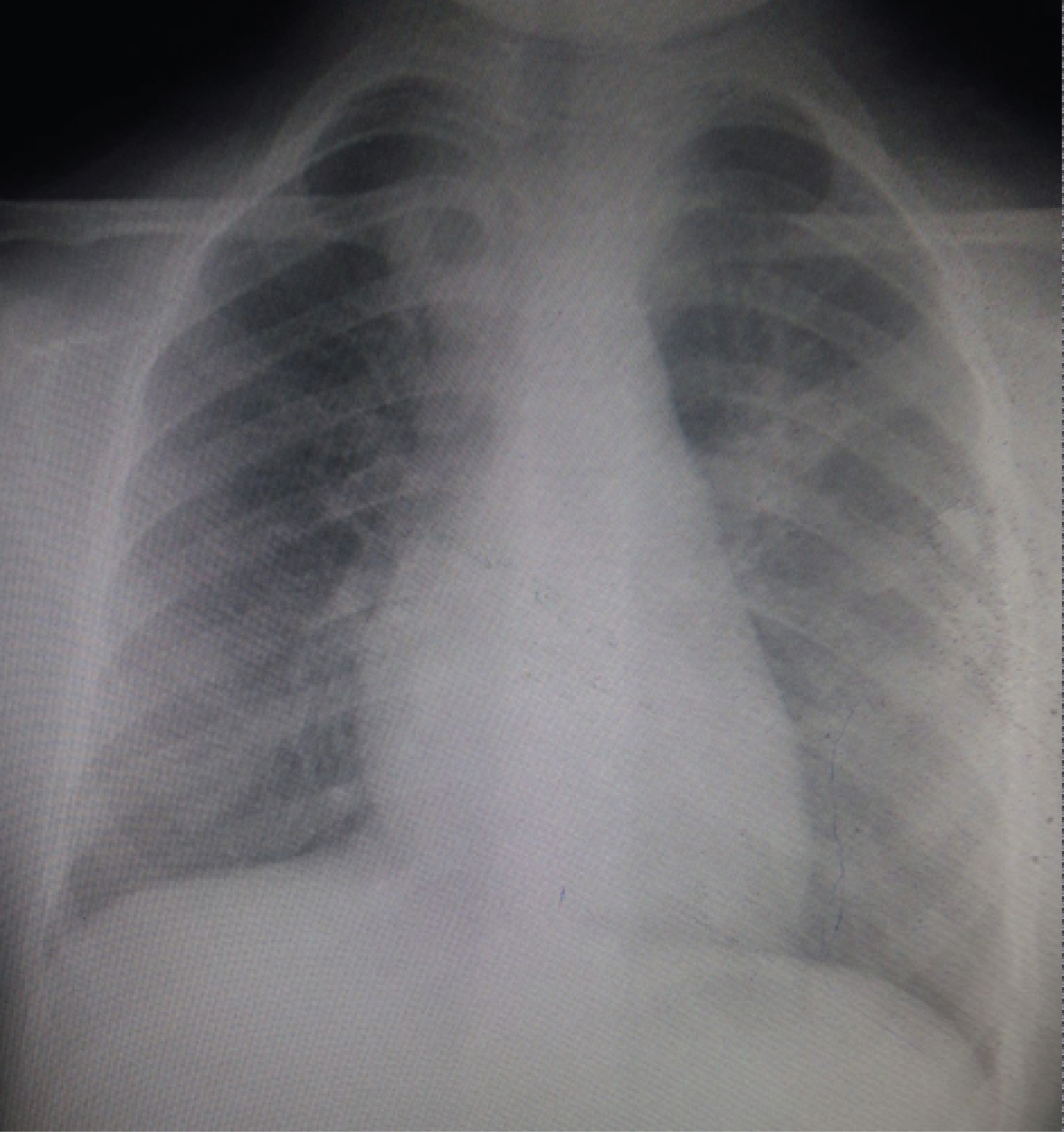 Figure 1: Frontal A chest radiography showing thoracic distension with bilateral alveolar opacities.
View Figure 1
Figure 1: Frontal A chest radiography showing thoracic distension with bilateral alveolar opacities.
