Background: Coil migration is a rare but devastating endovascular complication that can lead to severe neurological deficit. There are only 11 cases reported in the literature, with the majority located within the middle and anterior cerebral arteries.
Objective: The objective of this article is to describe our experience in the management of an unusual case of a cerebral aneurysm with distal coil migration.
Methods: We describe the management of an unusual case of a cerebral aneurysm with distal coil migration. A 57-year-old female diagnosed with a right M2 middle cerebral artery saccular aneurysm (Fisher 4 Hunt and Hess 2) underwent endovascular treatment with coils. Post-operative imaging displayed coil migration to the right parietal level towards the ipsilateral angular artery.
Results: Subsequent surgical intervention of the aneurysm and conservative management for the migrated coils was determined. The procedure was well tolerated and the patient underwent a favorable evolution without neurological deficit or associated ischemic event.
Conclusion: Coil migration is an unusual but possible complication, requiring an individualized case-based approach for the best possible outcome in favor of the patient's well-being. We suggest an individual case-based interdisciplinary approachfor optimal management of this complication.
Aneurysm, Coils, Endovascular, Migration
Endovascular techniques for the treatment of cerebral aneurysms have increased by virtue of the technological progress of coils, stents and catheters. However, they are by no means a risk-free procedure. [1,2]. These techniques present a complication rate of 10-19%, with coil migration corresponding to 0.5-3%, [1,3,4] one of the most feared events due to its potential to produce severe neurological deficits [5].
Currently there are only 11 cases of coil migration reported in the literature, with the majority located within the middle and anterior cerebral arteries [3]. This complication can occur in an early or late fashion and present clinically from asymptomatic extending to severe neurological deficit. [6].
Considering its infrequency, a standardized treatment protocol for its resolution has not yet been established; surgical, endovascular and conservative management are potential options and must be individualized to each case [3,4].
Based on these considerations, the objective of this article is to describe our experience in the management of an unusual case of a cerebral aneurysm with distal coil migration.
We describe the management of an unusual case of a cerebral aneurysm with distal coil migration. A 57-year-old female diagnosed with a right M2 middle cerebral artery saccular aneurysm (Fisher 4 Hunt and Hess 2) underwent endovascular treatment with coils. Post-operative imaging displayed coil migration to the right parietal level towards the ipsilateral angular artery. The patient gave their consent to the procedure and consented to publication of surgical images. The ethics committee of our institution approved the publication of the reported case.
A cerebral computed tomography (CT) was performed revealing subarachnoid hemorrhage (SAH) with predominance within the sylvian cisterns and an associated intraventricular hemorrhage (Fisher 4, Hunt and Hess 2) (Figure 1A).
