Cerebral salt wasting, a rare complication of cranial neurosurgery, has not been reported after a functional pituitary tumor resection. The simultaneous presentation of diabetes insipidus (DI) and cerebral salt wasting after pituitary surgery presents a unique diagnostic challenge. We present a case of a 27 y.o. man with a 6-month history of acromegaly as evident by an IGF-1 of 1040 ng/mL (reference range: 101-307 ng/mL). MRI of the pituitary revealed a 3.2 cm × 3.2 cm × 3.1 cm macroadenoma extending beyond the sella turcica. He underwent image guided transsphenoidal pituitary resection. Post-operatively, he developed triphasic diabetes insipidus. However, 5 days after surgery, urine osmolality and Na concentrations were increasing, despite worsening hyponatremia. While hyponatremia could be misdiagnosed as concurrent syndrome of inappropriate antidiuretic hormone (SIADH), persistent natriuresis is indicative of cerebral salt wasting syndrome (CSWS). Therapeutic goals for these patients are to replace lost sodium and prevent further natriuresis. Treatment with hypertonic saline and fludrocortisone were successful. At three month follow up, the patient's serum osmolarity remained normal and fludrocortisone was discontinued. Here the clinical importance and potential diagnostic methods of differentiating SIADH and CSWS in the critical care setting are reviewed.
Cerebral salt wasting syndrome, Hyponatremia, Acromegaly, Transsphenoidal pituitary resection
Post-operative care for neurosurgical patients requires extensive monitoring for early detection and treatment of complications. Sodium homeostasis is particularly challenging, as there are a myriad of postoperative syndromes involving sodium disturbances. Potential causes of hyponatremia in neurosurgical patients are numerous, SIADH being the most common [1]. More rarely, it can be caused by cerebral salt wasting syndrome (CSWS), a distinct clinical entity from SIADH for which the treatment is different [1]. If CSWS is misdiagnosed as SIADH and fluid restriction is subsequently ordered, the electrolyte imbalances of CSWS could worsen and lead to further damage to the nervous system. This puts the patient at risk for severe sequelae, making clinical distinction of these two entities in neurosurgical patients paramount. However, this can be challenging as both can present with similar laboratory findings, such as elevated urine sodium concentration. Presented here is a case of CSWS which is being reported for the first time after a transsphenoidal surgery for a growth hormone secreting macroadenoma.
A 27-year-old man presented to his primary care physician with complaint of 40 pounds of weight gain over 6 months, severe headaches, fatigue, excessive hunger with nocturnal wakening to eat, along with increasing shoe, tongue and hand size. Laboratory work up showed: IGF-1 of 1132 ng/mL (reference range: 101-307 ng/mL) and elevated fasting insulin of 47.0 mU/L (reference range: 3.0-25.0 mU/L), with concomitant fasting glucose of 119 mg/d (reference range: 65-99 mg/dL). MRI of the head revealed a macroadenoma measuring 3.2 cm × 3.2 cm × 3.1 cm extending beyond the sella turcica, encroaching on the optic chiasm, and invading the left cavernous sinus. Based on these findings the patient was diagnosed with acromegaly.
The patient was referred to neurosurgery for evaluation. Visual field testing revealed bitemporal hemianopsia. Based on the observed chiasmatic involvement and cavernous sinus invasion, surgical debulking was recommended. An image guided endoscopic transnasal resection of the tumor with abdominal fat pad graft harvest was performed.
The following day, the patient reported peripheral vision loss in the left eye that progressively worsened overnight and transsphenoidal endoscopic image guided exploration of the sella was performed on postoperative day 3 after the initial resection. A hematoma was evacuated and additional tumor was removed. Visual disturbances improved after the second procedure and further neurosurgical intervention was not required.
On postoperative day 1 after the initial transsphenoidal tumor resection he had dilute urine (129 Osm) and high urine output (4.5 mL.kg/hr) and the lost volume was replaced with IV fluids. He received desmopressin (DDAVP) three times. Urine osmolarity remained above 150 Osm after administration of DDAVP and no further doses were given, as serum sodium and urinary osmolarity had remained normal for several days.
