A 38-year-old with ankylosing spondylitis presented to a sports medicine clinic following a traumatic cycling accident. Physical exam found pain, swelling and ecchymosis overlying the proximal thigh. Point of care ultrasound revealed an underlying large hematoma causing a closed degloving of the overlying tissue or a Morel-Lavallée lesions. MRI confirmed size of the lesion and diagnosis made previously. The patient was treated conservatively without any invasive procedures, infection and with excellent pain control. He returned to cycling successfully and has had no adverse side effects. This case demonstrates the use ultrasound in the early detection of this type of injury as well as the use of noninvasive techniques not previously demonstrated on a lesion of the size presented.
Morel-Lavallée lesions, Non-invasive management, RICE method, Hematoma
Morel-Lavallée lesions (MLL) are subcutaneous fluid collections that are the result of shearing forces or crush injury. They occur from separation of interfacial planes between subcutaneous soft tissue and the skin [1,2]. This separation causes disruption of the capillaries and lymphatics producing an accumulation of fluid consisting of blood, lymph, necrotic debris and liquified fat [1,3,4]. The most common location is over the greater trochanter, but can occur anywhere on the trunk or extremities [1,2,5]. These lesions typically present with pain and swelling at the location of injury, but can be difficult to differentiate from other soft tissue masses due to the possibility of presentation hours to years after the trauma occurs [1,2,6].
MRI is currently the gold-standard for diagnosis of MLL with the Mellado-Bencardino classification distinguishing six different types based on imaging findings [1,4,7]. Ultrasound provides another modality of assessment and diagnosis of MLL with characteristic findings that can be supported by clinical context [3]. Invasive treatments of large lesions are preferred with either percutaneous drainage or surgical incision and drainage. In chronic MLL, a fibrous capsule can form around the fluid collection making surgical resection a necessity [5,6,8]. We present a case of a large MLL that was identified early based on ultrasound findings and treated noninvasively.
38-year-old amateur cyclist with ankylosing spondylitis (AS) was riding at high speed with a group of cyclists when he lost control of his bicycle hitting the brakes and flipping over the handlebars. He hit asphalt first, then rolled into the grass on the shoulder of the road. The patient was driven to the nearest emergency room where he was treated initially for his injuries. Along with the diagnosis of concussion he sustained injuries to his left hip, right knee, and left elbow with multiple abrasions, contusions, and chipped incisors.
On day 5 post injury the patient was noted to have an antalgic gait walking into the sports medicine clinic. Exposure of the left hip revealed reddish-purple, non-blanching discoloration of the skin with a large amount of swelling over his lateral left thigh extending anteriorly towards the groin (Image 1). The patient was tender to palpation over the noted lesion, had full active range of motion with pain elicited with movement. Patient's vitals were within normal limits. Ultrasound examination of the lesion revealed a hypoechoic lesion significant for a large fluid collection beneath the subcutaneous tissue layer (Image 2). There was no visible evidence of encapsulation, loculation, or air fluid levels. Doppler did not exhibit free flowing of fluid. Underlying muscle was undisrupted. There was no obvious disruption to the underlying cortical layer of the femur. An MRI was ordered which confirmed a large fluid collection of the interfacial planes of the left hip measuring 15 cm × 17 cm × 2 cm which could contain up to 510 ml of fluid. Diagnosis of Morel-Lavallée lesion was made.
 Figure 1: Left Thigh, initial presentation.
View Figure 1
Figure 1: Left Thigh, initial presentation.