View Figure 1
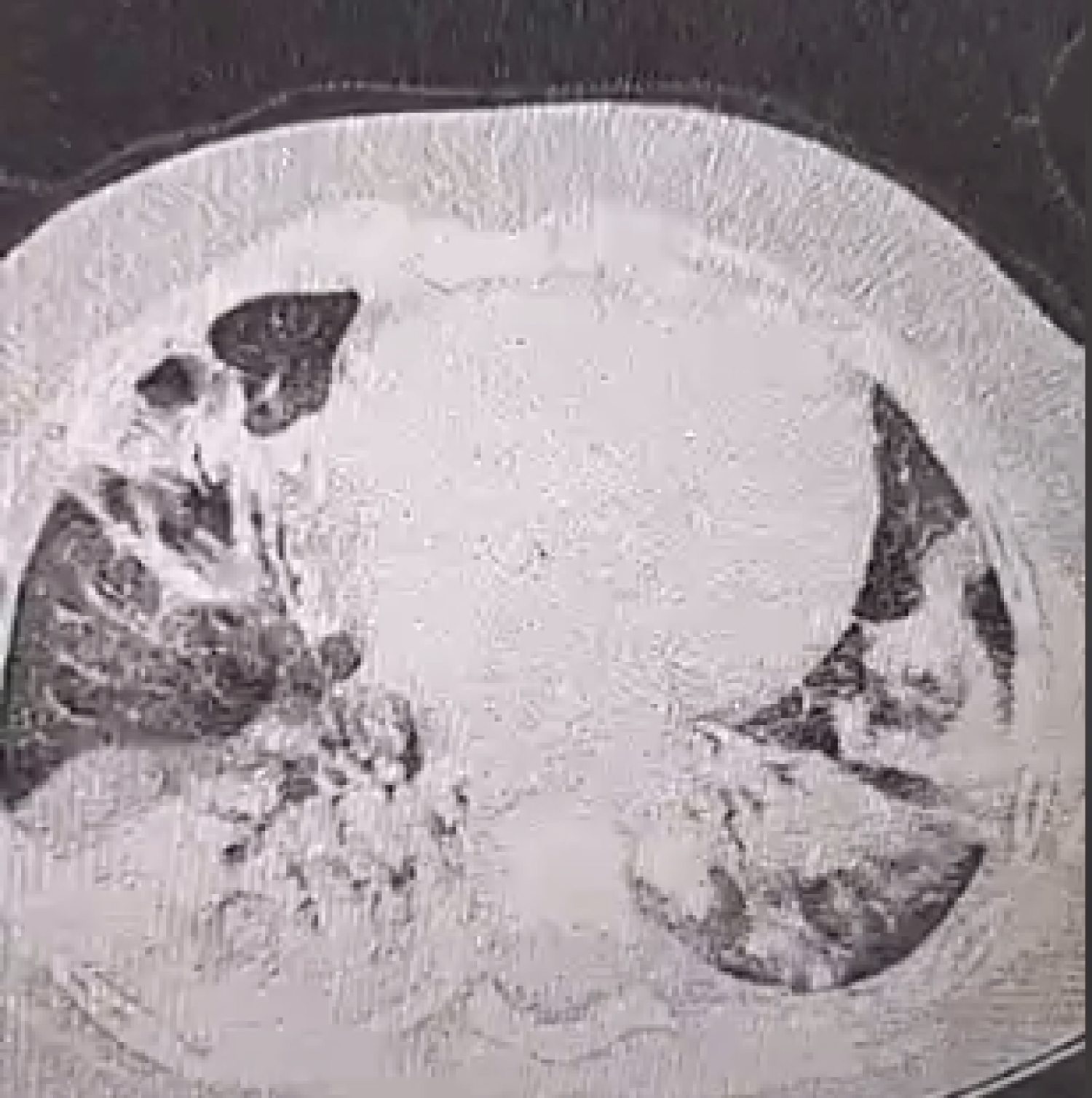 Figure 2: Thoracic computed tomography scan showing peripherally and bilaterally distributed ground-glass areas in the upper lingular and middle lobes associated with foci of alveolar condensation occupying almost the entire lower lobes as well as the middle and lingular lobes.
View Figure 2
Figure 2: Thoracic computed tomography scan showing peripherally and bilaterally distributed ground-glass areas in the upper lingular and middle lobes associated with foci of alveolar condensation occupying almost the entire lower lobes as well as the middle and lingular lobes.
View Figure 2
A follow-up thoracic computed tomography scan was normal with no pulmonary embolism. She was discharged 15 days after hospitalization with a background treatment for asthma. A functional respiratory exploration performed after her discharge confirmed the diagnosis of asthma. As for the epidemiological investigation, the RT-PCR SARS-CoV2 tests of the parents and the sister as well as the Covid serology results were negative. The serological tests did not detect Ig M and IgG antibodies against SARS-CoV2 in the patient's family members.
Previous publications related to COVID-19 in children have concluded that, compared to adults, children have a better overall prognosis, but this condition can be severe and may require complex management. The rate of admission to pediatric intensive care units for COVID-19 varies according to the studies and countries and the percentage rarely exceeds 10% [3].
