Ganglioneuromas of the cervical spine are rare lesions. There are only 6 documented cases in the existing literature that are associated with neurofibromatosis type 1, in which all patients presented with tetraparesis.
We present a case of a young female with NF1, who developed bilateral upper limb paresthesia after a minor fall. Her neurological examination was consistent with cervical myelopathy, with long tract signs evident but no loss of power. MRI of the cervical spine showed bilateral dumbbell ganglioneuromas at C2 with intradural extension and compression of the cervical cord with myelomalacia. The patient underwent posterior C1-2 decompressive laminectomies and excision of these lesions.
Cervical ganglioneuromas are rare lesions that should be considered in the NF1 patient with signs of myelopathy. While they are typically benign, there are isolated reports of malignant transformation and long-term surveillance may be warranted.
Cervical bilateral dumbbell ganglioneuroma, Neurofibromatosis
NF1: Neurofibromatosis Type 1; CGN: Cervical Ganglioneuroma
Cervical ganglioneuromas producing spinal cord compression are very uncommonly reported in the English literature. Dumbbell CGN in association with NF1 are even fewer, with only 6 previously documented cases. Typically, spinal tumours associated with NF1 are histologically found to be neurofibromas. This case of bilateral dumbbell CGN causing cervical myelopathy in a patient with NF1 highlights the rarity of these lesions, and the need to consider them in the differential diagnosis.
A 42-year-old female was referred to the neurosurgical clinic with a complaint of bilateral upper limb numbness and headaches for one week. This occurred after a fall from standing height, with no head or cervical spine trauma. The numbness was consistent with paresthesia and involved the C5-T1 dermatomes bilaterally. Her headaches were in the occipital region, constant, and graded as 5/10 severity. There was no associated nausea/vomiting, fever or seizures.
The remainder of the history was significant for neurofibromatosis type 1, which was clinically diagnosed previously (axillary freckling, more than 6 café-au-lait spots larger than 15 mm, more than 2 neurofibromas). Physical examination was consistent with the above findings of NF1. Neurological examination did not reveal any abnormality of gait or tone, and power was graded as 5/5 in all limbs. However, reflexes were brisk (3+) in all limbs, and her plantars were up going bilaterally. There was neither clonus nor a positive Hoffman's sign.
