Fat embolism syndrome (FES) is defined as the presence of fat particles (i.e., > 100 particles per mm2) in the blood circulation that result in symptoms and/or organ failure. FES could result from mechanical causes, trauma or sepsis and, even if very rare, is a fatal disease that develops within 12-72 hours. FES manifestations can vary from mild cognitive changes to coma and even cerebral edema and brain death. The exact incidence of FES stemming from traumatic long bone injuries varies in literature, from 0.9% when clinical criteria are used for diagnosis to 29% in post-mortem autopsies [1]. Cerebral fat embolism (CFE) has been described in about 10% of FES cases based on clinical criteria, but the true incidence is also unclear due to the absence of definitive diagnostic testing [2]. We present a case of isolated CFR with no intracardiac shunt or pulmonary dysfunction in a polytrauma patient of 20-years-old.
A 20-years-old male was admitted to our emergency department for a road car accident with a diagnosis of bilateral lower extremities fractures (tibial shaft fracture and femoral neck fracture. After six hours he underwent a surgical intervention of endomedullary nailing for both fractures (Figure 1). Before surgery, this patient was conscious at all times but 24 hours after surgery, he manifested state of confusion, with episodes characterized by delusional ideation, confabulation and psychomotor agitation. On neurological physical examination, the patient was alert, disoriented in time, cranial nerves appeared uninjured, and there were no focal limb signs. Brain CT scan and electroencephalogram showed no abnormalities. Due to the persistence of the symptomatology, MRI of the brain was performed, which showed multiple, millimeter-long areolae of pathological signal restriction in DWI study sequences at the bilateral nucleocapsular