Approximately 30 million annual clinic visits are attributed to cough in the United States. Moreover, evaluation and management of persistent cough in pulmonary clinics account for roughly 40% of patient volume. The most common etiologies are: Upper airway cough syndrome (UACS), asthma, non-asthmatic eosinophilic bronchitis (NAEB) and gastro-esophageal reflux disease (GERD) - all of which are treatable. However, despite avoidance of triggers and medical therapy, there remains an elusive diagnosis for some individuals with persistent cough. Further investigation warrants bronchoscopy, which is indicated for patients with persistent or unexplained cough.
The purpose of this study is to assess the diagnostic yield of fiberoptic bronchoscopy (FB) with Broncho-alveolar lavage (BAL) for chronic cough in patients with normal chest roentgenogram. FB records were reviewed in cohort for a period of 3 years. Only patients with normal chest roentgenograms who remained refractory to medical therapy were included in the study. Fifty-two (52) cases encompassing ages 20-90 were reviewed. In 42 cases, BAL was negative for any diagnostic cause. Eight (8) cases were significant for infectious processes, one (1) case diagnosed bronchiectasis, and 1 case was lost to follow-up. Statistical analysis between the total cases in each group was statistically significant p < 0.001. Thus, though FB with BAL is indicated in chronic cough of unknown etiology, its diagnostic yield is low.
Chronic cough, Upper airway cough syndrome (UACS), Asthma, Gastroesophageal reflux (GERD), Non-asthmatic eosinophilic bronchitis (NAEB), Fiberoptic bronchoscopy (FB)
Every human has a natural defense mechanism that removes mucus, noxious substances and infections from the larynx, trachea, and large bronchi. The innate cough mechanism is a symptom experienced by healthy, non-smoking individuals, as well as immunocompromised hosts. However chronic cough, in the absence of inciting drugs such as ACE inhibitors, can be a clinical pointer to "silent" diseases [1,2]. Our study referred to the conventional definition of chronic cough, which is defined as "refractory cough to therapy for > 8 weeks in hosts with stable or normal chest roentgenogram" [1]. The most common etiologies, excluding confounders such as cigarette smoking and ACE inhibitors, are upper airway cough syndrome (UACS - formerly known as postnasal drip syndrome), asthma, non-asthmatic eosinophilic bronchitis (NAEB) and gastroesophageal reflux disease (GERD) [3].
UACS, which accounts for 41%-58% of chronic cough cases, can be initially treated with antihistamines and decongestants. Antibiotics that cover Streptococcus pneumoniae and Haemophilus influenzae for 10 days may be added if infective sinusitis is suspected. Cough variant asthma, which accounts for 24%-59% cases of chronic cough, can be initially treated with inhaled bronchodilators, inhaled corticosteroid (ICS) and, in specific cases, leukotriene receptor antagagonists. GERD accounts for 21%-41% of chronic cough patients and can be initially treated with diet, exercise and proton pump inhibitors (PPI). NAEB, which is commonly under diagnosed due to lack of resources, accounts for up to 33% and can be initially treated with an ICS, similar to asthma [4].
Epidemiologic surveys report persistent cough present in 11% to 18% of the general population. In fact, patients with persistent cough constitute up to 40% of chest specialist outpatient practice [1]. In 2006, the American College of Chest Physicians published evidence-based guidelines for the diagnosis and management of chronic cough. Bronchoscopy was cited as a means of further investigation for patients > 15-years-old with inadequate response to optimal medical therapy after a 4 - 6 week follow up [1]. Thus, this study seeks to explore the diagnostic yield of FB with BAL in patients with normal chest roentgenograms.