View Figure 1
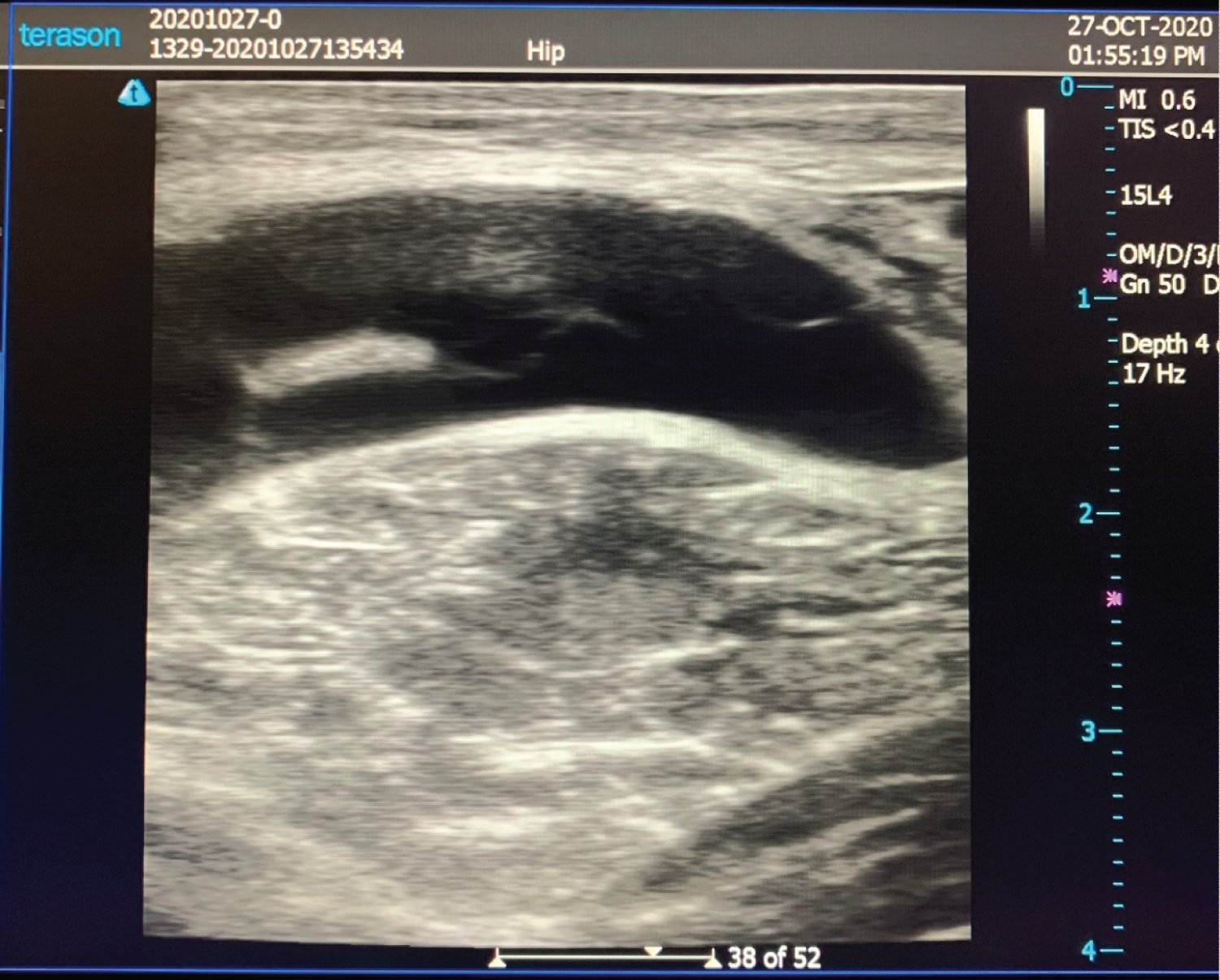 Figure 2: Ultrasound Image, Initial exam.
View Figure 2
Figure 2: Ultrasound Image, Initial exam.
View Figure 2
Decision was made to treat the patient non-invasively due to the immunocompromised status caused by his current medications for AS. Treatment consisted of continuous compression with a hip spica wrap along with cold compression, 4-6 times per day for 30 minutes. He followed routinely for recovery progression and measurement of lesion (Image 3). Physical therapy focused on core strengthening, early mobilization, manual therapy with ROM preservation, and low-impact stationary bike while minimizing shearing forces. The patient was able to maintain full functional activity during treatment without complications. After 6 weeks of treatment, the patient showed overall clinical improvement (Image 4). His greater trochanteric circumference measurements had decreased from 101 cm to 97 cm. He returned to cycling on an indoor trainer utilizing a power meter to titrate wattage output as tolerated and advanced to outdoor cycling once back to baseline power output without significant symptoms (Image 5).
 Figure 3: Follow up measurement of Left thigh.
View Figure 3
Figure 3: Follow up measurement of Left thigh.
View Figure 3
 Figure 4: Recovery left thigh injury.
View Figure 4
Figure 4: Recovery left thigh injury.
View Figure 4
 Figure 5: Return to activity post recovery.
View Figure 5
Figure 5: Return to activity post recovery.
View Figure 5
Treatment of MLL currently consists of noninvasive management with compression or invasive managements of percutaneous aspiration, sclerotherapy, or surgical interventions. Noninvasive management of acute MLL is an effective approach when intervention occurs prior to the development of a fibrous capsule or with smaller lesions [3,5,6,9]. Noninvasive management involves placing a compression banding over the affected area with rest, elevation and periodic use of ice with a healing time of 2-11 weeks. Noninvasive management without compression banding resulted in a high incidence of cases requiring subsequent surgery [3]. Once a fibrous capsule has developed around the lesion, surgical intervention is the only recommended treatment for resolution of the lesion [3,5,6]. Some have recommended invasive management of all large lesions [2]. Large lesions defined as those containing greater than 50 ml can be more frequently found in the pelvis, flank and thigh. Previously, large lesions which were not treated surgically were more likely to have a recollection or encapsulation of the lesion [2,4].
Ultrasound provides an accessible modality for early evaluation of MLL allowing for earlier intervention with noninvasive management [3]. This earlier identification and management can precede development of a fibrous capsule to mitigate necessity for surgical intervention and the complications it can entail. On ultrasound, MLL appears as nonspecific fluid collections with heterogeneous or homogeneous echogenicity depending on the chronicity of the lesion [6]. Acute lesions are typically heterogeneous in appearance with irregular margins and lobular shape. Chronic lesions are typically homogenous with smooth margins and a flat or fusiform shape [3,6]. Echogenicity of the fluid collections has no relationship with the age of the lesions [3,10].
This case supports the effectiveness of noninvasive management as an initial treatment in the setting of acute MLL. Ultrasound provides a quick, easily accessible modality to identify these lesions following a traumatic event involving shearing forces. Given early identification and intervention, favorable outcomes can be achieved with noninvasive management without necessitating procedural intervention and the risks it involves. More research is necessary on the effectiveness of using ultrasound for early identification of MLL and subsequent intervention with noninvasive management given the appropriate ultrasound findings for an acute lesion.