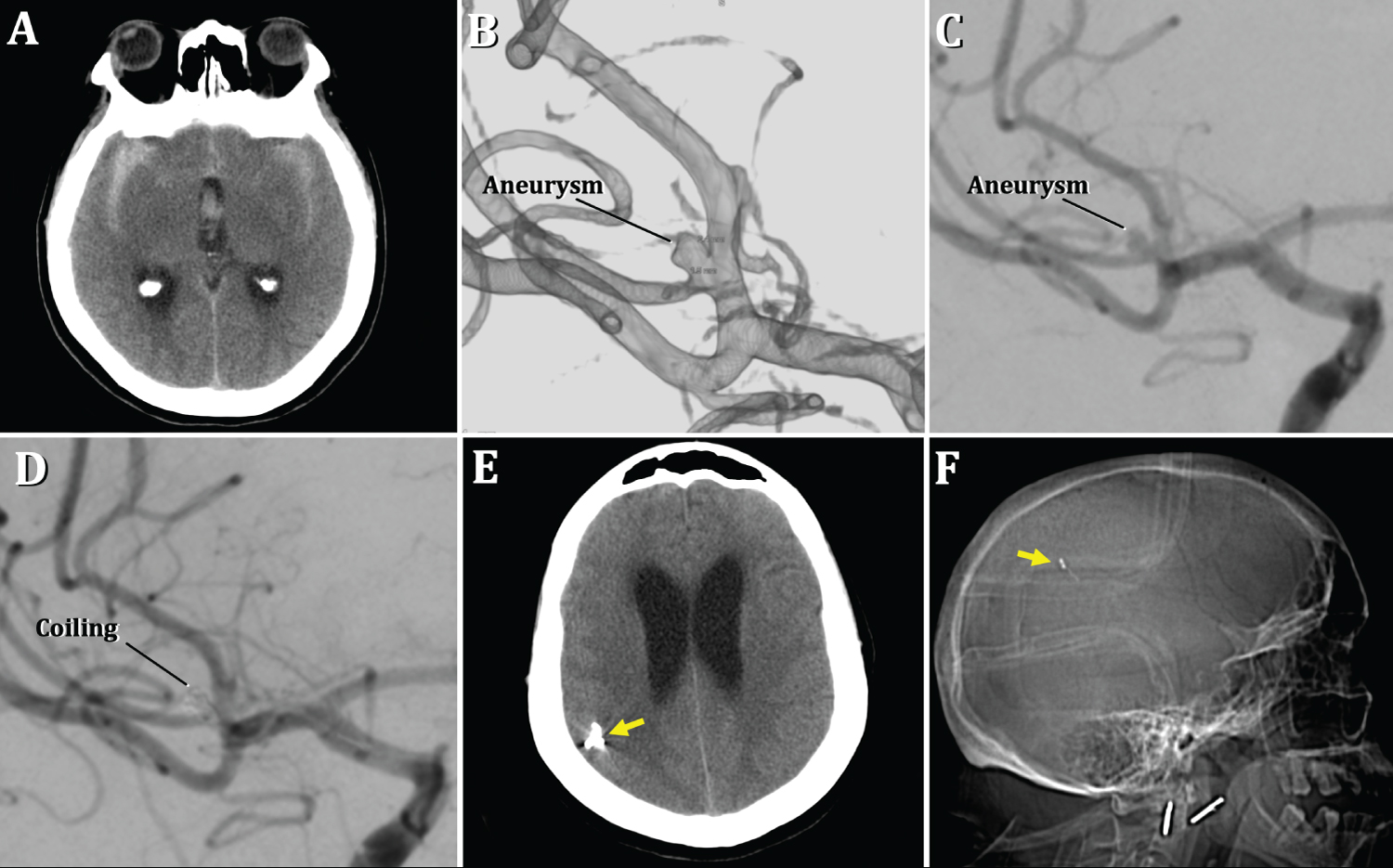 Figure 1: A, B, C) Pre-embolization images. A) Axial projection of cerebral CT scan showing SAH within the sylvian cisterns and interhemispheric fissure, associated with hemorrhage within the third ventricle, Fisher grade 4. B), C) Digital cerebral angiography with 3D reconstruction showing an aneurysm at the bifurcation of the right M2 superior branch, measuring 2.4 mm × 2.3 mm.
Figure 1: A, B, C) Pre-embolization images. A) Axial projection of cerebral CT scan showing SAH within the sylvian cisterns and interhemispheric fissure, associated with hemorrhage within the third ventricle, Fisher grade 4. B), C) Digital cerebral angiography with 3D reconstruction showing an aneurysm at the bifurcation of the right M2 superior branch, measuring 2.4 mm × 2.3 mm.
D), E) F) Post-embolization images. D) Digital cerebral angiography displaying coils within the aneurysmal sac. E), F) Control brain CT with scout view; F) Showing distal coil migration to the right parietal region (yellow arrow).
View Figure 1
Digital cerebral angiography showed a saccular aneurysm located at the bifurcation of the upper branch of the M2 segment of the right middle cerebral artery, measuring approximately 2.4 mm × 2.3 mm (Figure 1B and Figure 1C). Initially, the endovascular team opted for treatment with coils. The procedure was well tolerated and the patient underwent a favorable evolution without neurological deficit. Initial post-op angiography confirmed correct coil placement and aneurysmal occlusion (Figure 1D). She subsequently initiated antiplatelet and anticoagulant treatment.
On the second day post-embolization, a CT scan was performed showing coil migration to the right parietal level (Figure 1E and Figure 1F). A cerebral angiography was repeated and revealed persistence of the right M2 segment aneurysm and distal migration of the coils towards the ipsilateral angular artery. Regional preservation of blood flow was also noted.
The case was assessed in conjunction with the endovascular and vascular neurosurgical department, deciding surgical intervention of the aneurysm and conservative management for the migrated coils. This was determined based on the small diameter of the affected vessel, its adequate vascular permeability and the patient's asymptomatic presentation without an associated ischemic event.
Under general anesthesia, a right pterional craniotomy was performed with a subsequent durotomy and exposure of the sylvian fissure. Over a tense and swollen brain, abundant SAH was observed over the convexity and within the sylvian cisterns. With delicate microsurgical dissection, the lamina terminalis was opened, allowing cerebral relaxation and distal to proximal dissection of the fissure. Exposure and 360º dissection of the small aneurysmal sac located at the bifurcation of the upper branch of M2 was achieved (Figure 2A). A 5 mm curved miniclip was applied for occlusion (Figure 2B and Figure 2C). Adequate vascular patency of both the upper and lower branches of M2 were verified with microvascular doppler ultrasonography. The patient tolerated the intervention and was admitted to the Intensive Care Unit without neurological deficit.