Flexible fiberoptic bronchoscopy allows for visualization of the lumen and mucosa of the trachea, proximal and segmental airways. It has therapeutic and diagnostic purposes in specific circumstances. Various studies have shown its superlative efficacy in a wide variety of hosts. In one study, 38 patients were suspected of having tuberculosis (TB) of which 28 (73.68%) were proven to have TB following FB. In the same study 46 patients were suspected of having a lung mass, and 31 (67.39%) cases were proven following FB [5]. In another study, bronchoscopy yielded a diagnosis of 40.5% for infection, 67% for TB, 61.2% for malignancy and 43% for interstitial lung disease [5].
Albeit the question remains, does FB yield the same diagnostic results in chronic cough? Evidently, the purpose of this research is to determine if FB yields similar diagnostic results in chronic cough.
Retrospective cases of outpatient bronchoscopy records between January 2013 and September 2016 at St. Joseph's Regional Medical Center were gathered. Patients with normal chest x-rays with chronic cough without a diagnosis were included.
A total of 52 patients with a mean age of 60 ± 16 years were collected, including 27 females and 25 males. The causes of chronic cough were as follows: 42 cases (80.77%) yielded negative lavage, 8 (15.38%) yielded infectious etiologies, 1 (1.92%) showed abnormal lung pathology, specifically bronchiectasis, and 1 (1.92%) specimen was lost to follow-up. Infectious causes included 1 (12.5%) of Haemophilus influenzae, 3 (37.5%) of Pseudomonas, 3 (37.5%) of Staphylococcus aureus and 1 (12.5%) of Aspergillus. We performed statistical analysis between the total number of cases in each group and found low diagnostic yield in lieu of a normal chest x-ray with a statistical significance of Chi Square 11.56, p < 0.001 (Figure 1).
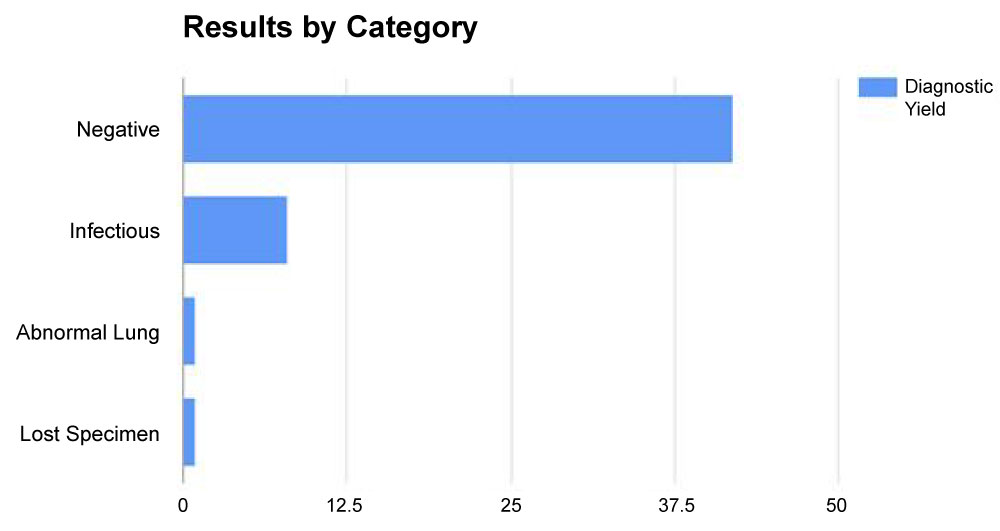 Figure 1: The diagnostic yield of FB with Bal by category. View Figure 1
Figure 1: The diagnostic yield of FB with Bal by category. View Figure 1
A cough is a complex arc involving stimulation of cough receptors that exist not only in the respiratory epithelium, but also the pericardium, esophagus, diaphragm, and stomach. These receptors are sensitive to a variety of mechanical and chemical stimuli which activate the vagus nerve, then eventually the phrenic nerve and spinal motor nerves [1]. A cough can be initiated by a variety of mechanisms affecting any region of this path. To diagnose the cause of a chronic cough is thus dependent on many mechanisms and in some cases requires multiple studies beyond radiographs and sputum analysis. Examples include Barium swallow, 24-hour esophageal pH monitoring, direct laryngoscopy evaluation and multichannel intraluminal impedance (MII) to exclude and assess GERD [1].