On postoperative day 5 after the initial resection, his serum sodium dropped from 142 mmol/L to 126 mmol/L (reference range: 136-145 mmol) and his urine osmolarity was greater than 500 Osm, which the team diagnosed as SIADH. Consequently, fluid restriction to 1 L for 24 hours was ordered. The next day, hyponatremia persisted and hypertonic saline was administered; however, serum sodium levels continued to drop overnight. On postoperative day 6 after the initial resection, CSWS was diagnosed based on high urine osmolarity (716 Osm on day 6), continued high urine output, and urine sodium concentration of 240 mEq/L. These values represent a disproportionate amount of urine sodium as compared to sodium intake. Fludrocortisone 0.1 mg once daily was added at this time to restrict further renal salt wasting. Hypertonic saline was continued as hyponatremia persisted.
On postoperative day 9 after the initial resection, sodium was improving slowly and hydrocortisone 25 mg three times daily was added to enhance the mineralocorticoid effects of fludrocortisone and induce renal sodium and volume retention. At the time of discharge, postoperative day 10 after the initial resection, serum sodium had normalized to 138 mmol/L and he was otherwise stable. Hydrocortisone and fludrocortisone were both continued outpatient and on postoperative day 18 after the initial resection, he reported a normalized appetite but still experienced subjective polyuria.
At follow-up with endocrinology 2 months postoperatively, the patient's urine sodium and serum electrolytes had remained normal with regular checks since discharge. Fludrocortisone was discontinued, and he reported no further increased thirst or polyuria. He remained asymptomatic with normal serum electrolytes.
The incidence of CSWS after cranial neurosurgery has been reported to be between 0.8% and 34.6% of patients [1]. However, it is clear that CSWS is a rarer cause of hyponatremia than SIADH and is less likely to be considered by the physicians supervising the patient's recovery.
CSWS was first described in the literature in 1950 as a complication of brain disease and not necessarily cranial neurosurgery [2]. It is characterized as a condition of pathological natriuresis and volume depletion at the level of the kidney [2]. The most common brain disturbance that results in this particular syndrome is subarachnoid hemorrhage after cerebral aneurysm rupture [2]. Trauma and surgery remain less common causes of this presentation [3]. The mechanism for this disorder's disruption of sodium balance has yet to be fully elucidated, however several theories have been proposed. Some examples include interrupted sympathetic output to the kidney from the nervous system resulting in less renin-angiotensin-aldosterone system (RAAS) activation or increased natriuresis as a result of the release of an unknown natriuretic peptide that opposes the RAAS [4]. Some studies have cited excessive release of brain natriuretic peptide (BNP) and human atrial natriuretic peptide (hANP) as possible mediators of CSWS pathophysiology [5]. These peptides, when released by various tissues into the blood, act against the pressures of the RAAS system and oppose salt retention and facilitate loss of sodium in the urine at the level of the nephron [6].
CSWS differs from SIADH in terms of its clinical findings in that it includes volume depletion [7]. CSWS involves loss of sodium and fluid at the level of the kidney after a traumatic event involving the brain [7]. Conversely, SIADH involves retention of water alone at the level of the collecting duct of the nephron with normal excretion of sodium, resulting in a dilutional hyponatremia [8]. SIADH does not involve a loss of sodium, meaning the volume status of the patient remains euvolemic, whereas CSWS involves natriuresis and hypovolemia [7,8]. The mechanism for SIADH involves excessive and inappropriate secretion of antidiuretic hormone (ADH), also called arginine vasopressin, from the posterior pituitary into the blood, causing alteration in nephron function by binding to the vasopressin-2 (V2) receptor and increasing the number of aquaporins present in the cells of the collecting duct thereby increasing the retention of water [8]. As a result of the etiology and volume status, fluid restriction and administration of vaptan drugs, which antagonize the V2 receptor and prevent water retention, are key parts of the treatment of SIADH in an effort to reverse dilutional hyponatremia [7]. Such interventions in a patient with CSWS, who is already volume depleted, would further worsen their volume status and put the patient at greater risk for complications [1]. Consequences of this misdiagnosis could include seizure, cerebral edema, or worsening of vasospastic ischemia secondary to cerebral bleeding from trauma or surgery [4,7].
