Poncet's disease is a rare form of reactive arthritis described in people with active Tuberculosis (TB). We report a case of Poncet's disease in a 17-year-old boy who posed a diagnostic challenge because of the presence of purulent effusion from affected joints. His arthritis preceded pulmonary symptoms which were in fact mild and largely subclinical. Clinical remission occurred within 10 days of anti-Tuberculous therapy and the diagnosis of Poncet's disease was established. The case highlights the need to consider Tuberculosis as a cause of arthritis even in the absence of established Pulmonary Tuberculosis especially in endemic areas.
About 10-35% of all extra-pulmonary Tuberculosis (EPTB) affects the skeletal system with the commonest form being TB of the spine, Pott's disease. Tuberculosis that affects the joints occurs in three forms: Tuberculous arthritis, Poncet's disease and rarely a prosthetic joint infection by the organism.
Tuberculous arthritis is often a mono-articular infection of the joint by the Mycobacterium organism in which case there is an objective demonstration of the presence of the organism in the affected joint. Poncet's disease on the other hand is an aseptic arthritis reactionary to the presence of pulmonary Tuberculosis or some form of extra-pulmonary tuberculosis excluding the affected joints themselves. It is otherwise referred to as tuberculous rheumatism and there is no direct invasion of the joint by the Mycobacterium organism. It was described by the Frenchman Poncet in 1897 and is often polyarticular.
This case was reported because of the diagnostic challenge it posed and the relative rarity of Poncet's disease. It should always be considered in people with polyarticular arthritis for whom most of the common causes have already been ruled out.
A 17-year-old boy presented to us with fever and painful swelling of the right shoulder and elbow joints for 4 days' duration. The following joints were also swollen and painful howbeit at a lesser extent; left shoulder, left elbow, both knees and right ankle. The hip joint was initially spared, and all the small joints were also spared. He was not a known sickle cell disease patient, did not have symptoms of anaemia, and had no rashes, oral ulcers, early morning joint stiffness, dysuria, urethral discharge, night sweats, anorexia, recent sore throat, or dysphagia. He however had 10 episodes of non-bloody, non-mucoid diarrhoea a day prior to presentation.
On examination, he looked small for age, mildly pale, febrile with temperature of 38.1 �C and had a hyperactive precordium but no lymphadenopathy or erythema nodosum. The right shoulder, right elbow and left ankle were swollen, warm and tender. All the large joints except both hips were tender on passive motion. Frank pus was drained from two of the affected joints; analysis showed pus cells, WBC of 9,000 with neutrophils of 4,000, negative GeneXpert for Mycobacterium and no bacterial growth.
The total white blood cell count was 15.2 × 109 /L with differential neutrophilia and haemoglobin was 9.9 g/dl, with a microcytic hypochromic picture that kept declining on admission necessitating transfusion of two units of blood at some point. The erythrocyte sedimentation rate and C-reactive proteins were all elevated. ESR was 59, reduced to 48 while on admission and subsequently rose again to 141. C-reactive protein was 185 and subsequently rose to 282. Rheumatoid factor was negative and Anti-nuclear antibody was only weakly positive (1:80). Blood cultures on three different occasions taken at the heights of fever did not grow any bacteria. HIV screening was also negative. Haemoglobin electrophoresis revealed a genotype of AA. An echocardiogram did not reveal any features suggestive of infective endocarditis. Radiographs of all affected joints looked grossly normal.
A diagnosis of sepsis with polyarticular septic arthritis with differentials of adult-onset Still's disease was made and parenteral clindamycin and ceftriaxone commenced. These were later reviewed at Meropenem after no improvement was observed. Surgical arthrotomy was also done with drainage of 150 ml of pus from the right shoulder, 30 ml each of frank pus from right elbow and left ankle joints. The patient continued to spike temperatures with involvement of new joints and swelling of previously drained joints.
After the second week on admission, the patient developed a moderate right pleural effusion that prompted further chest imaging with CT scan revealing a left lung consolidation with associated pleural thickening and cavitation as well as a solitary left lung nodule all of which were consistent with pulmonary tuberculosis. Pleural fluid adenosine deaminase levels were however in normal range. A multidisciplinary team of orthopedic surgeons, rheumatologists, infectious disease specialists and respiratory physicians held a meeting and made a consensus of a possible disseminated Tuberculosis, recommending commencement of anti-Tuberculosis therapy and investigating for a primary immunodeficiency syndrome which came out non-suggestive. A colonoscopy was done following a second episode of explosive diarrhoea which revealed widespread multiple whitish deposits in the colon suggestive of tubercles in gastrointestinal tract.