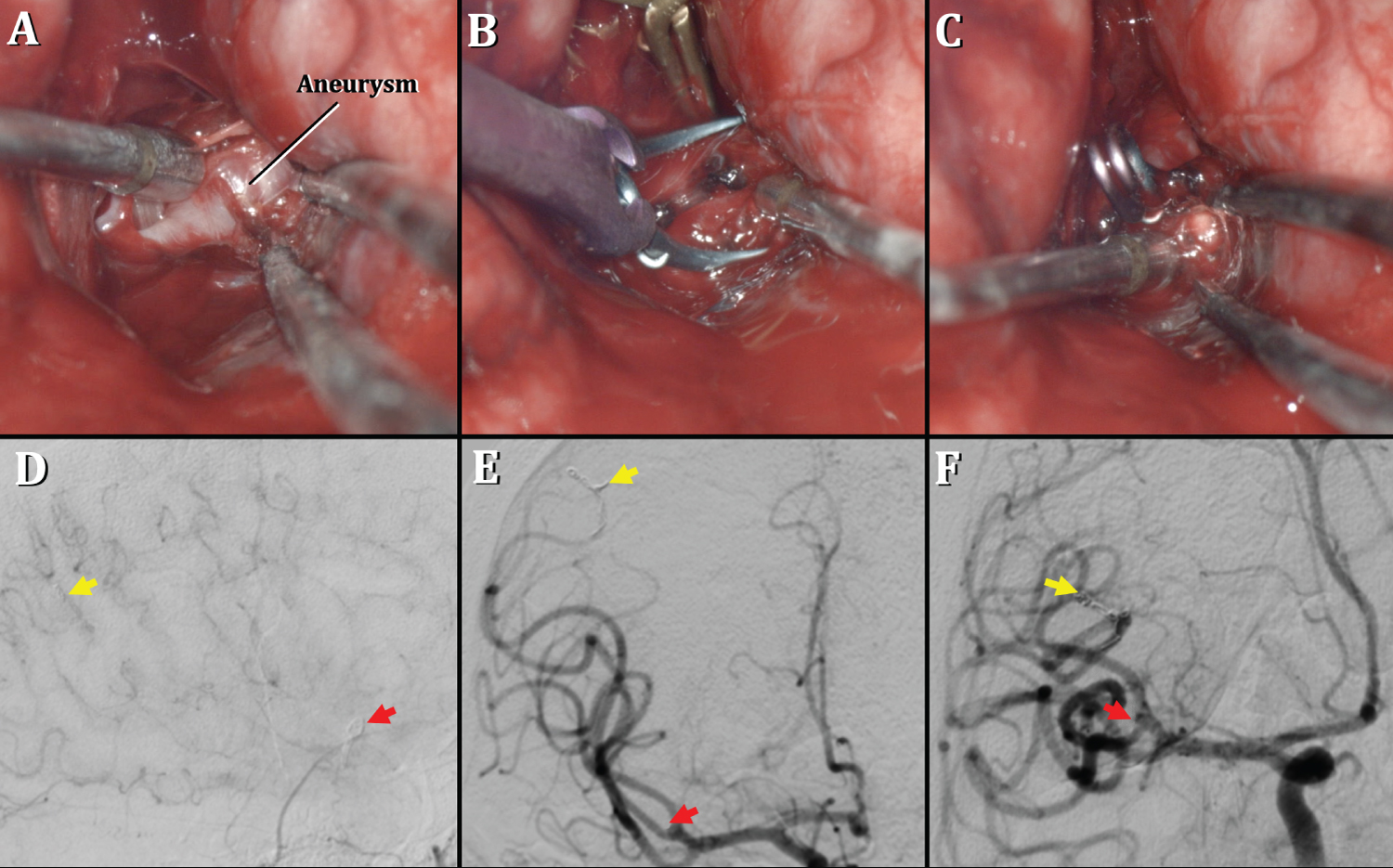 Figure 2: A), B), C) Intraoperative images. A) Exposure of the aneurysmal sac and placement of a temporary clip in the upper branch of M2; B) Placement of a 5 mm curved mini clip; C) Removal of the temporary clip and correct placement of the permanent clip is verified, achieving visualization of both free M2 branches.