In terms of differentiation of these conditions, it can be difficult based only on clinical laboratory findings. Both conditions will have blood hypo-osmolarity, hyponatremia, high urine specific gravity, and high urine sodium content [9]. Further, ADH levels are unreliable [9,10]. While SIADH will have high serum ADH levels from unprovoked release, in CSWS there is resultant hypovolemia which will be sensed by baroreceptors in the carotid body and lead to stimulation of ADH release from the pituitary, so both conditions could have elevations in ADH [9]. Perhaps there lies a difference in the degree of ADH increase, with more substantial increases likely attributable to SIADH, but such a quantitative analysis has yet to be reported in the literature.
In this patient, nephrology and endocrinology made the diagnosis of CSWS by monitoring the response of the patient's urine sodium and serum sodium to fluid restriction. As is shown in Table 1, fluid restriction initiated on post-operative day 5 did not improve serum sodium levels on Day 6 and in fact sodium continued to trend downward. This indicated that water retention alone was unlikely the cause of hyponatremia and that there must be an additional component of active sodium loss in the urine. Response to fluid restriction has been cited in several studies as a major method of differentiating SIADH and CSWS [5]. However, restriction of fluids during the course of CSWS can worsen clinical picture and puts the patient in danger of the aforementioned complications, so using this as a tool for detection of CSWS may not be ideal.
Other methods of detection may include monitoring the fractional excretion of urinary ions. For example, since CSWS includes pathological naturesis despite hyponatremia, the fractional excretion of sodium (FeNa) in such patients will be far higher than expected for a person who is hyponatremic (higher than 2%) [11]. In contrast, in the setting of SIADH FeNA usually remains below 0.5% as the kidneys maintain euvolemia through sodium retention [12]. Other studies cited increased levels of the fractional excretion of uric acid (FeUA) as tools for monitoring CSWS, as ADH release increases uric acid retention to act as an osmotic draw for water [9,13]. As such, if SIADH is the underlying cause, FeUA has been observed to be lower than in CSWS patients.
Further, the main clinical difference between the two conditions lies in volume status, but this can be a difficult aspect of the patient presentation to assess. Factors such as blood pressure, and the presence or absence of orthostatic hypotension can be used, but are insufficient on their own [9]. Inferior vena cava diameter measurement by ultrasound can be used to assess volume status since a IVC diameter of less than 15 mm indicates hypovolemia in most adult patients [9].
Treatment for CSWS requires repletion of sodium and fluids with isotonic or hypertonic saline, depending on the degree of hyponatremia, and the addition of fludrocortisone, a synthetic mineralocorticoid that induces sodium retention, reduces natriuresis, and improves fluid volume [2,4]. In patients where fludrocortisone may not replete sodium levels on its own, glucocorticoid co-administration can act to augment fludrocortisone's effectiveness. In the patient presented, hydrocortisone was added for a time as an adjunct to his dosage of fludrocortisone. This was successful in opposing natriuresis and normalizing serum sodium levels.
In conclusion, we present the first case in the literature of CSWS after resection of a functional adenoma. We recommend measurement of FeNa or inferior vena cava diameter in all patients who are recovering from cranial neurosurgery, cerebrovascular events or TBI who also have hyponatremia to differentiate CSWS and SIADH. Urine sodium was not measured in this patient on days 6 and 7 when it may have been helpful to rule out SIADH and possibly have spared the patient a day of fluid restriction. While sensitivity and specificity studies for these factors in terms of detection of CSWS have yet to be done, they may help guide the clinician to make more appropriate management decisions in such patients and protect those with CSWS from preventable adverse outcomes (Figure 1 and Table 1).
