Measles and malaria are highly infectious diseases worldwide and are of major public health concern. Although measles is a leading cause of death of young children in many developing countries, it is vaccine preventable. This study was carried out to determine the seroprevalence of measles IgM as well as the prevalence of malaria parasite among febrile children attending Ahmadu Bello University Medical Center, Samaru Zaria, Nigeria. A total of 80 blood samples purposively and randomly collected were analyzed for measles virus IgM and malaria parasites using ELISA (Diagnostics Automation/Cortez Diagnostics, California) and microscopy respectively. Data concerning demography, risk factors and clinical symptoms were collected using questionnaire. The result was analyzed using SPSS version 21 and Chi-square at 95% confidence interval and p ≤ 0.05 was considered significant. Out of the 80 samples analyzed, 64 (80.0%) were seropositive for measles virus IgM antibody. Children within 10-12 years had the highest seroprevalence of measles IgM (88.9%: 8/9) while those within 4-6 years had the lowest (76.3%: 29/38). The antibody was detected more in female children (83.8%: 31/37) compared to male children (76.7%: 33/43). For malaria parasite, 40.0% (32/80) of the children were positive for malaria, with the highest prevalence (55.0%: 5/9) obtained among children who were 10-12 years, while the least (30.8%: 4/13) was recorded among children within 1-3 years. Malaria parasite was distributed with higher frequency among female children (40.5%: 15/37) compared to male children (39.5%: 17/43). Measles and malaria co-infection was detected in 26 of the 80 (32.5%) children. Vaccination status, reddening of eyes, cough and weakness were the factors found significantly associated with measles (P ≤ 0.05) while the use of insecticide treated net and vomiting were significantly associated with malaria (P ≤ 0.05). Proper and complete vaccination of children against measles and effective use of insecticide treated mosquito net is recommended.
Measles is a highly contagious viral disease caused by Morbillivirus; a member of the Paramyxovirus family, which is transmitted to susceptible individual through aerosol or by direct contact [1]. Measles occurs only in human with no known animal reservoir. The virus infects the mucous membranes of exposed individual and then spreads to other part of the body [1,2]. It is characterized by prodromal fever, which begins about 10 to 12 days after exposure to the virus, and lasts 4 to 7 days. A runny nose, a cough, red and watery eyes, and small white spots inside the cheeks can develop in the initial stage. After several days, a rash erupts on the face and upper neck which spreads, eventually to the hands and feet [3]. Neurological complications occur more often and manifest in the form of acute or chronic encephalitis [4].
Because of gaps in vaccination coverage, measles outbreaks occurred in all regions globally between 2017 and 2018 with an estimated 110,000 deaths mostly among children under the age of five [3]. Nigeria is one of the ten countries in the world with measles vaccine coverage of less than 50% [5]. Measles is endemic in Nigeria with recurrent outbreaks occurring at irregular intervals. In 2019, Nigeria reported 30,457 suspected cases to the WHO of which 24,994 were confirmed. Kaduna state accounted for 1,370 of the confirmed cases in Nigeria [6] and Zaria is a Local Government Area in the state.
Malaria is an acute febrile illness caused by the protozoan parasite, Plasmodium (P). In human, malaria is caused by four different species of Plasmodium: P. falciparum, P. malariae, P. vivax and P. ovale. In addition, P. knowlesi that normally infect animal occasionally infect human [7]. The most common cause of malaria in the hotter and humid regions of Africa is P. falciparum accounting for 99.7% of all malaria cases [7]. Malaria parasite is transmitted by female anopheles mosquito which bites mainly between dusk and dawn causing variable clinical features that includes fever, chills, headache, muscular aching and weakness, vomiting, cough, diarrhoea and abdominal pain. The incubation period of malaria is 7 days or longer, thus, a febrile illness developing less than one week after the first possible exposure may not likely be malaria.