A large body of research also embodies diagnosis and characterization of asthma. Noninvasive biomarkers such as exhaled nitric oxide (FENO) and sputum or blood eosinophilia assist in asthma diagnosis and guidance of management. Most recently, evaluation by periostin levels as a biomarker has also offered further insight in understanding reactive airways and even bronchiectasis [6].
Over the past decades, FB has been utilized as a tool for diagnostic and therapeutic interventions in patients with pulmonary pathologies associated with chronic cough. In addition, it has been regarded as a safe intervention with complications of less than 0.1% to 11% in several studies. Moreover, several studies have reproduced data that reveal a mortality rate of 0% to 0.1% [7]. Table 1 illustrates the major and minor complications associated with FB in 3 studies.
Table 1: Complications and Outcomes associated with FB. View Table 1
Based on the data from Table 1, it can be deduced that FB is relatively a safe procedure. With careful selection of patients, proper management of sedation, and usage of FB by skilled intensivists or pulmonologists, complications can be as low as 0.02%. Such results may have led to widespread usage of bronchoscopy. Therefore, this paper seeks to ask a provocative question - is it possible that the availability and relative low risk have led to excessive usage of FB? With any diagnostic test, clinicians are faced to answer the following questions: Will the test lead to a change in management? Will the test improve patient outcome? How cost effective is the test? But more importantly, clinicians must ascertain the accuracy of the test in ruling in or out the disease in question. In other words, what is the diagnostic yield of the test as proven by dependable research?
In our study of a sample of 52 patients with normal roentgenogram, the diagnostic power for FB was surprisingly low. FB was statistically significantly found to be non-diagnostic in 42 (80.77%) patients.
Sen, et al. also recognized that FB has a low diagnostic yield in patients with chronic cough [8]. A retrospective study was conducted in patients with unexplained cough that was refractory to medical therapy. Patients with hemoptysis, acquired immunodeficiency syndrome (AIDS) or with roentgenograms suggesting the primary diagnosis were excluded. In this study of 25 patients with chronic cough for 2 - 240 months, FB was diagnostic in only 7 (28%) cases. This leaves an impressive 72% (18) to be non-diagnostic.
As was eluded to earlier, FB is more appropriate in patients suspected of having malignancy or Tuberculosis Infection. Alzeer, et al. demonstrated this in retrospective review over 3 years where diagnostic bronchoscopies were conducted in 592 out of 720 cases [5]. Tuberculosis and Malignancy were the two main indications, yielding diagnosis in 67% of suspected Tuberculosis cases and 61.2% of malignancy cases, respectively. It is to be noted this study did not exclude cases with abnormal chest roentgenograms, as was highlighted in our study.
We strongly believe that for patients with chronic cough and normal roentgenogram, the usage of FB will be significantly non-diagnostic and clinicians should entertain the possibility of other noninvasive/minimal invasive testing.
The diagnostic yield of FB with BAL in patients with chronic cough and normal chest x-ray was significantly low. To mitigate this problem it is recommended that FB be performed in a selective patient population. Several studies have reproduced high diagnostic yield of FB with BAL in a patient population with a high prevalence of malignancy and infection such as TB. Though FB is indicated to further evaluate the cause of chronic cough in patients with normal roentgenograms, our experience showed that the yield was surprisingly low. Our results were statistically significant and lead us to question whether FB is actually indicated, given such poor diagnostic yield. Therefore in a patient population of chronic cough with normal roentgenogram, we recommend that clinicians explore other noninvasive or minimally invasive tests while considering their accuracy and cost. In recent research, there has been a great deal of development involving noninvasive biomarkers that further expand our diagnostic means. As many tools are still being evaluated for their efficacy, we recommend the continued exploration of new methods for utilization in chronic cough.
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript.