CT: Computed Tomography; ED: Emergency Department; GCS: Glasgow Coma Scale, HGG: High-grade Glioma; MRI: Magnetic Resonance Imaging
As physicians and neurosurgeons, our daily practice in Emergency Departments sometimes calls us to manage patients and to take decisions in sub-optimal conditions, maybe with partial anamnesis, incomplete neurological examinations or with lacks in routine radiological and laboratory exams. Such eventuality, although it may sometimes lead to misdiagnose and to confound some pathological conditions, fortunately is not always linked to bad repercussions for patients. This is especially true when decision-making processes are mainly guided by symptoms and clinical signs, rather than preconceptions and opinions linked to a professional deformation process.
As an example of this general warning, we present the case of a 55-year-old man suffering an acute right hemiparesis with consciousness impairment due to a brain multi-cystic disease, initially attributed to neuro-cysticercosis, but eventually found to be a metastatic localization of a lung tumor. Following the principle described above, the patient underwent a simultaneous double-biopsy procedure of the two main cysts looking for brain decompression, irrespective of the disease hypothesis, following what clinical conditions required free from preconceptions, assuring him a good outcome.
A 55-year-old Asian man was carried to our Emergency Department (ED) in a confusional state, complaining a serious hemiparesis equally affecting his right arm and leg, started the day before, about three months after a return trip from his native home in a small village of East China (Glasgow Coma Scale (GCS) 13, E4V3M6). In recent years the patient lived in very poor conditions in Italy, without a stable work situation. His anamnesis was characterized by an history of several alcohol-related problems, without any smoking habit. Patient complained fever (37.3 ℃) by some days and routine lab exams showed a small increase in inflammation indexes. Routine bed thoracic X-ray did not show any pathological findings and an urgent Head-Computed-Tomography (CT) scan disclosed three large hypodense cystic lesions in the left hemisphere, solid nodules within them after contrast administration, with a clear mass effect and initial uncal herniation, then confirmed by Magnetic Resonance Imaging (MRI) (Figure 1). It is well known among neuro-specialists that ring-enhancing lesions may be linked to High-Grade Gliomas (HGG), metastasis, or infectious cerebral diseases [1-5]. In this particular case, the radiological findings of multiple cystic lesions with nodules within them, together with the anamnestic notes, suggested us an infectious disease, like toxoplasmosis, tuberculosis or, above all the most likely, neuro-cysticercosis [5-10].
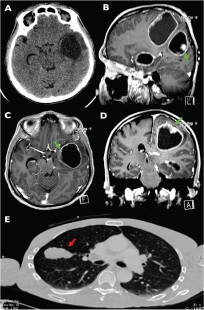 Figure 1: A) Brain axial CT-scan of the head performed at the arrival of the patient at the Emergency Department showing a left temporal cystic lesion causing a clear mass effect on surrounding structures; B-D) Brain MRI (T1-weighted sequences with contrast administration) showing posterior frontal, parietal-occipital and temporal cystic lesions in the left hemisphere, characterized by peripheral contrast enhancement and solid nodules within them (green arrows) after contrast administration, exerting a trans-falcine herniation; E) Lung axial CT-scan with contrast administration showing a 5 cm mass in the anterior segment of the superior lobe of the right lung (red arrow), characterized by contrast enhancement. Brain specimen histological analysis confirmed the malignant nature of parenchymal lesions (microcytoma metastasis).
View Figure 1
Figure 1: A) Brain axial CT-scan of the head performed at the arrival of the patient at the Emergency Department showing a left temporal cystic lesion causing a clear mass effect on surrounding structures; B-D) Brain MRI (T1-weighted sequences with contrast administration) showing posterior frontal, parietal-occipital and temporal cystic lesions in the left hemisphere, characterized by peripheral contrast enhancement and solid nodules within them (green arrows) after contrast administration, exerting a trans-falcine herniation; E) Lung axial CT-scan with contrast administration showing a 5 cm mass in the anterior segment of the superior lobe of the right lung (red arrow), characterized by contrast enhancement. Brain specimen histological analysis confirmed the malignant nature of parenchymal lesions (microcytoma metastasis).