Malaria is a life-threatening disease in many tropical and sub-tropical areas and there is a risk of its transmission in over 100 countries and territories where over 125 million international travelers visit every year [7]. According to reports by WHO [7], fifteen countries in sub-Saharan Africa and India bear almost 80% of the global malaria burden. Five countries accounted for nearly half of all malaria cases worldwide: Nigeria (25%), Democratic Republic of the Congo (11%), Mozambique (5%), India (4%) and Uganda (4%). In 2018, Bernard, et al. [8] reported a malaria incidence of 66.7% in Zaria, an indication of endemicity in this population.
Children are at risk of serious consequences or even death if they become infected with malaria or measles or are co-infected by both diseases. Fever is a common clinical feature of both malaria and measles. Despite the availability of vaccine for measles and effective control programme for malaria in Nigeria, measles and malaria are still endemic in the country [9]. In addition to vaccination, WHO recommends that laboratory surveillance should be included in each country's measles and malaria control Programme [10]. Limited information is available on measles and malaria co-infection in the study area. The study was therefore conducted to detect measles and malaria among febrile children in Zaria, Kaduna State, Nigeria.
The study was conducted at Ahmadu Bello University (ABU) Medical Center, Samaru Main Campus, Zaria, Nigeria. The ABU Medical Centre is a medical facility with capacity to consult 500 to 1000 patients per day. The total number of students and staff living in the Samaru is estimated at 50, 000. Zaria lies on the high plains of Northern Nigeria at an altitude of 670 m above sea level and located at a latitude 11°04 and longitude 7°42°E. The climatic conditions in Zaria are tropical with well-defined wet and dry season.
The study population consisted of children of all sexes with febrile condition who were presented at the ABU Medical Centre. In addition to fever, these children were those presenting with either cough, coryza, conjunctivitis or symptoms of malaria parasite infection or a combination of two or more of these symptoms.
Children included in the study, were febrile children between 1-12 years-old, who presented with suspected sign and symptoms of measles or malaria and whose parents or caregiver consented. Non consenting febrile children as well as those outside the age group who were not presenting with measles and malaria sign and symptoms were excluded from the study. Informed consent was obtained from each participant caregiver and ethical approval was obtained from the research Ethical Committee of the Medical Center. Convenient sampling method was employed in recruiting the participants.
Between February and May 2018, about 2 ml of blood was aseptically collected from each of the 80 children enrolled in the study. The blood sample was collected by a laboratory technician and was divided into two parts. The first portion of each of the blood sample was dispensed into sterile labeled plain sample bottles, allowed to clot and spun for 3 minutes at 3000 rpm to obtain the serum. The second portion of the blood was used in preparing thin smear for malaria parasites investigation.
A thin film was prepared on a glass slide by placing a drop of blood on a clean and labeled glass slide. Another slide was inclined about angle 45° used to spread the blood to obtain a head, body and a smooth tail (fish tail). The slide was air dried on a staining rack, fixed with methanol for 3 minutes and allowed to air dry. Already prepared Giemsa stain was poured on the slide for about 30 minutes and rinsed. The slides were air dried and viewed under the microscope using 100 x objectives (oil immersion).
Assay (ELISA) procedure: Measles specific IgM antibodies in serum were detected by enzyme immunoassay (Diagnostics Automation, U.S.A) in accordance with the manufacturer's instruction.
The results of the laboratory analysis and data obtained from the questionnaires were analyzed using Statistical Package for Social Science (SPSS) version 21. Pearson Chi square test at 95% confidence interval and a significant level of 0.05 was used to determine the relationship between the socio-demography data and the seroprevalence rate.
A total of 64 out of the 80 children were found to be positive for measles IgM giving a prevalence of 80.0%, while 32 (40.0%) of the children were malaria positive (Figure 1). A total of 26 children (32.5%) were co-infected with measles and malaria giving a sero-prevalence of 32.5%.
