Objective: This study aimed to analyze the effects of detraining after previous resistance training (RT) performed with different exercise orders (EO) on muscular strength, flexibility and functional capacity in older women.
Methods: Twenty-three older women (61.6 ± 6.7 years; 74.2 ± 12.6 kg; 156.2 ± 5.9 cm) were randomized to a group that performed the exercises from multi- to single-joint order (MJ-SJ, n = 10) or a group that performed the exercises from single- to multi-joint order (SJ-MJ, n = 13). Both performed the same RT program (7 exercises, 3 sets of 10-15 maximum repetitions, twice a week, 16 weeks). Following the RT program, participants detrained for 16 weeks. Muscular strength (handgrip strength test), flexibility (sit-and-reach test), and functional capacity assessments (30-s arm curl, 30-s stand chair, 10m walking, getting up and moving) were carried out pre-training, post-training and post-detraining.
Results: Results indicated that the effects of detraining do not depend on the manipulation of EO. Maintenance of benefits obtained from the RT program was observed only for flexibility, where both groups had higher scores compared to pre-training (MJ-SJ = 11%; SJ-MJ = 24.4%).
Conclusion: We conclude that detraining in older women can compromise previous gains made in muscular strength and functional capacity.
Training interruption, Strength training, Range of motion
Detraining is defined as a partial or complete loss of adaptations induced by a physical exercise program as a result of training interruption [1]. This may be a common occurrence among older adults, regardless of the reason (e.g., vacation, travel, surgery, hospitalization) [2] and results in the gradual decrease in gains achieved from an exercise program [3]. The process might be more pronounced in older adults [4] since it may operate in conjunction with declines in physical and functional capacities as a result of the natural aging process.
Prescription of RT programs involves control of several variables that can directly influence the benefits resulting from the practice of this type of exercise. The literature indicates that the manipulation of variables, such as weekly frequency [5,6] and volume [7] do not provide a greater retention of gains obtained as a result of the practice of RT in older people subsequently undergoing detraining. On the other hand, after detraining the older individual who performed resistance exercises at high intensity showed greater retention of gains compared to those who exercised at low intensity [8,9] indicating that the intensity of the RT program may play an important role after a detraining period.
Exercise order (EO), characterized as the sequencing of the exercises that compose a RT protocol [10,11] is a variable of training structure that influences the volume and intensity of the session [12]. Regarding intensity, investigations involving different EO with older adults indicate that muscular strength gains are greater for exercises performed at the beginning of the session [13] which can be attributed to the ability to use higher external loads [12]. To date, the effects of detraining after RT programs performed with different EO are lacking, including important health and quality of life indicators for older adults, such as handgrip muscular strength, flexibility and functional capacity.
Given that a hiatus in exercise training may occur in older adults, it would be beneficial to determine if one particular EO would provide more sustained benefits in fitness than another EO. Therefore, the purpose of the present study was to analyze the effects of detraining after previous RT with different EO on muscular strength, flexibility and functional capacity in older women. We hypothesized that the magnitude of retention of the benefits obtained as a result of performance of RT would be greater in participants exposed to multi-joint exercises at the beginning of the session compared to those performed at the end of the session.
The present study was carried out over a total of 35 weeks. In weeks 1, 18, and 35 anthropometric, muscular strength, flexibility and functional capacity tests were performed. The RT program was conducted between weeks 2 and 17, and detraining between weeks 19 and 34. Participants were instructed not to perform any other type of physical exercise during the entire study period, especially during detraining, where they were instructed to resume their respective routines, abstaining from performing physical exercises.
Participant recruitment was carried out through newspaper and radio advertisements and home delivery of flyer in the central city area and residential neighborhoods. Initially, 41 women were interested in participating in the study and were admitted as long as they met the following inclusion criteria: (1) 60 years or older; (2) Female; (3) Physically independent; (4) Not being involved in physical exercise more than once a week for the last six months prior to the beginning of the study. After initial screening, 32 participants were randomly assigned (ramdom.org) to one of two groups: One group that performed their exercises from multi-to single-joint order (MJ-SJ, n = 16), while the other group performed their exercises in a single-to multi-joint order (SJ-MJ, n = 16). Both groups were submitted to the RT program twice a week for 16 weeks. During the RT program, nine participants dropped out the study (MJ-SJ, n = 6; SJ-MJ, n = 3), due to personal reasons or loss of interest. Thus, 23 participants (MJ-SJ, n = 10; SJ-MJ, n = 13) completed the RT phase. After 16 weeks of detraining, the remaining 23 participants were submitted to the same pre and post-training evaluations.