MRI of the brain and cervical spine was ordered, and it revealed enlarged dorsal root ganglia bilaterally at C2, C3 and C4 nerves. These were most prominent at C2 nerve roots bilaterally, with medial and anterior enlargement that extended intradurally and compressed the cervical spinal cord (Figure 1). Hyperintense signal on T2 sequences were noted on the cord at this level, consistent with myelomalacia. MRI of the brain was within normal limits. The patient consented to posterior C1-2 decompression and excision of the C2 nerve root tumours, with the possibility of C1-2 fusion if instability was created.
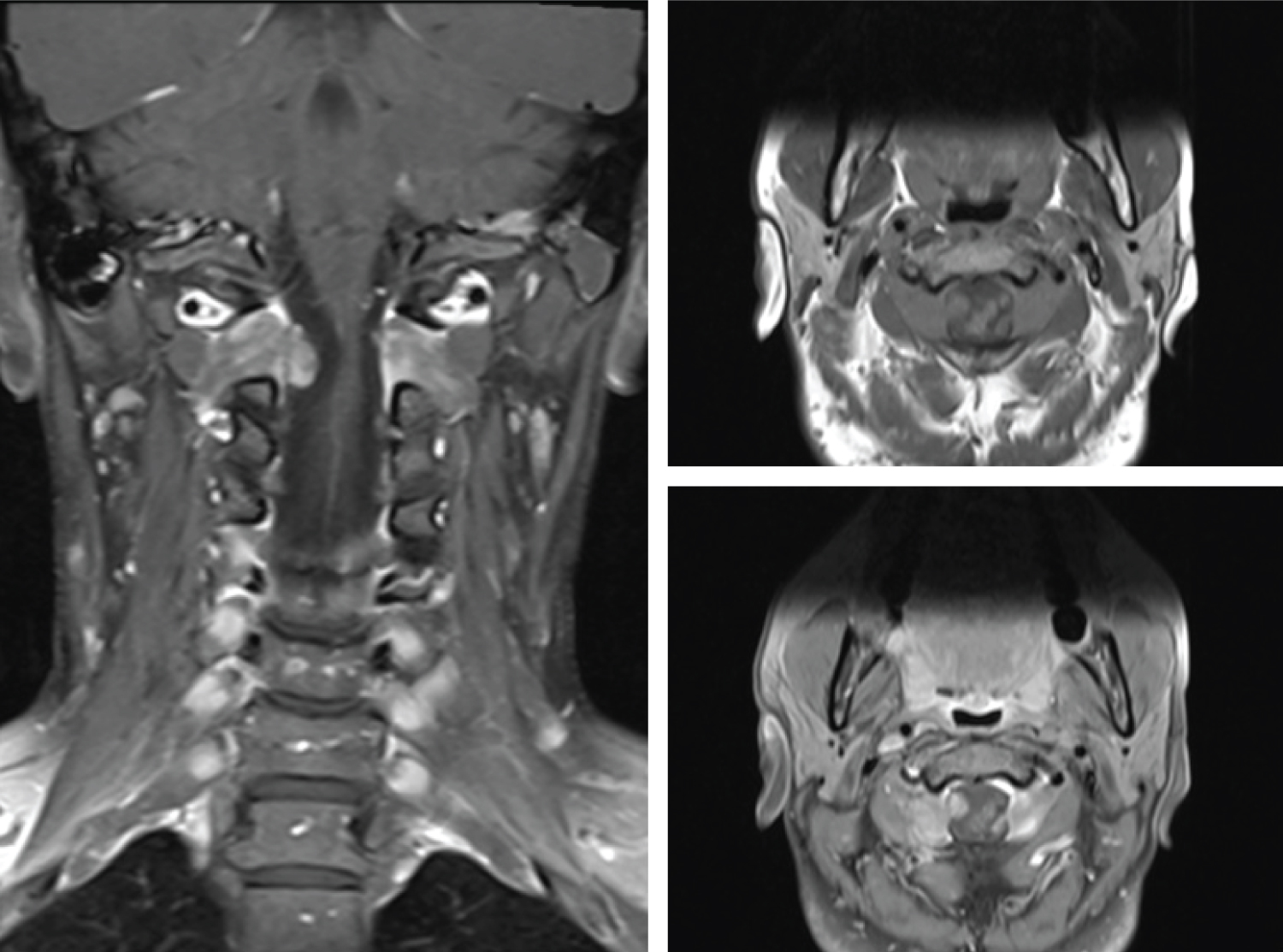 Figure 1: Left image - pre-operative coronal T1 post-contrast MRI showing bilateral dumbbell C2 tumour with intradural extension and cord compression.
Figure 1: Left image - pre-operative coronal T1 post-contrast MRI showing bilateral dumbbell C2 tumour with intradural extension and cord compression.
Right image - pre-operative axial T1 MRI pre-contrast (top) and post-contrast (bottom) showing C2 ganglioneuroma with mild contrast enhancement and intradural extension.
View Figure 1
Neuromonitoring was utilized, with motor evoked potentials and free-running electromyography done as a baseline and then throughout the procedure. The patient was positioned prone in the Mayfield head clamp, with 3-point fixation. The head and neck were slightly flexed to expose the posterior cervical region. A midline incision from the inion to C4 was performed, and the fascia and muscle dissected off the midline. C1 and C2 were confirmed via x-ray localization, and laminectomies of both levels performed.
The operative microscope was then used to perform a durotomy and tenting of the dura to expose the spinal cord. The tumours at the C2 nerve roots were identified (Figure 2), and gentle sharp and blunt dissection performed to fully excise both tumours. No adverse events were detected by the neuromonitoring, which would have indicated compromise of the spinal cord during the operation. Watertight closure of the cal sac was performed with 4-0 monofilament suture, and dural matrix and sealant applied to help prevent CSF leaks.