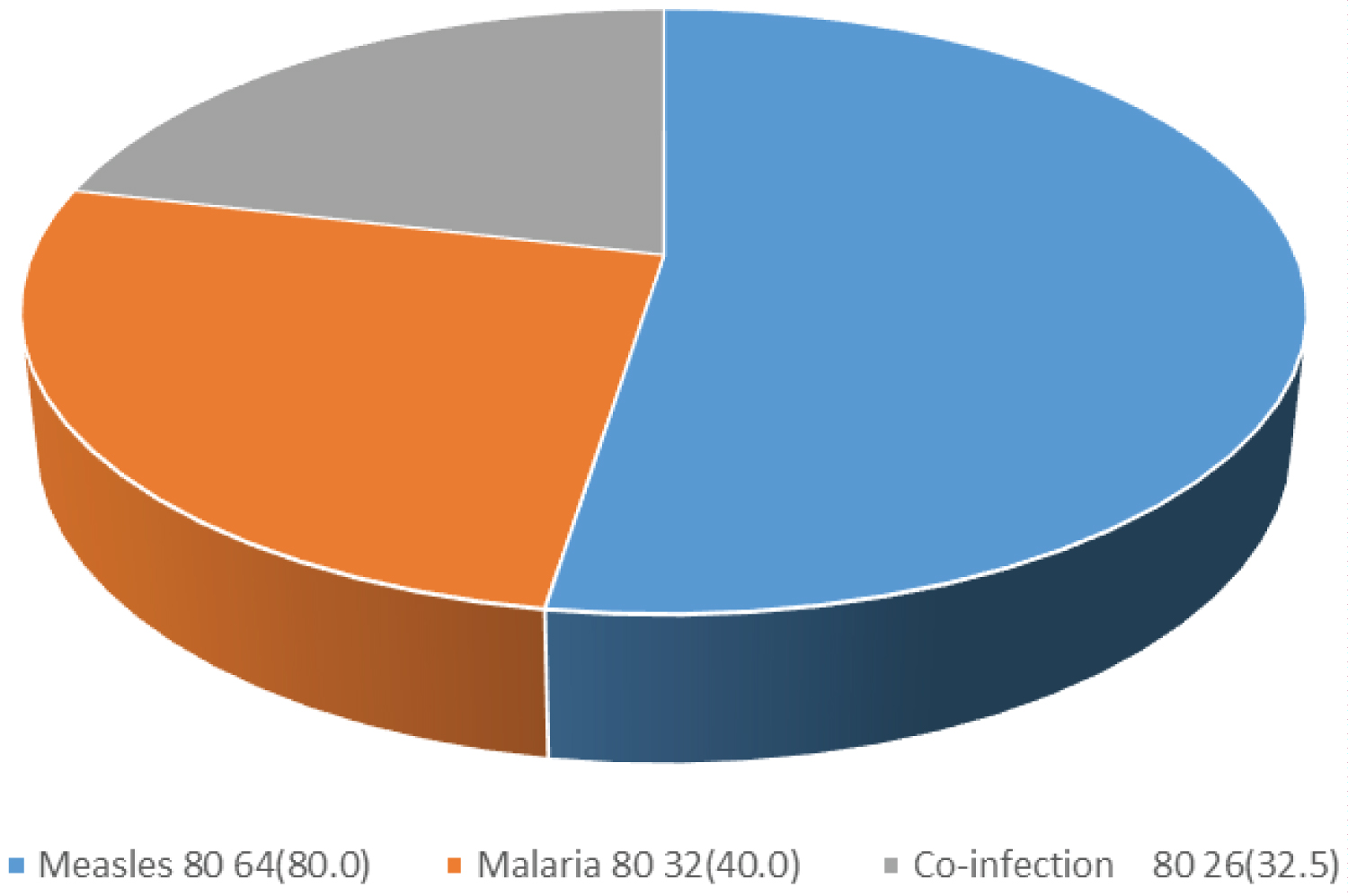 Figure 1: Seroprevalence of Measles IgM and Malaria Parasites among Febrile Children attending Ahmadu Bello University Medical Center Samaru Main Campus, Zaria.