Written informed consent was obtained from all participants after being provided with a detailed description of study procedures, benefits, and possible risks. This study was conducted in accordance with the Helsinki Declaration and approved by the local University Ethics Committee (Process 2.754.821). Figure 1 presents the schematic design of participant recruitment and allocation, based on the CONSORT 2010 Flow Diagram [14].
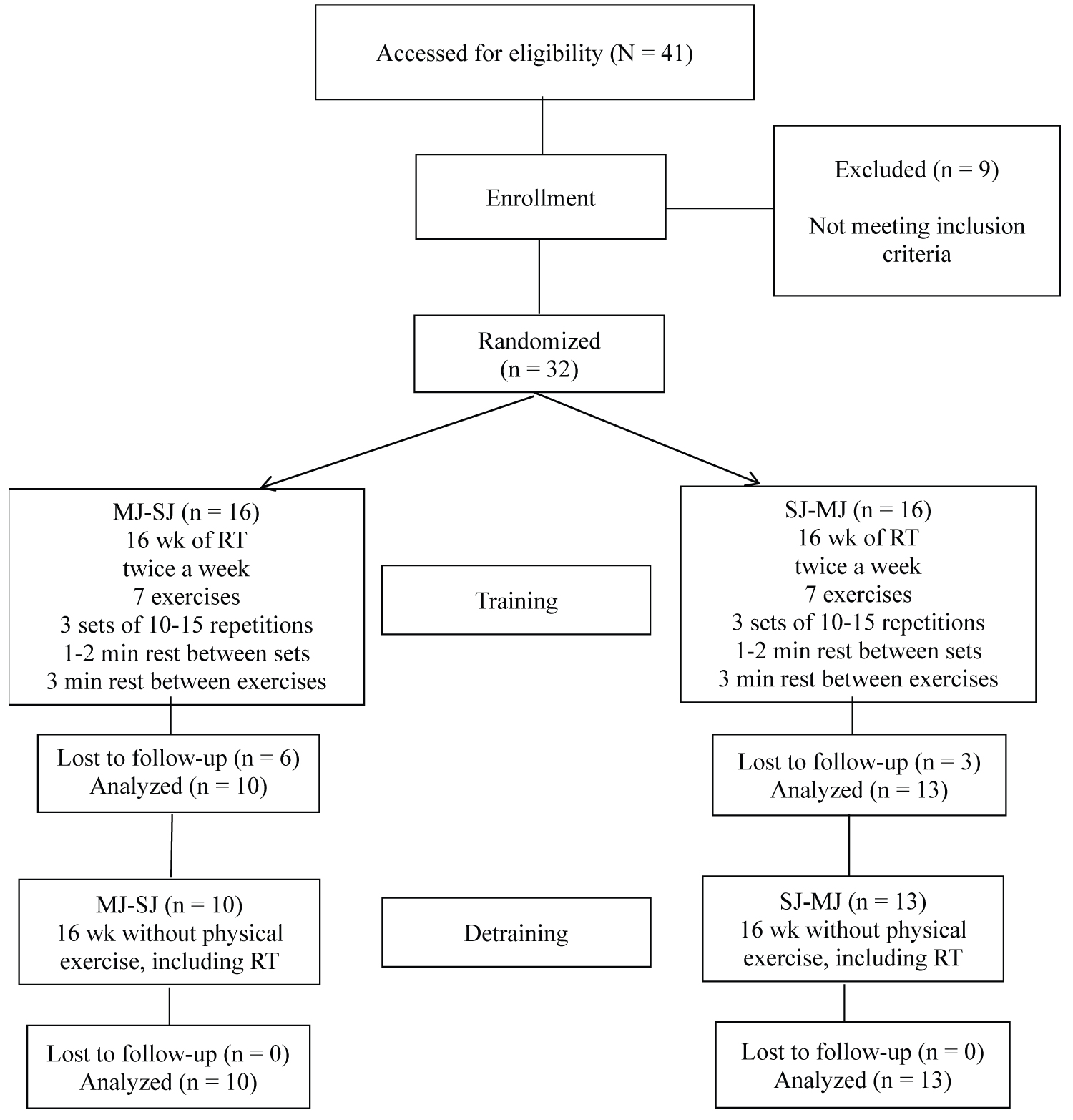 Figure 1: Schematic representation of participant recruitment and allocation.