Temperatures settled after eight days of anti-Tuberculous therapy and all joint swellings resolved after ten days of treatment. All joints became completely pain-free after two weeks of the anti-TB therapy. He was discharged after 40 days of admission with continued physiotherapy (Figure 1, Figure 2, Figure 3, Figure 4 and Figure 5).
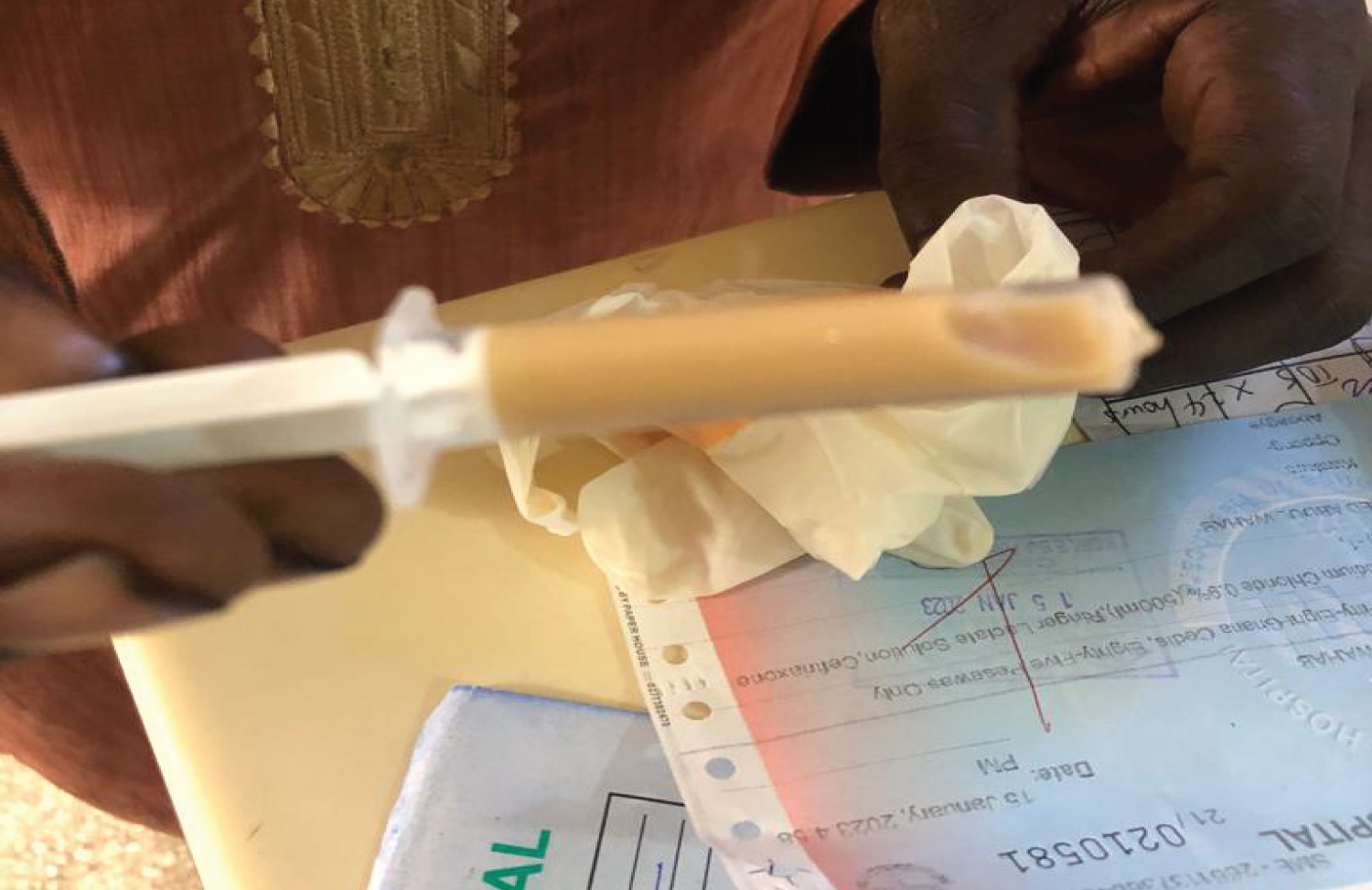 Figure 1: Frank pus drained from right shoulder.