View Figure 1
Figure 1: Seroprevalence of Measles IgM and Malaria Parasites among Febrile Children attending Ahmadu Bello University Medical Center Samaru Main Campus, Zaria.
View Figure 1
The sero-prevalence of measles IgM among febrile children with respect to gender and age is shown in Table 1. Out of 80 blood samples analysed, 43 (53.75%) were obtained from male children and 37 (46.25%) from female children. Higher prevalence rate (83.8%: 31/37) was obtained among female children compared to male children (76.7%: 33/43) with no significant difference (χ2 = 0.616, df = 1, P = 0.433). Children within age group 10-12 years had the highest prevalence (88.9%: 8/9) while children within age group of 4-6 years had the lowest prevalence (76.3%: 29/38). The difference observed was statistically insignificant (χ2 = 1.156, df = 3, P = 0.764).
Table 1: Seroprevalence of Measles IgM and Malaria Parasite among Febrile Children in Relation to Gender and Age. View Table 1
Higher malaria prevalence rate (40.5%: 15/37) was obtained among female children compared to male children (39.5%: 17/43) with no significant difference (χ2 = 0.008, df = 1, P = 0.927). The prevalence of malaria among febrile children with respect to age is shown in Table 2. Children within the age range 10-12 years had the highest prevalence (55.0%: 5/9) while children within age range of 1-3 years had the lowest prevalence (30.8%: 4/13). The difference observed was statistically insignificant (χ2 = 1.735, df = 3, P = 0.629).
Table 2: Seroprevalence of Measles IgM and Malaria Parasite among Febrile Children in Relation to Risk Factors. View Table 2
The sero-prevalence of measles IgM and prevalence of malaria among febrile children in relation to associated risk factors are presented in Table 3. Only vaccination was found to be significantly associated with the incidence of measles among children (χ2 = 9.091, df = 1, P = 0.003). Similarly, only the use of insecticide treated net was found to be significantly associated with the incidence of malaria among febrile children (χ2 = 27.778, df = 1, P = 0.000). There was no significant association between malaria and measles vaccination among febrile children (P > 0.05). Vaccinated children were two times more likely to be infected with malaria (OR = 2.143, 95% CI = 0.771-5.953).
Table 3: Seroprevalence of Measles IgM and Malaria Parasite among Febrile Children in Relation to Signs and Symptoms. View Table 3
The results obtained with respect to signs and symptoms of Measles are shown in Table 4. Reddening of the eyes (P = 0.00), cough (P = 0.00) and weakness of the body (P = 0.044), were found to be significantly associated with measles. Febrile children with headache were more than four times more likely to be infected with measles (OR = 4.451, 95% CI = 3.213-6.789). Children with body weakness were five times more likely to be infected with measles (OR = 5.276, 95% CI = 3.348-8.305), while fever and headache were found to be constantly associated with measles. Rashes and vomiting were not found to be significantly associated with Measles (P > 0.05). As presented in Table 4, only vomiting was found to be significantly associated with malaria (χ2 = 14.732, df = 1, P = 0.00), while reddening of the eyes, rashes, cough, weakness of the body were not significantly associated with malaria (P > 0.05). Fever (40.0%) and headache (40.0%) were found to be constantly associated with malaria. Febrile children with body weakness were about two times more likely to be infected with malaria (OR = 1.681, 95% CI = 1.401-2.016) and children who were vomiting were twenty-two times more likely to be infected with malaria (P = 0.00; OR = 22.14, 95% CI = 2.79-175.89).
Table 4: Measles and Malaria Co-infection in Relation to Gender and Age group. View Table 4
Results of co-infection of children with measles and malaria in relation to gender and age are shown in Table 5. A similar co-infection rate (32.6%: 14/43) was seen among male and female children (32.4%: 12/37) (χ2 =0.000, df = 1, P = 0.990). Children within the age range 10-12 years had the highest co-infection rate (44.0%: 4/9) while children within age range of 1-3 years had the least (15.4%: 2/13). The difference observed was not statistically significant (χ2 = 2.849, df = 3, P = 0.416).