Figure 2: A), B), C) Intraoperative images. A) Exposure of the aneurysmal sac and placement of a temporary clip in the upper branch of M2; B) Placement of a 5 mm curved mini clip; C) Removal of the temporary clip and correct placement of the permanent clip is verified, achieving visualization of both free M2 branches.
D), E), F) Post-clipping digital cerebral angiography. D) Lateral projection displaying the location of the aneurysm clip in relation to the bifurcation of the upper branch of M2 (red arrow) and migrated coils in the right angular artery (yellow arrow). E), F) Anteroposterior projection showing absence of residual aneurysmal sac (red arrow) and persistence of distally migrated coils (yellow arrow).
View Figure 2
Post-op control angiography showed correct clip placement without exposed aneurysmal sac or residual neck, and adequate permeability of the M2 segment and right angular arterydespite persistence of the migrated coils (Figure 2D, Figure 2E and Figure 2F). Given the favorable evolution, the patient was discharged with antiplatelet therapy, Rivaroxaban at a dose of 15 mg/day was selected.
Coil migration is a very rare complication of endovascular treatment, representing 0.5%-3% in a series by Gatto, et al. of 403 patients with embolized ruptured cerebral aneurysms [6]. Other reported complications include arterial perforation (2.3%-4.7%), thromboembolism (2.5%-14.5%) and main artery occlusion (2%-3%). Most occur at the intracerebral level, however authors such as Shaikh, et al. have described an even more exceptional case of migration towards the peripheral circulation, specifically to the popliteal artery [1].
There are multiple causes that could explain coil migration. Banerjee claims that this generally occurs when the neck-sac ratio is unfavorable, [7] as can be seen in the case of Fiorella, et al., describing a small aneurysm measuring 4.5 mm × 4.4 mm × 3.9 mm (mean 2.5mm) [8] as well as wide neck aneurysms such as one presented by Gao, et al. [9]. Others attribute the endovascular technique itself as the cause, either due to intrinsic coil properties (shape, location, size and instability) or insufficient packing [3,10].
On the other hand, coil migration has been associated with the interruption of anticoagulation in a series of patients presented by Gao, et al. [9]. Along these lines, Tomoya emphasizes the important but questionable role that antithrombotic agents play in delaying migration, fundamentally with the use of Rivaroxaban at a dose of 15 mg/day [3].
There are several aspects of this complication yet to be defined, among these is time of intervention [4]. Some ensued removal in the immediate period of migration, [2] while others intervened days or even months posterior to the event, [7,10] without obtaining significant or conclusive differences. Standard method of treatment is also uncertain. Hajime, et al. propose clipping in combination with coil removal by arteriotomy. However, the authors highlighted that removal was not always feasible and possibly counterproductive due to endothelial proliferation and inflammation of the arterial wall [3,4,10]. Zhi, et al. achieved therapeutic success of transcranial extraction of coils with migration towards the carotid bifurcation and M1 segment, acknowledging an increased risk of stenosis and post-arteriotomy occlusion in patients with vasospasm secondary to SAH [5]. Another valid alternative is endovascular intervention, albeit in the same way as arteriotomy, it is not always possible considering risk of distal coil displacement [5]. Conservative management is accepted primarily in cases of asymptomatic migration without an ischemic event and with adequate blood flow within the affected vessel [4,6,9].
Coil migration is an unusual but possible complication, requiring an individualized case-based approach for the best possible outcome in favor of the patient's well-being. The proposed alternatives present both risks and benefits to a greater or lesser extent, which is why we suggest studying each case in detail and in an interdisciplinary manner with a neurovascular, endovascular and neuroanesthesia team, expanding the range of therapeutical options.
In our particular case, clipping of the aneurysm with conservative management of the migrated coil allowed a favorable anddefinitiveoutcome without associated complications, which we hope will contribute to the experiences previously published.
The authors report no conflict of interest concerning the materials or methods used in this study of the findings specified in this paper. We confirm that the manuscript has been read and approved by all named authors and that there are no other persons who satisfied the criteria for authorship but are not listed. We further confirm that the order of authors listed in the manuscript has been approved by all of us. We confirm that we have given due consideration to the protection of intellectual property associated with this work and that there are no impediments to publication. We understand that the Corresponding Author is the sole contact for the Editorial process (including Editorial Manager and direct communications with the office). I am responsible for communicating with the other authors about progress, submissions of revisions and final approval of proofs. We confirm that we have provided a current, correct email address which is accessible by the Corresponding Author.
None
The patient gave their consent to the procedure and consented to publication of surgical images.