View Figure 1
Figure 1: Frank pus drained from right shoulder.
View Figure 1
 Figure 2: Temperature chart showing rising temperature peaks while on antibiotics.
View Figure 2
Figure 2: Temperature chart showing rising temperature peaks while on antibiotics.
View Figure 2
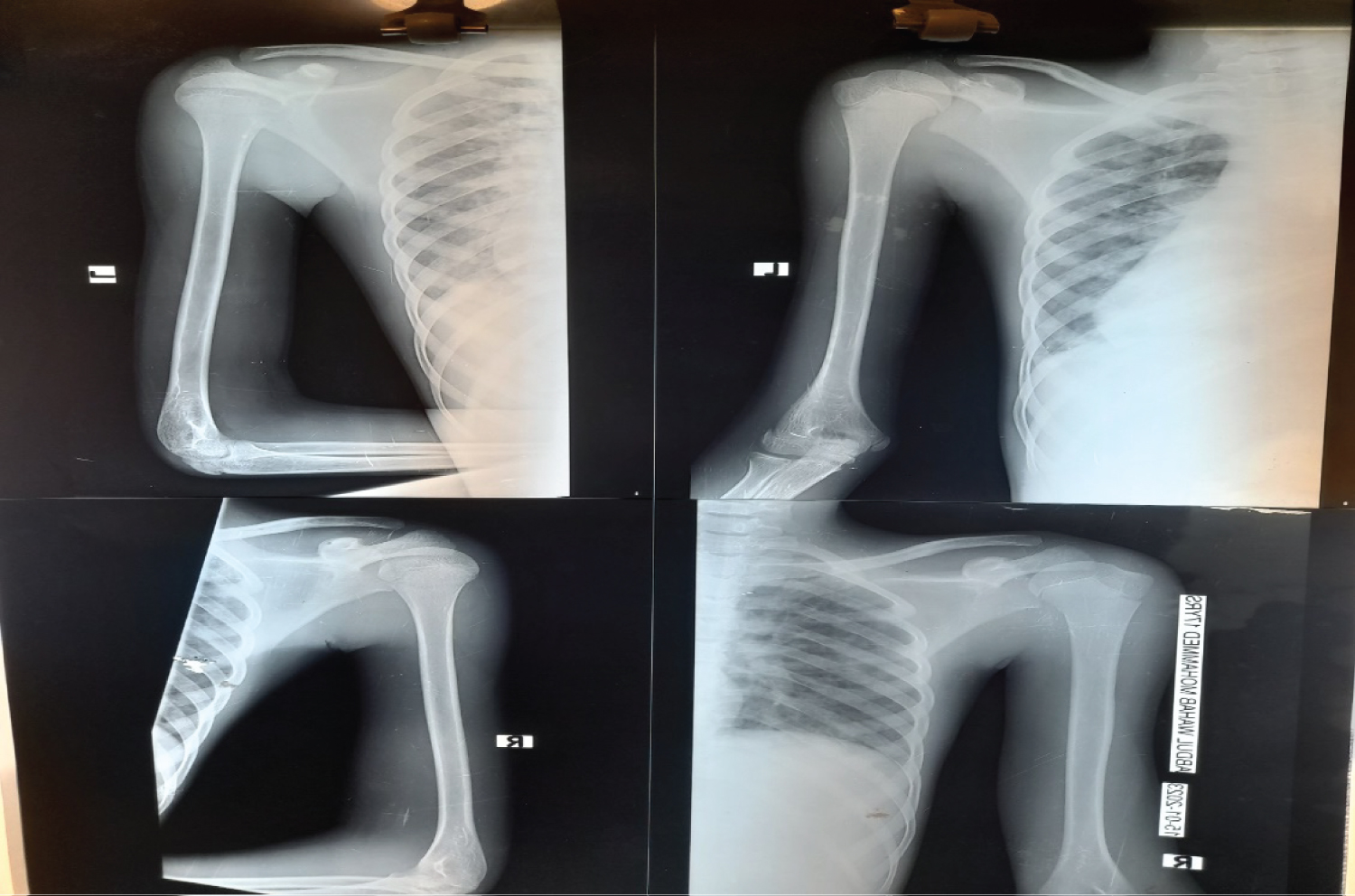 Figure 3: Plain radiographs of affected joints showing no typical changes.