Table 5: Measles and Malaria Co-infection in Relation to Risk factors. View Table 5
The sero-prevalence of measles and malaria co-infection among febrile children in relation to associated risk factors is presented in Table 6. Only the use of insecticide treated net was found to be significantly associated with co-infection among children (χ2 = 17.094, df = 1, P = 0.000). Measles vaccination among febrile children was not significantly associated with co-infection (P > 0.05).
Table 6: Measles and Malaria Co-infection among Febrile Children in Relation to Signs and Symptoms. View Table 6
As presented in Table 6 with respect to signs and symptoms, cough (P = 0.054) and vomiting (P = 0.002) were found to be significantly associated with co-infection. Febrile children that had cough were two times more likely to be co-infected with malaria and measles (OR = 2.539, 95% CI = 0.971-6.641). Children that vomited were fourteen times more likely to be co-infected with malaria and measles (OR = 14.706, 95% CI = 1.849-116.972). While fever and headache were found to be constantly associated with co-infection. Children with fever were more than two times (OR = 2.436, 95% CI = 0.876-5.678) while those with headache were almost two times (OR = 1.567, 95% CI = 0.554-4.231) more likely to be co-infected. Rashes, reddening of eyes and body weakness were not found to be associated with co-infection (P > 0.05). Febrile children with reddening of eyes were two times more likely to be co-infected (OR = 1.705, 95% CI = 0.662-4.386).
This study found the seroprevalence of measles IgM among febrile children attending the Ahmadu Bello University Medical Center Samaru Main Campus, Zaria to be 80.0%. This implies that, there might have been a silent outbreak of measles among children in the study area during the study period. This assertion is buttressed by the fact that, the 80% rate obtained in the present study is higher than rates of 32.2% [11] 21.2% [12] and 35.10% [13] previously reported among children in Kaduna State. Consequently, if these children's symptoms are not properly diagnosed and treated, they might develop complication involving the central nervous system [14,15]. Detection of measles IgM remains the gold standard for diagnosis of measles infection as recommended by the WHO in surveillance guidelines for measles, in the WHO African Region [6].
The results of this study shows that measles is still a major challenge to Nigerian health system. Nigeria still ranked high among countries reporting highest measles infections yearly as seen in the WHO report of 2019 [6]. Measles infection among previously vaccinated children as seen in this study has been reported to be milder and usually subclinical [15] and is probably due to vaccine failure. It is not known from this study whether primary vaccine failure or secondary was the major cause of infection in the vaccinated children, as there was no data available on the seroconversion status of the children after vaccination. Causes of primary vaccine failure could be failure of the cold chain, inadequate viral dose and host immune factors such as persistence of maternal immunity [16]. Nutritional status of the children as well as presence of other underlying diseases such as malaria and HIV among others could be responsible for secondary vaccine failure although these factors were not determined in this study.
About 40.0% of the children were found to have malaria and were infected with only P. falciparum. This rate of infection is considerable, even though it is lower than a rate previously reported in the area [17]. This considerable low percentage of parasitaemia might be as a result of effective use of insecticides treated net as 75% of the children said they sleep under treated nets.
The seroprevalence of measles-malaria co-infection was found to be 32.5%, and this might have exacerbate the condition of the children. Measles IgM was detected with a slightly higher prevalence among female children, but did not reach a significant level, implying infection was due to chance. This finding is not in agreement with the report of Abdulfatai, et al. [13] and Chechet, et al. [11] but was similar to the report of Shohat, et al. [18] and Bassey, et al. [19] who found more female children infected than male but with a significant level.