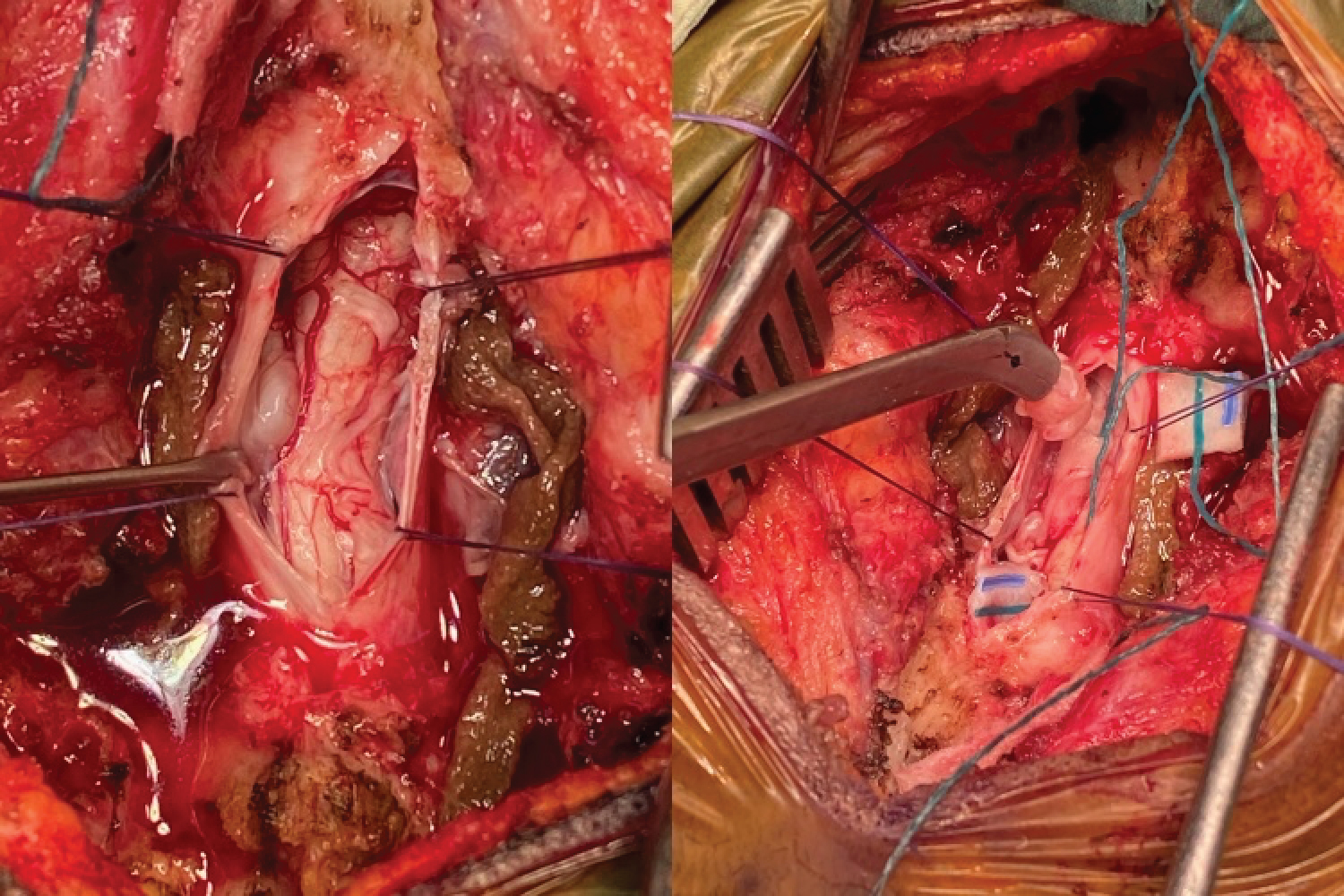 Figure 2: Intraoperative exposure of tumour at right C2 nerve root (left image) and removal of tumour (right image) after dissection. The depression on the cervical cord (left image) can be appreciated, where the left C2 tumour was, prior to excision.
View Figure 2
Figure 2: Intraoperative exposure of tumour at right C2 nerve root (left image) and removal of tumour (right image) after dissection. The depression on the cervical cord (left image) can be appreciated, where the left C2 tumour was, prior to excision.