View Figure 1
Considering the sudden worsening (in 2-3 hours by the Emergency Department admittance) of both hemiparesis and general neurological status, quickly leading the patient to a comatose state (GCS 7, E2V2M3) he underwent a simultaneous stereotactic double-biopsy procedure of the two main cysts on the same day of ED admittance, to obtain a quick decompression and a microbiological/cytological analysis (Figure 2). Histological findings resulted in small-cell pulmonary carcinoma metastasis, then further studied with thoracic CT with contrast administration. The cognitive and clinical conditions of the patient quickly improved after surgery (GCS 15) and he was addressed to oncologists/radiotherapists and rehabilitation clinic on day 10 post-op.
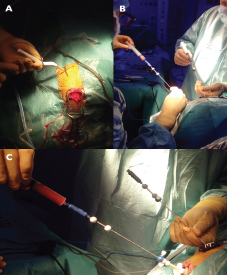 Figure 2: A) Stereotactic biopsies were performed with the aid of neuronavigation (Stealth S7® - Medtronic, Minneapolis, USA); B) Intraoperative view of the simultaneous aspiration and double-biopsy procedure of the two main cysts; C) Particular of biopsy procedure: biopsies were simultaneously performed by one surgeon, using a skull mounted trajectory guide system (Navigus® frameless biopsy system, Medtronic).
View Figure 2
Figure 2: A) Stereotactic biopsies were performed with the aid of neuronavigation (Stealth S7® - Medtronic, Minneapolis, USA); B) Intraoperative view of the simultaneous aspiration and double-biopsy procedure of the two main cysts; C) Particular of biopsy procedure: biopsies were simultaneously performed by one surgeon, using a skull mounted trajectory guide system (Navigus® frameless biopsy system, Medtronic).
View Figure 2
As said, the appearance on MRI of brain ring-enhancing lesions may suggest different diseases [6-10]. As this is the case, it can be said that brain metastases usually are present in 15-40% of patients with cancer, many of them are asymptomatic [2]. Certain malignancies are often associated with brain metastases, including cancers of the lung, breast, skin, colon, pancreas, testes, ovary, cervix, renal cell carcinoma, and, frequently, melanoma [11,12]. When symptoms become evident, headache, seizure, syncope, focal neurological deficit, or papilledema may be present. Brain metastases are solitary approximately in 50% of the cases, in 20% of the time is possible to find two lesions, and in 30% of the time, three or more lesions are disclosed [13]. Some tumors (breast, renal cell, colon, and thyroid) are more commonly solitary, while others such as lung cancer and melanoma tend to create multiple localizations of metastatic disease [14].
While metastasis from small-cell lung cancer may often present as multiple and hemorrhagic lesions, localized at the white-gray matter border and surrounded by edema [2], viable cysts of neuro-cysticercosis usually present as small round areas with the scolex appearing as a nodule of high density within the cyst; large cysts are not uncommon [7,15], and this was the most likely preoperative diagnosis in this case. Neuro-cysticercosis is still an important public health issue worldwide and is widely prevalent in many countries with high poverty in sub-Saharan Africa, Asia, and Latin America. Nevertheless, the number of cases in non-endemic countries has also increased due to international travels and migrations [7,10,16,17].
Far from us the intention to discuss whether the differential diagnosis may have been correctly done before, what seems to be important is to keep in mind how, in an emergency setting, quick anamnesis and partial routine exams may deceive the differential diagnosis process. Nevertheless, symptoms and clinical signs should be the key factors in leading decision-making processes, especially when urgency requires prompt and quick decisions. In fact, it should be noted that apart from looking for a histological/microbiological diagnosis, the primary surgical indication would have had the same rationale irrespective of the disease hypothesis, following what clinical conditions required: to reduce intracranial pressure with simultaneous aspiration of two cysts, to avoid lack of accuracy in surgical maneuvers due to possible brain shift, as it could have occurred with a standard surgical removal of multiple lesions. With this case-report we want to stress, therefore, the necessity to manage urgency and emergency patients mainly following what contingency and neurological status requires, free from preconceptions.
1. Diagnosis and patient management in urgency may be difficult;
2. Brain ring-enhancing lesions are usually associated to glioma, metastasis or cerebral abscesses;
3. Keeping in mind also minor causes of brain ring-enhancing lesions may help in the prompt treating of patients affected by rarer diseases;
4. In urgency, treating patients keeping in mind symptoms and signs is advocated;
5. A case treated following such suggestions is here presented.