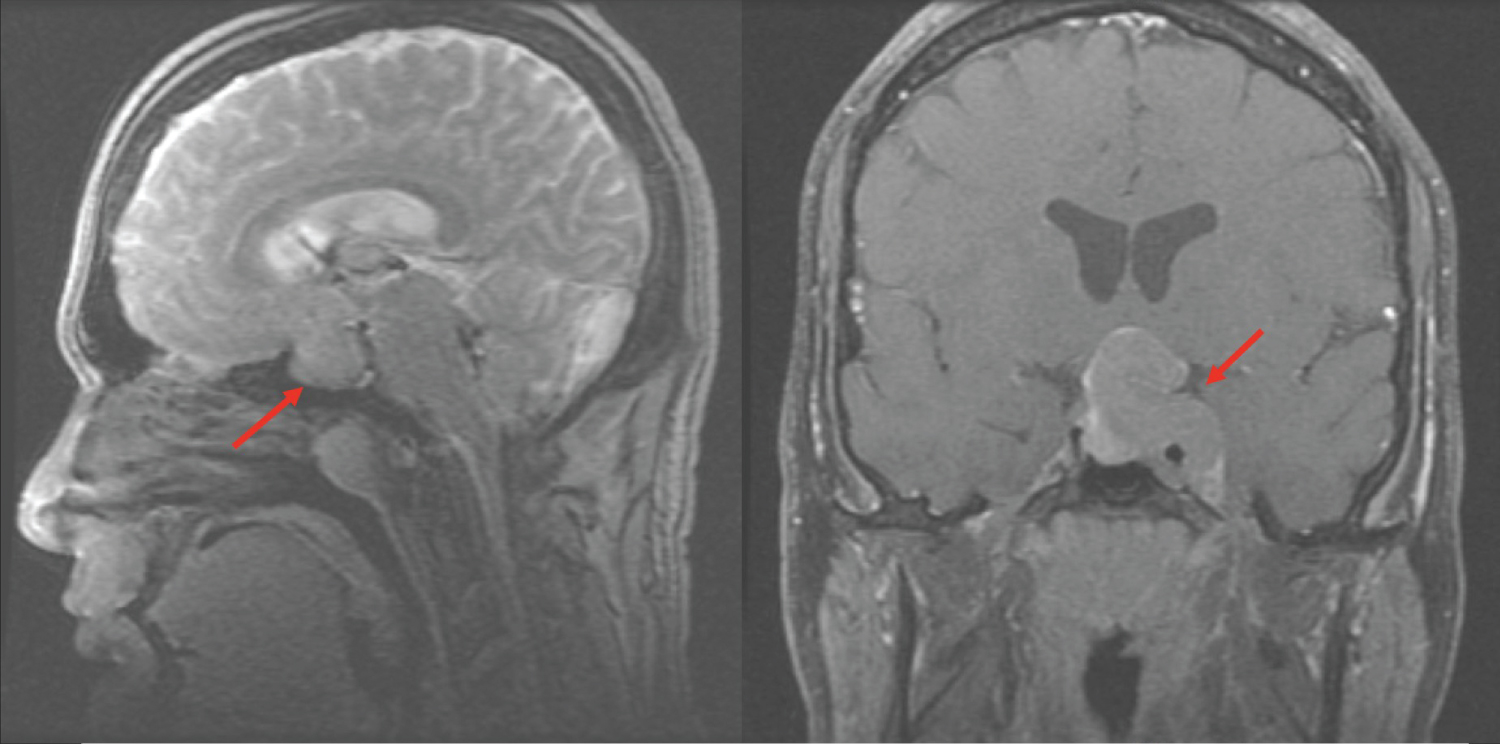 Figure 1: CT of the Head, sagittal and coronal sections. Here a CT of the head reveals a 3.2 cm × 3.2 cm × 3.1 cm macroadenoma extending beyond the sella turcica with encroachment on the optic chiasm.
View Figure 1
Figure 1: CT of the Head, sagittal and coronal sections. Here a CT of the head reveals a 3.2 cm × 3.2 cm × 3.1 cm macroadenoma extending beyond the sella turcica with encroachment on the optic chiasm.
View Figure 1
Table 1: Density grades in male group. View Table 1
We would like to thank St. Luke's University Health Network and the Lewis Katz School of Medicine at Temple University for their support in our research. We would also like to thank the patient for his permission to publish these findings.