Figure 1: Schematic representation of participant recruitment and allocation.
Note: RT: Resistance Training; MJ-SJ = Group that performed the exercises from multi- to single-joint order; SJ-MJ = Group that performed the exercises from single-to multi-joint order.
View Figure 1
Body mass was measured to the nearest 0.1 kg using a calibrated electronic scale (Omron, Model HBF-214, Illinois, USA), and height was measured to the nearest 0.1 cm with a wall stadiometer (E120A - Tonelli, São Paulo, Brazil), according to procedures described in the literature [15]. For both measures, participants wore light workout clothing and no shoes. Body Mass Index (BMI) was calculated as body mass (kg) divided by height (m 2 ).
Muscular strength was assessed using the handgrip strength test performed with an isometric dynamo-meter (Smedley T.K.K 5401 GRIP-D, Takei, Tokyo, Japan). In a standing position, participants held the dynamometer in the dominant with the arm extended alongside the body. Upon a signal from the examiner, participants performed a maximum contraction. During the test, there was encouragement by standardized verbal commands. Participants were measured three times, and the best performance attempt was utilized. The rest interval between attempts was one minute.
Flexibility was evaluated by the sit-and-reach test, performed according to standard procedures [16]. A standard box was placed on the floor with a measuring tape attached to the top at the 38 cm mark. Participants sat on the floor with shoes on and fully extended the legs with the soles of the feet flat against the end of the box. The participant extended the arms forward, placing one hand on top of the other. With palms down, the participant reached forward sling hands along the measuring scale as far as possible without bending the knees. Three trials were performed, with an interval of one minute between trials, and the highest score was considered test´s final result [17].
Functional capacity was assessed in a single day by a team of examiners, with each examiner responsible for the same test at the different moments to ensure measurement quality. A battery with four tests was employed to measure upper-body muscular endurance (30-s arm curl test), lower-body muscular endurance (30-s chair stand test) [18], gait speed (10m walking test) [19], and agility and dynamic balance (getting up and moving test) [20].
A supervised whole-body RT program was performed in the morning during 16 weeks in the University facilities. The protocol was based on recommendations for RT in an older population to improve muscle endurance and muscle strength [21]. Exercise professionals with substantial RT experience personally supervised all participants to help ensure consistent and safe performance. Participants performed RT using a combination of free weights (preacher curl) and machines. The MJ-SJ group performed the exercises in the following order: Chest press, seated row, triceps push down, preacher curl with barbell, horizontal leg press, knee extension, and seated calf raise, while the SJ-MJ group performed the same exercises, however, in the respective order: preacher curl with barbell, triceps push down, seated row, chest press, seated calf raise, knee extension and horizontal leg press. The RT program was performed twice a week, totaling 32 training sessions. For all exercises, 3 sets of 10-15 repetitions maximum were performed. Participants were instructed to inhale during the eccentric phase and exhale during the concentric phase while maintaining a constant velocity of movement at a ratio of 1:2 for the concentric and eccentric phases, respectively. The load used for each exercise was adjusted according to the participant’s ability and degree of improvement in exercise capacity throughout the study to ensure that participants exercised with as much resistance as possible while maintaining proper exercise execution technique. Progression in each exercise was made when 15 repetitions were completed for two consecutive sessions, with weight increased by 2-5% for upper limb exercises and 5-10% for lower limb exercises. Rest intervals between sets and exercises were 1-2 min and 3 min, respectively [11].
Instructors personally supervised all participants during the entire intervention and registered the load (kg) applied to each exercise every training session. Total training load was calculated as the sum of the highest load lifted for each exercise from the two training sessions performed week by week.
All participants were instructed not to perform any physical exercise, including RT, for 16 weeks after the post-training measurements, and were encouraged to maintain their regular daily living activities throughout this period and not to change their diet.
Normality was checked by the Shapiro-Wilk test. Data were expressed as means and standard deviations. Pre-training differences between groups were explored with independent t- test. Levene´s test was used to analyze homogeneity of variances. Two-way analysis of variance (ANOVA) for repeated measures was used for within- and between-group comparisons. Bonferroni´s post hoc test was employed to identify mean differences when an F-ratio was significant. The Effect Size (ES) was calculated to verify the magnitude of the differences using Cohen's d [22]. An ES of 0.20-0.49 was considered small, 0.50-0.79 medium and ≥ 0.80 large. Data were stored and analyzed using STATISTICA software version 10.0 (StatSoft Inc., Tulsa, OK, EUA).
Table 1 shows the general characteristics of the sample at pre-training according to groups. There were no significant differences for age or anthropometric measures between groups (p > 0.05).
Table 1: General characteristics of the participants at pre-training according to groups. View Table 1
Table 2 shows the pre and post-training and detraining results for muscular strength, flexibility and functional capacity according to training groups. A significant main effect of time was observed for muscular strength (MJ-SJ: +5%; SJ-MJ: +7%, small ES), flexibility (MJ-SJ: +22%; SJ-MJ: +19%, medium ES), upper-body muscular endurance (MJ-SJ: +36%; SJ-MJ: +39%, large ES), lower-body muscular endurance (MJ-SJ: +10%; SJ-MJ: +16%, small to medium ES), and agility and dynamic balance (MJ-SJ: -8%; SJ-MJ: -12%, large ES) at post-training, with no difference between the EO. There was no change on gait speed for any of the groups at pot-training.
Table 2: Muscular strength, flexibility and functional capacity in the different conditions according to the training groups. View Table 2
After detraining muscular strength (MJ-SJ = -2.5%; SJ-MJ = -7.7%), upper (MJ-SJ = -16.3%; SJ-MJ = -12.8%) and lower-body muscular endurance (MJ-SJ = -20.3%; SJ- MJ = -18.7%) significantly reduced and returned to pre-training levels, indicating that there was no retention of gains for these variables. In contrast, both groups had higher scores for flexibility compared to pre-training levels (MJ-SJ: +11%; SJ-MJ: +24.4%), indicating that flexibility gains obtained as a result of the RT program were retained. Finally, gait speed (MJ-SJ = -12.8%; SJ-MJ = -5.2%) and agility and dynamic balance (MJ-SJ = -20.6%; SJ-MJ = -20.3%) were smaller when compared to pre-training, indicating that these variables worsened after detraining. Our results were observed in both groups regardless of OE.
Figure 2 presents total training load in kg for both training groups, which significantly increased, block by block (every 4 weeks), except between weeks 9-12 and weeks 12-16, in which total training load did not increase for any of the groups (p > 0.05). There was no difference in total training load increases between groups throughout the investigation.
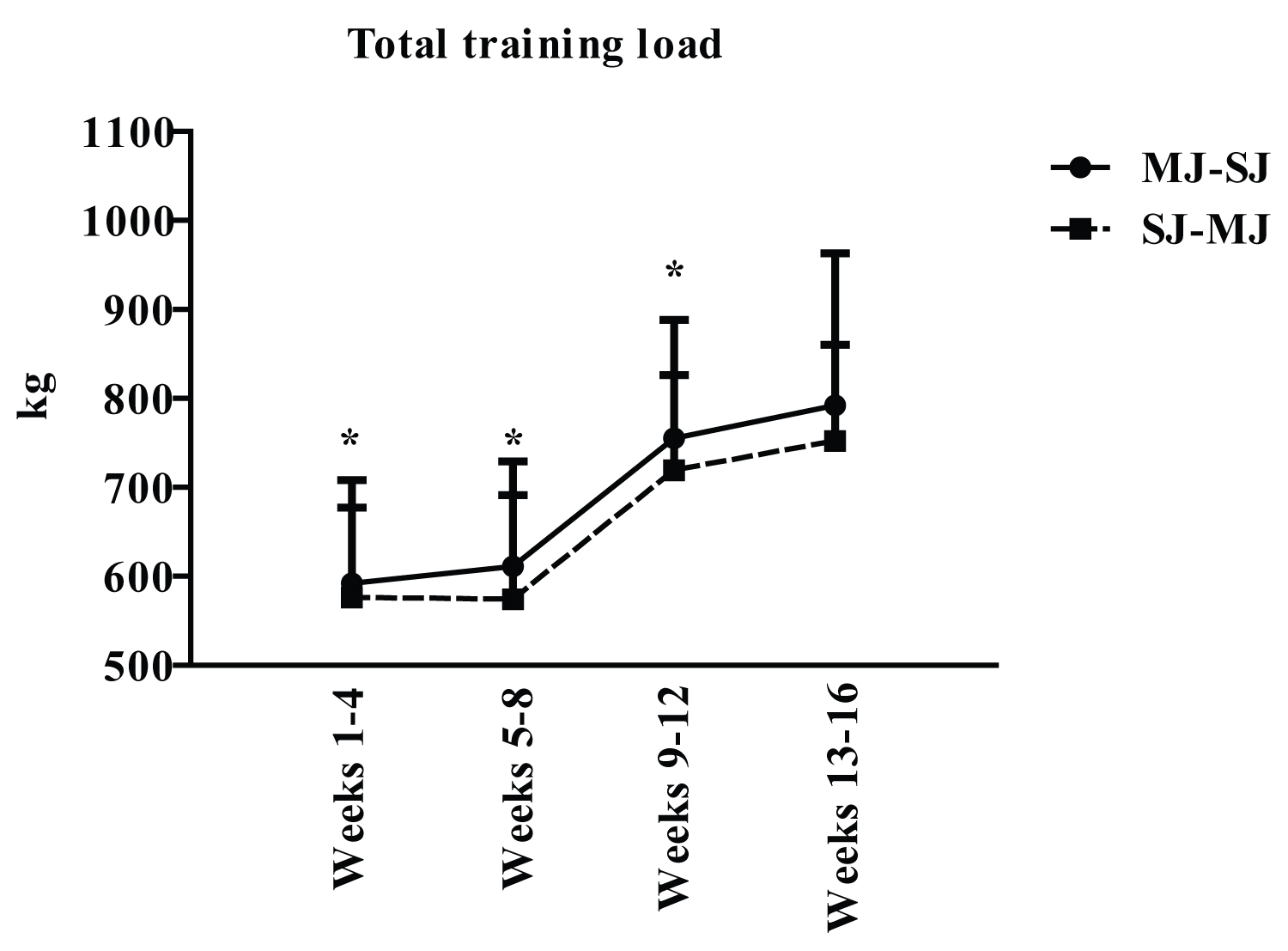 Figure 2: Total training load according to training groups, in kg.
Figure 2: Total training load according to training groups, in kg.
Note: MJ-SJ = Group that performed RT from multi-to single-joint exercises; SM = Group that performed RT from single-to multi-joint exercises. Data are presented as mean and standard deviation.
View Figure 2
Figure 3 shows individual relative changes of the participants in each of the variables analyzed, pre- to post-training, according to training groups. Despite the heterogeneity of responses, most of the participants showed an improvement in muscular strength (n = 16), flexibility (n = 20), upper-body muscular endurance (n = 21), lower-body muscular endurance (n = 18), and agility and dynamic balance (n = 19). On the other hand, few participants improved their performance in gait speed (n = 10).
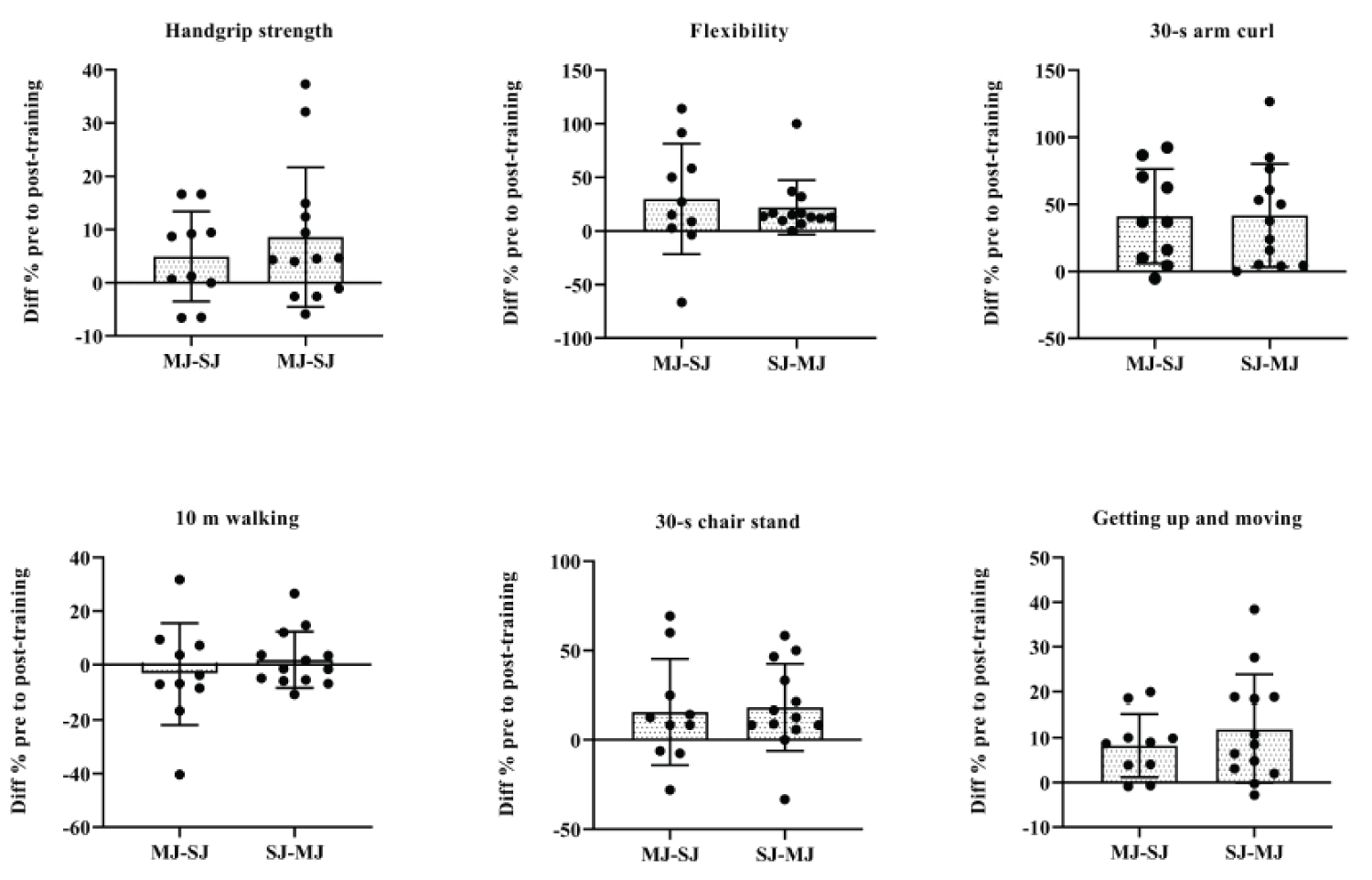 Figure 3: Individual responses for MJ-SJ and SJ-MJ participants after RT program.
Figure 3: Individual responses for MJ-SJ and SJ-MJ participants after RT program.
Note: MJ-SJ = Group that performed the exercises from multi- to single-joint order; SJ-MJ = Group that performed the exercises from single- to multi-joint order; the responses were calculated by subtracting the values of the results obtained in the pre-training evaluations from the results obtained in the post-training evaluations (post-training result - pre-training result).
View Figure 3
Figure 4 shows individual relative changes of the participants in each of the outcomes of the study, after detraining, according to training groups. The responses were heterogeneous and demonstrate that most of the participants showed a reduction in muscular strength (n = 17), flexibility (n = 14), upper-body muscular endurance (n = 19), lower-body muscular endurance (n = 22), gait speed (n = 19), and agility and dynamic balance (n = 22).