region, corona radiata, deep white matter and juxtacortical on both sides as well as at the posterior frontal cortical site. Additional similar areas were found at the posterior median and paramedian right commissural region and at bilateral retro trigonal site. These findings were compatible with multiple embolic-based ischemic foci in an evolving phase (Figure 2). There is no specific treatment for fat embolism or fat embolism syndrome. Therapy included prophylaxis stroke with aspirin at a daily dose of 100 mg, Low Molecular Weight Heparin (LMWH) 4000 IU once day and Dexamethasone 4 mg intravenous twice daily. After one day, the patient appeared markedly improved, alert, conscious and cooperative, oriented in time, with fluent speech, normal pupillary reflex, preserved strength, sensitivity and coordination, absent meningeal symptoms. The patient during hospitalization practiced echocardiographic "bubble-test" with evidence of suspected atrial septal defects (ASDs) at the level of the caval septum with left-to-right shunt and passage of microbubbles of moderate entity. Transesophageal echocardiography could not be performed because of the patient's difficulty in lying lateral decubitus. After 10 days, the patient repeated brain MRI that showed attenuation of known ischemic lesions (Figure 3).
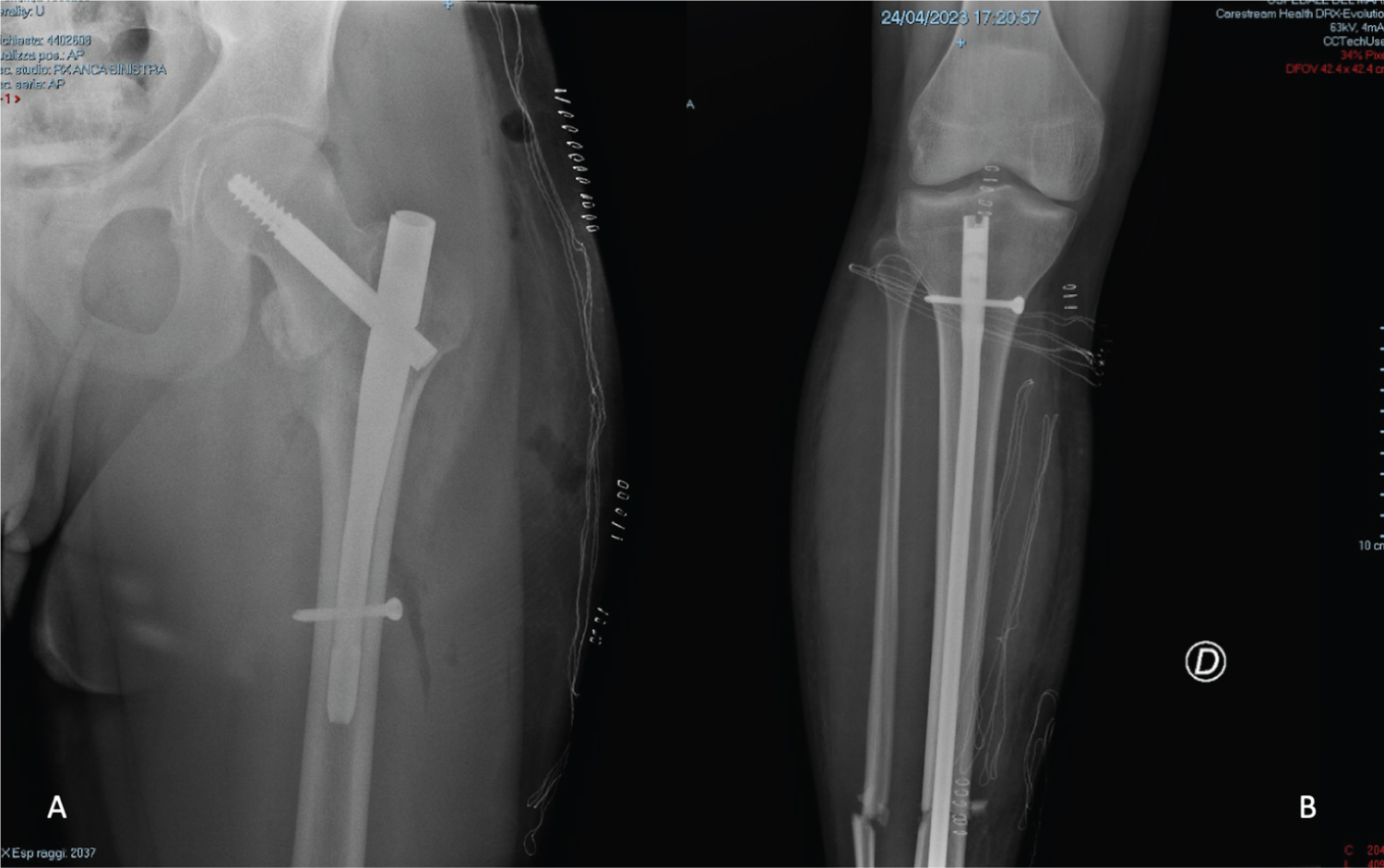 Figure 1: Post-operative X-Ray.
View Figure 1
Figure 1: Post-operative X-Ray.
View Figure 1
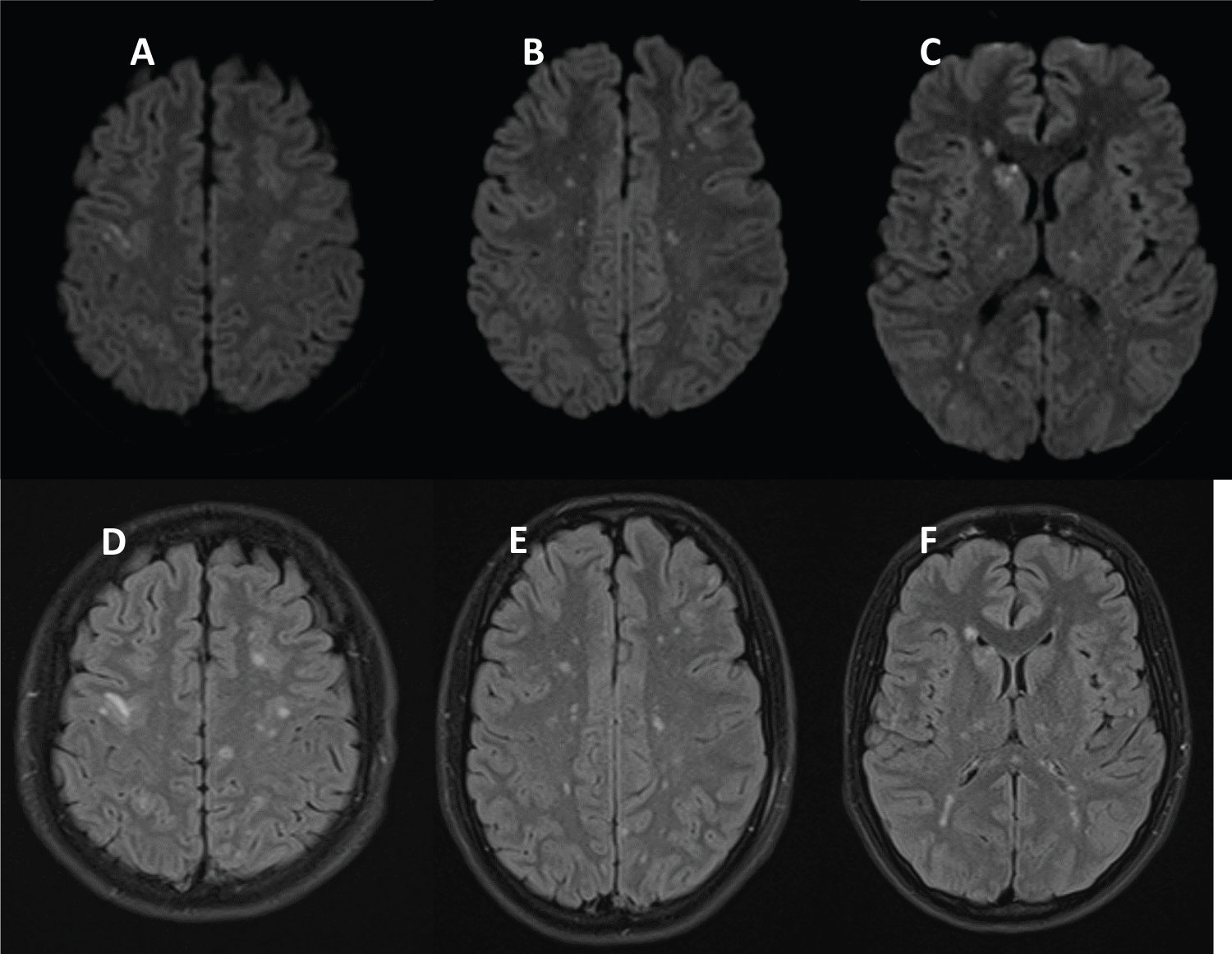 Figure 2: These foci are associated with parenchymal T2/FLAIR hyperintensities (D-E-F) and diffusion restriction (A-B-C), in particular along the hemisphere subcortical, periventricular white matter and bilateral nucleocapsular region. This imaging shows a "starfield pattern", the result of very numerous microemboli.
View Figure 2
Figure 2: These foci are associated with parenchymal T2/FLAIR hyperintensities (D-E-F) and diffusion restriction (A-B-C), in particular along the hemisphere subcortical, periventricular white matter and bilateral nucleocapsular region. This imaging shows a "starfield pattern", the result of very numerous microemboli.
View Figure 2
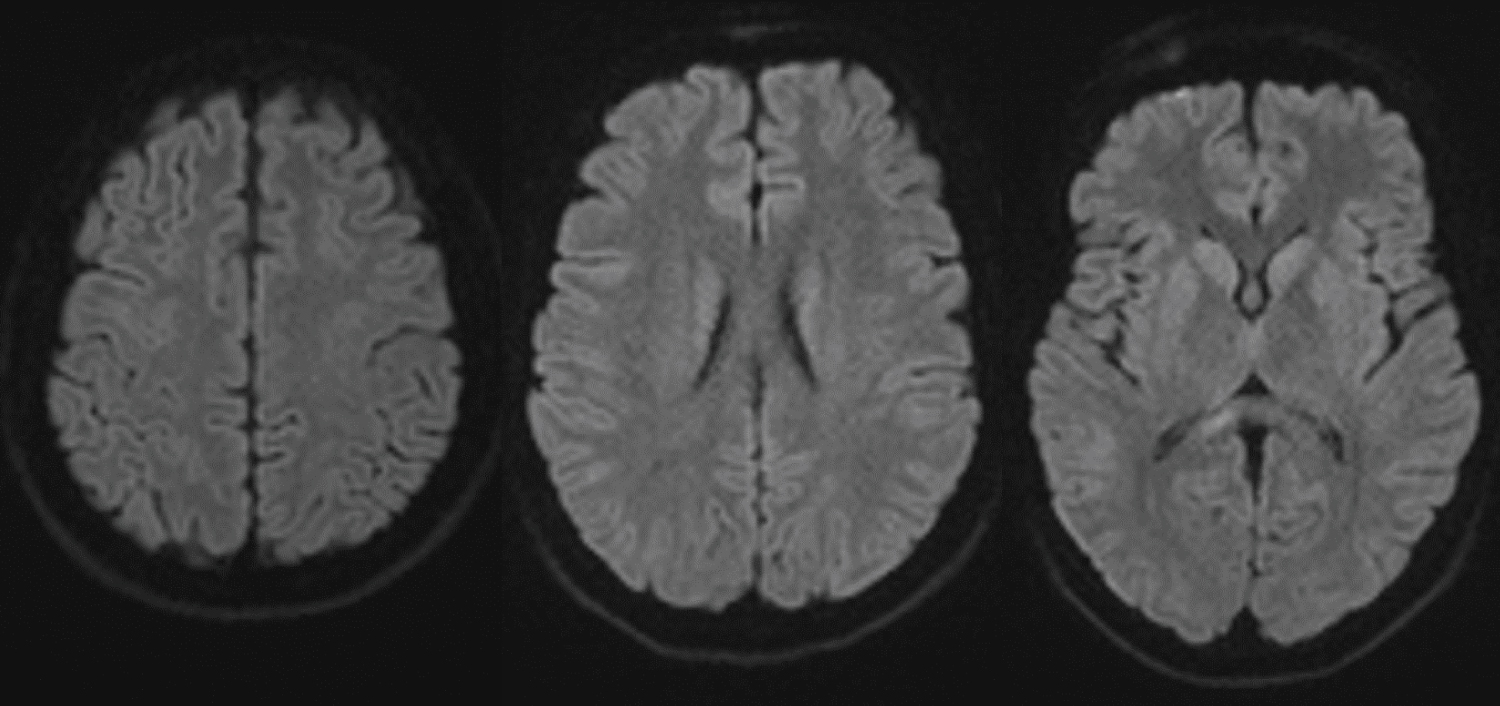 Figure 3: MRI FLAIR imaging after 10 days: Improvement of hyperintensity of known cerebral lesions.
View Figure 3
Figure 3: MRI FLAIR imaging after 10 days: Improvement of hyperintensity of known cerebral lesions.
View Figure 3
Fat embolism syndrome is a clinical diagnosis and is caused by the release of fat droplets into the systemic circulation after conditions or procedures such as long bone or pelvic fractures, orthopedic surgery or other interventions [1-5]. The pathophysiology of FES in unknows, but different mechanisms have been suggested [6]. The mechanical mechanism suggest that physical obstruction of the vascular system occurs, caused by fat globules released from the bone marrow of long bones due to the increased intramedullary pressure after trauma or orthopedic surgery (such as intramedullary nailing) [7,8]. The biochemical theory suggests liberation of free fatty acids after a local inflammatory response at the site(s) of fat emboli deposition, with a surge of catecholamines as a stress response to microtrauma of the affected capillary bed. These fatty acids interacts with lung lipases, leading to the activation of the intrinsic apoptosis cascade and subsequent damage to both lung parenchyma and capillary endothelium, with the development of an interstitial hemorrhages and edema [7,9,10]. The role of a PFO is not crucial in developing a lung fat embolism into a systemic embolism: The fat embolism is more of a biochemical and pathophysiological event, than a biomechanical one. The appearance of a patent foramen ovale associated with a systemic fat embolism should be less emphasized: Maybe arteriovenous shunts and anastomosis between the functional and nutritive, i.e. systemic circulation of lungs play a more important role in developing a SFE than a PFO [11]. The diagnosis of FES can be challenging and despite Gurd and Wilson's criteria (Table 1) have been adopted in clinical practice; no formal diagnostic criteria have been validated with large studies [12]. The clinical condition and neuroradiological imaging was compatible with fat embolism and "starfield pattern" [13,14]. High-risk patients should be monitored closely for subclinical signs of respiratory insufficiency and with positive radiographic changes [15]. Other clinical signs of fat embolism are petechial rash, tachycardia, fever, retinal fat or petechiae, urinary fat globules or oligoanuria, sudden drop in Hg-level, sudden thrombocytopenia, high erythrocyte sedimentation rate and fat globules in sputum [16]. There is no specific treatment for fat embolism or fat embolism syndrome. Evidence has suggested that corticosteroids may be effective at preventing FES associated with long bone fractures [17]. The type 1 starfield pattern is usually reversible, thus resulting in better prognosis. It is most commonly observed in the acute stages, rather than in subacute or late stages [18].
Table 1: Two major criteria or 1 major criterion and 4 minor criteria suggest a diagnosis of fat embolism syndrome. View Table 1
We reported a rare case of isolated FES occurred after high-risk orthopedic injury. The patient fortunately went on to full cognitive recovery due to early diagnosis and appropriate supportive therapy. We must always suspect isolated FES in polytrauma patient, even if the classical findings are not present, performing an early MRI to confirm the diagnosis.