View Figure 2
Controlled flexion-extension of the cervical spine was then performed under fluoroscopy, and there was no evidence of instability. Posterior C1-2 fusion was not required. Standard layered closure was done, and the patient was neurologically intact upon awakening.
Postoperative MRI revealed significant decompression of the spinal cord at the C1-2 level, and gross total resection of the tumours (Figure 3). Histological sections showed large neural bundles consisting of elongated wavy spindle cells within a fibrous background. Small clusters and single scattered ganglion cells were present within the lesion, consistent with a CGN.
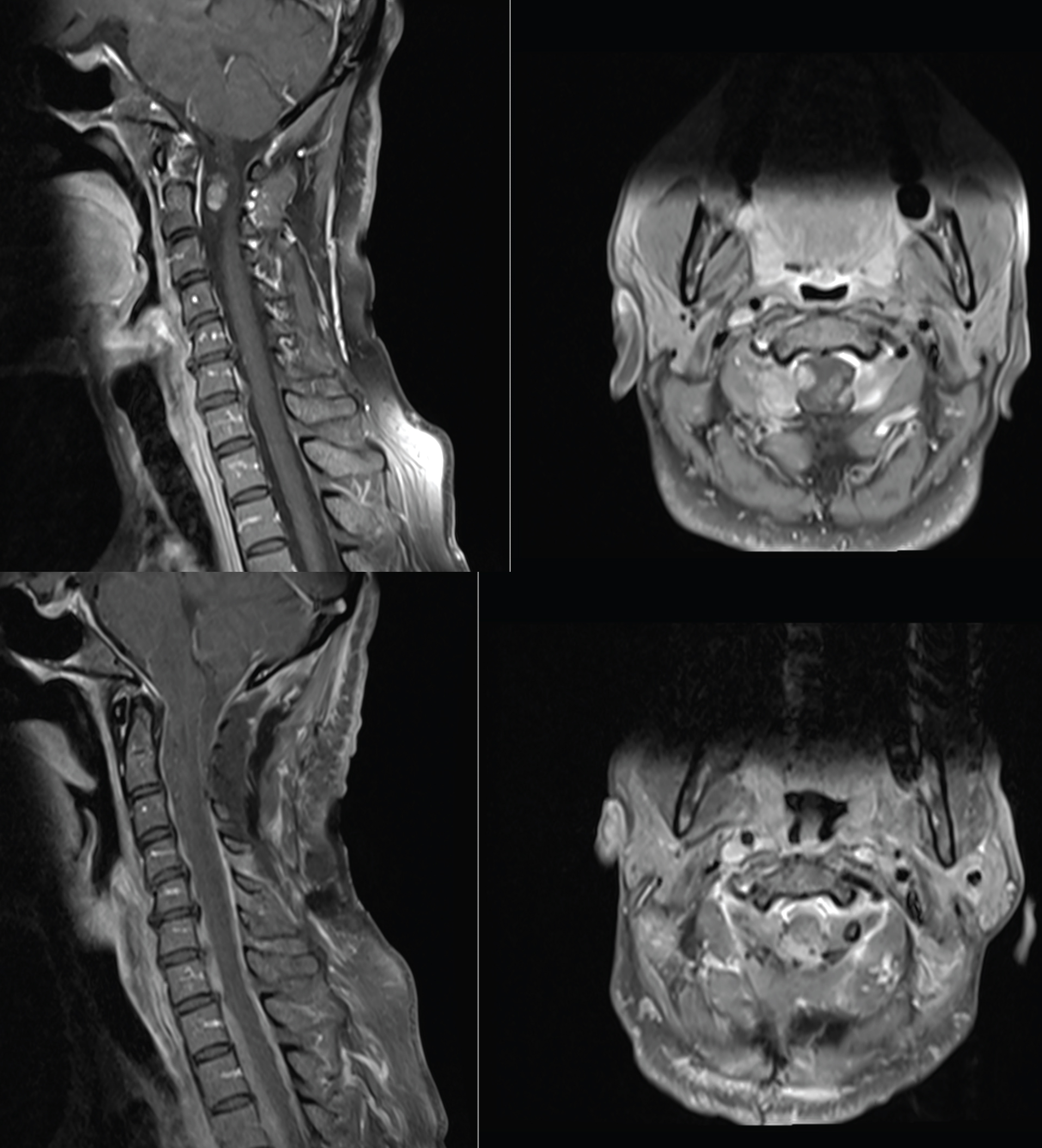 Figure 3: Preoperative (top row) and immediate postoperative (bottom row) T1 post-contrast MRI sagittal and axial images, showing degree of decompression and excision of dumbbell CGNs.