The seroprevalence of measles IgM with respect to age was found to be higher among children who were within 10-12 years-old. This indicate higher circulation of measles virus among older children as previously reported by Olaitan, et al. [12] and Wichmann, et al. [9]. This shift of infection to older children might probably be due to lack of immunization and consequently susceptibility to infection. This finding might also be due to past weak immunization efforts resulting in lack of provision of a second dose of measles vaccine at supplementary vaccination activities or incomplete course of routine vaccination among children [9].
There was an association between measles virus infection and vaccination status of the children. Vaccinated children had the highest seroprevalence as previously reported by Abdulfatai, et al. [13] and Aaby, et al. [15]. Detection of measles IgM in a vaccinated child implies re-infection or lack of seroconversion. This finding also implies that any non-immune person can become infected. A non-immune person is one that has not been vaccinated or was vaccinated but did not develop immunity due to primary or secondary vaccine failure. Seroconversion after measles immunization is mainly affected by incomplete immunization process, loss of vaccine potency and interference of maternal antibodies. Treatment with drugs known to interact with the measles vaccines may also cause vaccine failure [16,20]. Non-immune young children in the study area are therefore at highest risk of measles infection and its complications, including death. Measles complications are common and may be quite serious, thus emphasizing the need for proper and complete measles immunization.
Signs and symptoms such as fever, reddening of eyes, cough, headache, and body weakness were significantly association with measles virus infection. This agrees with WHO [3] and Jawestz, et al. [21] on the clinical case definition of measles virus symptoms.
Similar to measles IgM, malaria parasite was also detected with slightly higher prevalence among female children. This implies that, female children were probably more exposed to malaria parasite than male children during the study and the difference observed might be due to chance. Similar finding was previously reported by Achonduh-Atijegbe, et al. [22].
Older children were also more susceptible to malaria parasite in this study as previously reported by WHO [23]. This finding could probably be due to more frequent exposure to infected mosquito bite by these older children who tend to play more outdoors. More so, younger children are seen often more under the protective care of their parents and frequently sleep under insecticide treated mosquito net compared to older children. Older children in the study were therefore more at risk of coming down with malaria which might result in complications such as cerebral malaria, malarial hyperpyrexia and hemoglobinuria, if not treated on time.
Infection with malaria parasite was significantly associated with the use of insecticide treated net. Plasmodium falciparum was detected more in children who slept under insecticide treated nets. This observation reiterates the importance of the use of insecticide treated nets, a practice that can prevent malaria infection and its complications. The WHO [24,1] had recommended the use of insecticide treated nets to prevent mosquito bite for young children as well as Achoduh-Atijegbe, et al. [22].
In this study, fever, headache and vomiting were found to be significantly associated with malaria as previously reported by Achoduh-Atijegbe, et al. [22] and Aminu, et al. [17]. Cough, red eyes and weakness were significantly associated with measles, while fever, cough and vomiting were significantly associated with measles and malaria co-infection. Malaria is still endemic in Nigeria and the infection is known to interact with some Expanded Programme on Immunization vaccines [25]. Misdiagnosis of measles is common in endemic areas resulting in harm to vulnerable populations. Therefore, efforts need to be made to obtain clinical specimens for confirmation of disease in all suspected cases. Several diagnostic tests for measles exists, but some are limited by low positive predictive value in low transmission settings. The signs and symptoms found to be significantly associated with measles in this study can be therefore be used to complements laboratory test report for accurate diagnosis of measles in children that present with febrile conditions.
This study found a high seroprevalence of 80.0% for measles IgM among febrile children in Zaria, signifying a silent outbreak of measles among the children during the study period. Measles antibodies were detected mostly among vaccinated children, indicating re-infection or lack of sero-conversion. Malaria parasites were detected in 40% of children confirming its endemicity in the study area. Vomiting and cough were strongly associated with malaria and measles respectively, while fever, cough and vomiting were significant associated with measles and malaria co-infection detected in 32.5% of the children. The study reiterated the use of insecticide treated nets as a protective factor for malaria.