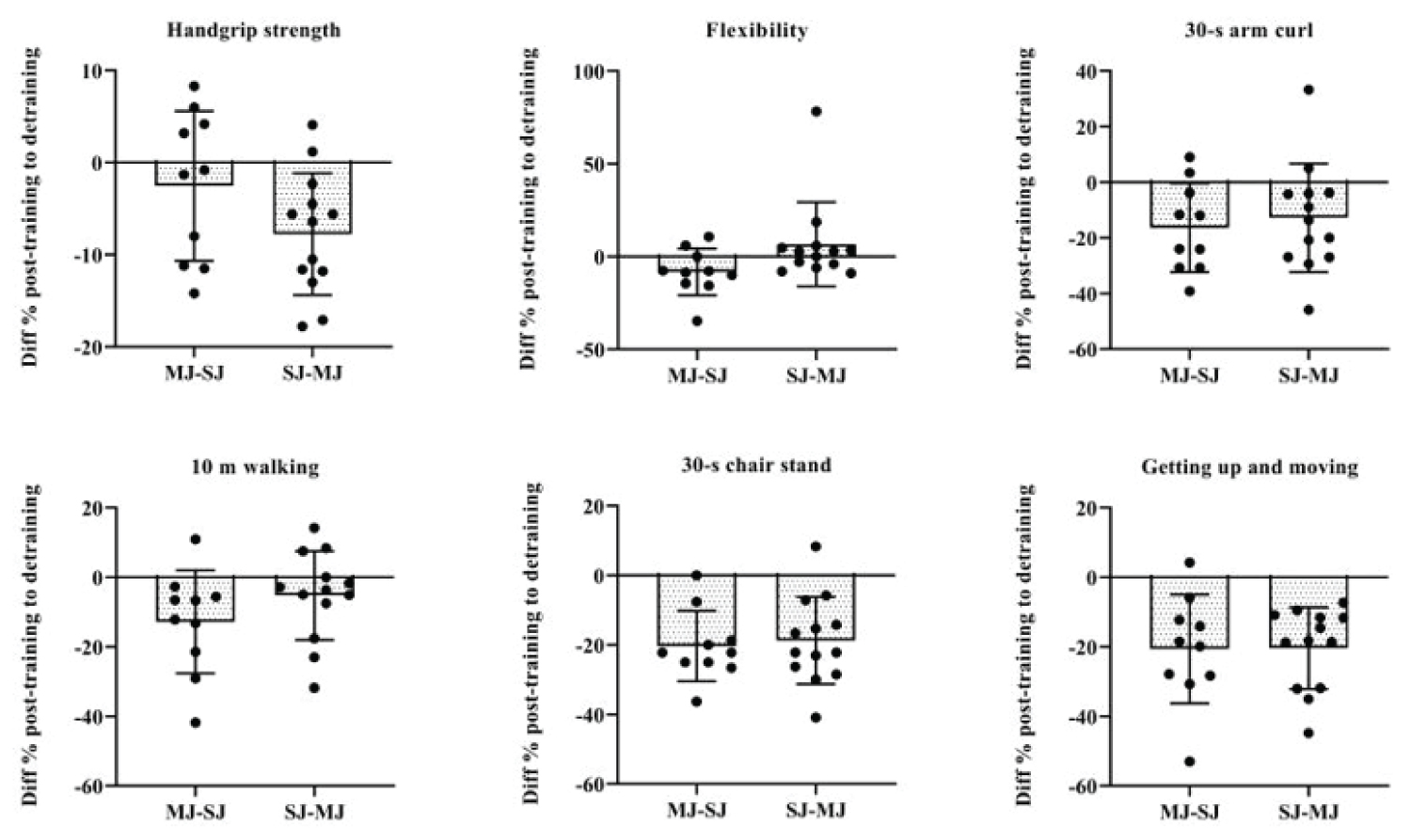 Figure 4: Individual responses for MJ-SJ and SJ-MJ group participants after detraining period.
Figure 4: Individual responses for MJ-SJ and SJ-MJ group participants after detraining period.
Note: MJ-SJ = Group that performed the exercises from multi-to single-joint order; SJ-MJ = Group that performed the exercises from single-to multi-joint order; the responses were calculated by subtracting the values of the results obtained in the post-detraining evaluations from the results obtained in the post-training evaluations (detraining results - post-training results).
View Figure 4
The main results of the present study were: (1) The effects of detraining after previous RT on muscular strength, flexibility and functional capacity indicators in older women do not depend on the manipulation of EO; (2) Detraining subsequent to the previous RT with different OE in older women did not reverse the gains in flexibility; (3) Detraining reverted increases in muscular strength and functional capacity indicators evaluated through the 30-s arm curl and 30-s chair stand test to the observed pre-training values; (4) Gait speed and agility and dynamic balance were the most affected by detraining.