View Figure 3
Figure 3: Preoperative (top row) and immediate postoperative (bottom row) T1 post-contrast MRI sagittal and axial images, showing degree of decompression and excision of dumbbell CGNs.
View Figure 3
The patient had an uneventful postoperative course, with near complete resolution of her paresthesia. She was discharged after 3 days, and at 6-week follow-up she remains well.
Ganglioneuromas are benign tumours that arise from the sympathetic nervous system, mainly from the paraspinal sympathetic ganglia. These are among the spectrum of peripheral neuroblastic tumours, which are neuroblastoma and ganglioneuroblastoma (intermixed), ganglioneuroma and ganglioneuroblastoma (nodular) [1]. While they are typically seen in the posterior mediastinum and abdomen, they can rarely extend into the neural foramina and spinal canal [2]. Only 16 cases of CGN [3] have been documented the English literature.
Of the 16 reported cases of CGN, 6 were associated with NF1 [3-7]. NF1 is a genetic disorder with varying neurocutaneous manifestations, including a predisposition for tumours. It is caused by mutations in the NF1 tumour suppressor gene on chromosome 17q11, which encodes for the protein neurofibromin. This protein influences multiple signaling pathways, including negative regulation of cell growth and proliferation. The '2-hit' hypothesis of tumour formation in NF1 includes a germline mutation in the NF1 gene (first hit) and a somatic mutation (second hit) causing loss of heterozygosity in the gene [8]. This gives rise to neurofibromas, ganglioneuromas and other tumours.
CGN causes symptoms related to the degree of spinal canal invasion and cord compression. In the 6 cases of NF1-related CGN, tetraparesis was the most common symptom with respiratory and sensory dysfunction also present in some patients [7]. Ganglioneuromas of the cervical spine are found to be dumbbell shaped and have a higher rate of intradural extension [3].
In our patient, despite the degree of high cervical spinal cord compression and myelomalacia on MRI, she only complained of paresthesia of the upper limbs, and had brisk reflexes on examination.
MRI is the investigation of choice, once cervical myelopathy is suspected. Features associated with CGN are low signal intensity on T1-weighted images, high signal intensity on T2- weighted images. Mild contrast enhancement is typical. CT imaging with bony windows should be performed if fusion is deemed a possibility, to allow pre-operative planning and implant measurement.
Ganglioneuromas are Schwannian stroma-dominant and can be either maturing or mature. While there may be overlapping features between ganglioneuromas and ganglioneuroblastomas, the neuroblastomatous foci do not form distinct nests in ganglioneuromas. Individual neuroblastomatous cells merge into the mainly ganglioneuromatous stroma, with either maturing or mature ganglion cells [1].
Since their nature is typically benign, and they are encapsulated, primary treatment involves surgical resection of the lesion in entirety. Depending on the extent of the tumour and degree of exposure required, fusion may be a possibility. Post-operative chemotherapy or radiation is not usually recommended due to the mature nature of these lesions and their favorable prognosis [9]. Long-term surveillance should be considered, since a rare development of neuroblastoma 11 years after resection of a spinal ganglioneuroma has been recorded in the past [10].
CGN should be suspected in any patient with NF1 and evidence of cervical myelopathy. Their incidence is rare when compared to neurofibromas, and our patient is the 7th such case reported in the English literature. Management is primarily resection, as these tumours are benign. Malignant transformation, although rare, warrants long term surveillance in these patients.
All authors have contributed equally to the creation, drafting and editing of this manuscript. There were no sources of funding, and none of the authors have any financial disclosures.