Vascular ring, which is a rare cause of respiratory distress in infants, results in respiratory and gastrointestinal findings due to tracheal and/or esophageal compression, but the diagnosis may be delayed because of the nonspecific symptoms. Double aortic arch is the most common vascular ring anomaly. A case of double aortic arch presented with respiratory distress, stridor, and feeding intolerance during infancy is discussed.
Respiratory distress, Vascular ring, Infant
Vascular ring is seen with an incidence of 1% in all congenital cardiovascular anomalies. Double aortic arch is the most common anomaly among vascular ring pathologies (40%) [1]. Abnormal regression of the brachial arch during embryogenesis results in persistence of two aortic arches, forming a vascular ring and compressing the trachea and/or esophagus. Diagnosis may be difficult because of the variations in the clinical spectrum [2].
A 4-month-old full term male infant was transferred from another medical center for the management of respiratory distress. According to the patient's medical records, the patient initially was admitted with the complaints of difficulty in breathing, wheezing and cough with the diagnosis of acute bronchiolitis. The patient was started on prednisolone and inhaler therapy. Since respiratory distress was persistent and his complaints worsened with feeding, antibiotic and anti-reflux therapy were added to the treatment with the pre-diagnosis of aspiration pneumonia. The patient was transferred to our hospital for further evaluation and treatment after 7 days of intensive inhaler therapy, antibiotic and anti-reflux treatments. In his past medical history: the baby was noted to have noisy breathing at 2nd-3rd weeks of his life. He was evaluated by ENT because of inspiratory stridor at 2 months of age and the laryngoscopic evaluation was reported as normal. Mom reports that noisy breathing improved slightly, but it did not change with position, alertness or feeding status. At presentation the patient was in moderate distress with suprasternal, subcostal and intercostal retractions. His respiratory rate was 50 breaths/min; SpO2 was 95% at room air. The cardiovascular findings were unremarkable. The chest X-ray revealed hyperinflated lung fields bilaterally. Respiratory sounds were coarse and inspiratory stridor and bilateral diffuse rhonchi were appreciated. The cardiovascular findings were unremarkable. Chest X-ray showed increased bronchovascular markings. Echocardiography was performed by the pediatric cardiologist and reported as normal. Then, contrast enhanced computed tomography revealed the double archus aorta with hypoplastic right arch compressing the trachea (Figure 1). The child was scheduled for surgery to correct the vascular ring.
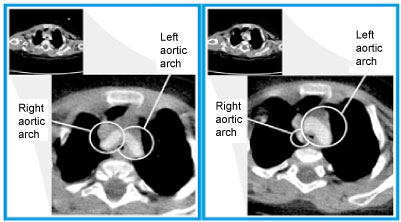 Figure 1: Contrast-enhanced computerized tomography axial section image showing the double aortic arch.
View Figure 1
Figure 1: Contrast-enhanced computerized tomography axial section image showing the double aortic arch.
View Figure 1
Since aortic arch anomalies are very rare, they are reported as case reports in general and epidemiological data are quite limited [3].
In the embryonic period, the ventral and dorsal aortas were connected by six primitive aortic arches. Each time an arch develops, the previous arc is regressed. The arches 1, 2 and 5 are regressed respectively and form a double aortic arch. In normal development, the right 4th arch is regressed and the left 4th arch forms the left aortic arch. If the double aortic arch remains at this stage, it may compress the trachea and esophagus at different degrees by surrounding these structures and forming a vascular ring. Double aortic arch is of 3 types; right dominant arch (75%), left dominant aortic arch (20%) and balanced aortic arch (5%) [4]. in our case, the left dominant aortic arch was detected.
If the vascular ring is tight, the compression is severe and may cause symptoms from birth. However, some patients with partial compression may be asymptomatic during their lifetime. There is a case diagnosed at 79-years of age in the literature [5]. Surgical treatment is the only option in symptomatic cases.
Although vascular ring is a rare cause of extrinsic tracheal compression, it was the most frequent cause of the airway compression due to the cardiovascular disease in children [6]. Clinical symptoms are usually seen in the first 6 months in double aortic arch anomaly. Respiratory symptoms are seen in 91% of patients and gastrointestinal symptoms are present in 40% of them. Respiratory symptoms are stridor, dyspnea, recurrent respiratory tract infections, apnea, cyanosis, while gastrointestinal symptoms are dysphagia, weight loss and developmental delay [4]. In our case, the clinical symptoms started in the newborn period of life and the diagnosis was made in the 4th month of life.
Double aortic arch is an isolated cardiovascular anomaly and may rarely be associated with other cardiac anomalies such as tetralogy of Fallot, truncus arteriosis, and transposition of the great arteries, VSD and aortic coarctation [7]. In our case, no additional cardiac anomaly was detected.
Chest X-ray, esophagogram with barium, CT angiography and MRI are helpful in the diagnosis. The order of diagnostic methods may vary according to the experience and preference of that center [8]. Chest X-ray should be taken in both postero-anterior and lateral directions. In the lateral view, forwardly inclined trachea should suggest the diagnosis of vascular ring. While the most commonly used method in the diagnosis of vascular ring is esophagogram with barium, nowadays, angiography is taking its place. Echocardiography is performed for the determination of additional intracardiac anomalies and vascular anatomy. Although vascular rings are usually isolated anomalies, they may rarely be associated with tetralogy of Fallot, truncus arteriosus and aortic coarctation [1,9]. Both MRI and CT angiography can reveal the positions of vascular, tracheobronchial, and esophageal structures and their relations to one another. These imaging modalities are performed in many centers to confirm the diagnosis, detect additional cardiac anomalies and prepare the patient for surgery [10].
All of these studies have drawbacks. CT angiography expose the patient to radiation and require intravenous contrast. MRI requires sedation of the patients. The expense associated with these investigations must also be considered. In our case, we followed the order of chest radiography, echocardiography and CT angiography in diagnosis. According to the experience of the center, bronchoscopy can be performed to see the pulsatile compression on the trachea, but the patient's symptoms may worsen as it is invasive and may increase tracheal edema.
In conclusion, double aortic arch is a rare cause of respiratory distress during infancy and should be considered in the differential diagnosis in patients presenting with symptoms of stridor, and feeding intolerance.