The results of previous studies that submitted older adults to previous RT programs that were prescribed based on the manipulation of intensity [8,9], of weekly frequency [5,6] and volume [7] indicate that, apparently, the effects of detraining on outcomes such as muscular strength, flexibility and functional capacity are related to the efficiency of the RT program. Such results may explain, at least in part, the findings of the present study, considering that we observed that the RT program in different EO was equally efficient in improving the performance of the participants in all the analyzed outcomes, except in the 10m walking test, corroborating the findings of previous studies that submitted older adults to RT programs in different OE and concluded that the manipulation of this variable does not influence outcomes such as muscular strength and functional capacity [13,23,24].
Our results also indicate that flexibility gains were retained after detraining subsequent to the previous RT program performed with different EO. Previously, it has been suggested that detraining can reverse flexibility gains of older individuals submitted to low-intensity RT programs (40% 1RM); in contrast, moderate (60% 1RM) and high (80% 1RM) RT programs can be efficient for maintaining flexibility gains in this population [9]. These findings support, even partially, the results of the present study, since the intensity of the RT program in different OE was controlled by maintaining the repetition zone between 10-15 RM, which theoretically corresponds to 60-79% from 1RM [25].
On the other hand, detraining reversed gains in muscular strength and reduced performance in the 30-s arm curl and 30-s chair stand tests to the observed pre-training values. Recently, no changes were observed in the handgrip strength values of older people submitted to different RT volumes and subsequent detraining [7]; however, despite this divergence, some reports support our post-training results, indicating that muscular strength can increase from upper limb exercises in which handgrip strength movements are performed [26]. In addition, we understand that the reduction in handgrip strength observed after detraining is natural for the studied population, given that such capacity presents a decline in middle age onwards [27].
Our results also indicate that there was an increase in performance in the tests of 30-s arm curl and 30-s chair stand observed post-training corroborating the findings of previous researches that submitted elderly women to the practice of RT in different EO and observed gains in the order of 14.8% and 14.3% in performance in the 30-s arm curl and 30-s chair stand tests, respectively [13]. The reduction in performance in the tests in question to the pre-training values that were observed after the detraining can be attributed to the decrease in the levels of strength and muscle power of the upper and lower limbs that are associated with the decline in functional capacity [28].
The decrease in muscular strength and power levels, especially in the lower limbs, may also be related to the reduction in performance in the 10m walking tests and getting up and moving, which were the functional indicators most affected by detraining. Previously, improvements in gait speed have been shown to be associated with increased muscle strength in the lower limbs as well as improved muscle quality in older women [19].
The present study has strengths that deserve to be highlighted. To our knowledge, this is the first study that analyzed the effects of detraining after previous RT with different EO on muscle strength, flexibility and functional capacity in older women, in addition, all training sessions were supervised by professionals with experience in RT, thus, the load adjustments were continuously applied and based on the individual progress of the participants throughout the sessions, ensuring the maintenance of intensity throughout the intervention.
On the other hand, our study has some limitations, such as the sample size and the absence of a control group, which could add to the results of the present study information about the behavior of the handgrip strength, flexibility and functional capacity of older women who maintained their respective routines. Based on this information, we could advance knowledge in relation to possible differences between maintaining a lifestyle that does not include the practice of physical exercise in comparison with the effects of detraining after previous RT.
From the results presented, the present study has important practical applications. As the outcomes of detraining were similar regardless of OE, professionals working in the prescription of RT can advocate the manipulation of other variables that can minimize the effects of detraining in elderly women who may interrupt the training program. In addition, the pandemic caused by the new coronavirus affected the routine of elderly women, who reported greater social isolation compared to men [29], with this, it is likely that this population is abstaining from the practice of RT. Given the above, the results of the present study provide an overview of the effects of detraining on outcomes related to health and quality of life of elderly women.
We conclude that the effects of detraining after previous RT on handgrip strength, flexibility and functional capacity indicators do not depend on the manipulation of EO. Only flexibility and two of the six functional indicators evaluated (getting up from floor and put on socks) were not negatively affected by detraining, therefore, interrupting RT programs can compromise the gains in muscular strength and functional capacity of older women.
The authors declare that they have no conflict of interests regarding the publication of this article.
We would like to thank the General Superintendent of Science, Technology and University Education (SETI) and University without Borders (USF) for the financial support, and all the participants for their engagement in our study.