To our knowledge, this is the first child hospitalized for SARS-CoV2 infection in a Tunisian pediatric intensive care unit.
The severity of SARS-CoV2 clinical manifestations depends essentially on the existence or not of comorbidities [4]. Our patient is obese and in adults, obesity represents an increased risk of severe COVID-19 infection with high mortality. The authors of a review and meta-analysis of the literature concluded that obesity in children increased the risk of developing a severe form by 2.87 [4]. This risk may result from a complex interaction of several mechanisms: obesity is characterized by ectopic fat deposits in the abdominal area, as well as the myocardium and thorax. These deposits have been involved as factors contributing to the release of inflammatory cytokines. On the other hand, lipid microdeposits at the level of the alveolar interstitial spaces aggravate the inflammatory infiltrate related to the viral infection, which could contribute to massive edema leading to ARDS [5]. The exploration performed at the time of our patient's discharge helped establish the diagnosis of asthma. In a systematic review aimed at finding out whether asthma is associated with a risk or higher severity of COVID-19 in children, the authors concluded that "there is insufficient evidence to indicate whether asthma is a risk factor for SARS-CoV2 infection or COVID-19 severity" [6]. There are also uncertainties about the dynamics of their contamination, transmission, and real contribution to the epidemic. Children are more likely to contract the virus from family members. On the other hand, the RT-PCR SARS-CoV2 and COVID-19 serology performed on our patient's family members proved that the origin of her contamination was out-of-home. Although, she had close contact with her parents and her sister and distancing measures were not applied, our patient did not transmit the virus to her family members. This question of contamination by children is raised, especially as the conclusions of the literature are sometimes contradictory. The symptoms of SARS-CoV2 are not specific and the identification of SARS-CoV2 infection in children is even more difficult during autumn and the flu season. About half of children infected with COVID-19 have fever or cough, and about one-third have both. Our patient was consulted 5 days after the onset of the symptoms. In the current epidemiological context, COVID- 19 should be suspected early by parents and primary care physicians. When on NIV, our patient met all ARDS criteria as established by the International Pediatric Consensus Conference, published in 2015 [7]. In adults, ARDS is the most frequent and most dreadful complication. Pediatric data related to children in severe to critical conditions are still limited. SARS-CoV2 pneumonia presents with some features that make it an atypical form of ARDS. The main feature is the dissociation between a relatively well-preserved pulmonary compliance and the severity of hypoxemia which is rarely observed in ARDS of other etiologies. Gattinoni, et al. classified SARS-CoV2-infected patients with ARDS into two categories. L profiles (Low elastance) present with high lung compliance and H profiles (High elastance) manifest impaired lung compliance [8]. However, patients with an L-profile can respond to increased FiO2, especially when administered through a high flow nasal system, without immediate resort to mechanical ventilation. In our patient, profound hypoxemia persisted while respiratory rate and signs of struggle improved markedly. This discordance is in favor of high thoracic compliance and an L profile. At the beginning of the pandemic, the infection was associated with many unknowns, particularly regarding the speed of the virus transmission. The first guidelines discouraged the use of HFO or any other non-invasive, potentially aerosol-generating approach. However, with more experience in the management of COVID-19, clinicians realized that mortality in patients on invasive ventilation was high and that HFO could avoid intubation when used carefully [9].
The use of HFO in case of SARS-CoV2 infection complicated by an ARDS is rare in children. In a multicentric study involving children hospitalized in 10 intensive care units in Chile, Colombia, Italy, Spain, and the United States, seven children with ARDS were on HFO, five did not require treatment intensification, and had a favorable outcome [10]. These findings are encouraging but larger-scale studies are needed. Patients treated with HFO should be closely monitored to detect the need for therapy intensification and mechanical ventilation. However, due to the persistent uncertainty, patients with COVID-19 should be cautiously treated. For our case, we adopted the strategy of the combination of HFO or e and prone positioning to save time and improve outcome. The outcome was favorable.
After more two years of collecting data and knowledge on corona virus, many questions remain indeed unanswered. There are still some unknowns when it comes to COVID-19, particularly in children. In this context, ARDS also seems to be atypical in children. HFO therapy may play a key role in improving the outcomes. Further data and guidelines are needed. In the meantime, we hope that this case will help manage other similar patients with the same conditions.
The authors declare no competing interest.
"All data underlying the results are available as part of the article and no additional source data are required."
Study conception and design: Samia Tilouche, Sameh Ghorbel, Emna Sfar
Data collection: Samia Tilouche, Nejla Soyah, Najoua Kahloul
Data interpretation: Samia Tilouche, Naila Hannachi, Jihene Bouguila
Drafting of the article: Samia Tilouche, Emna Sfar
Critical revision of the article: Lamia Boughamoura