View Figure 3
Figure 3: Plain radiographs of affected joints showing no typical changes.
View Figure 3
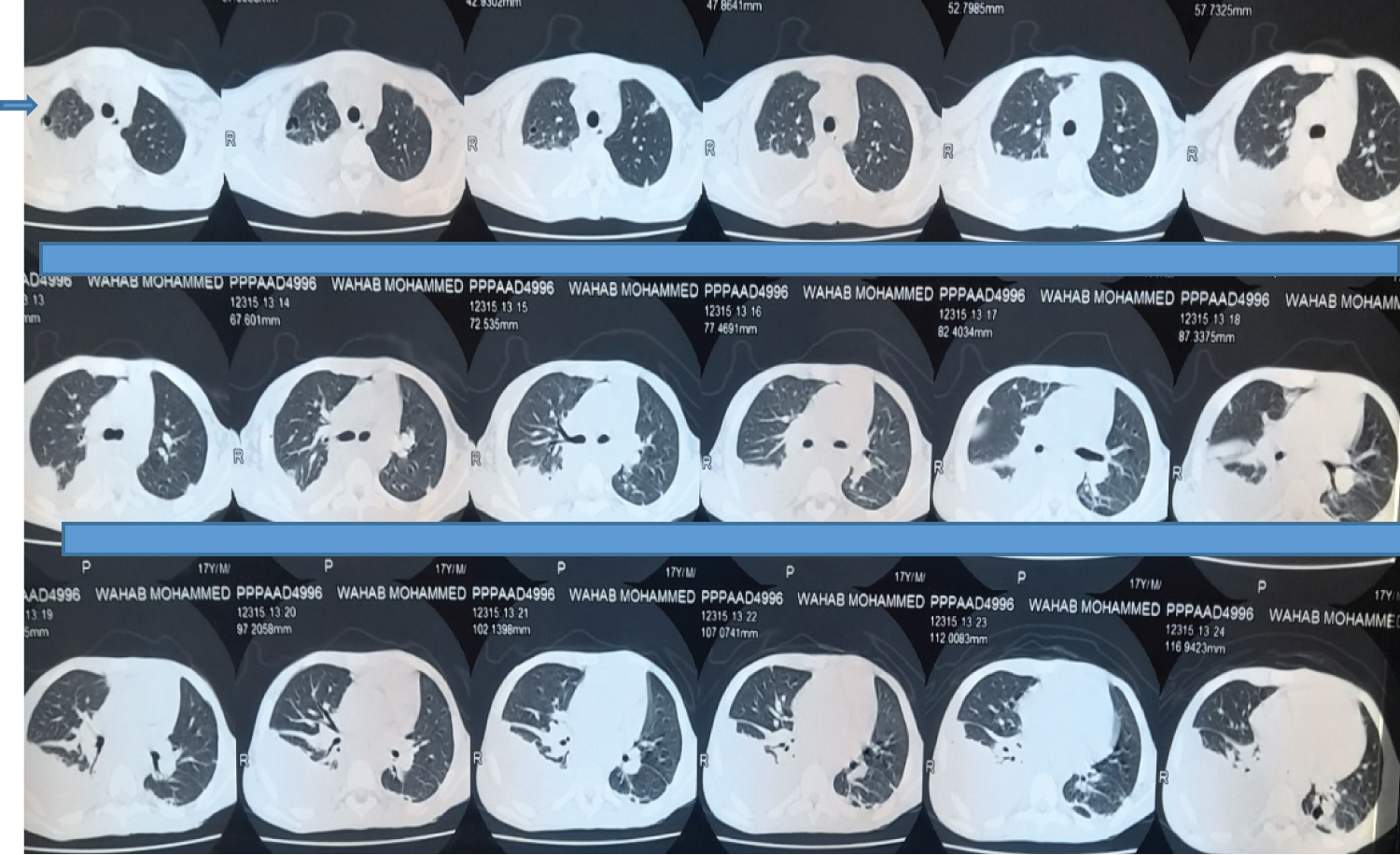 Figure 4: Chest CT scan showing left lung consolidation with cavitation, solitary left lung nodule and a right para-pneumonic effusion.
View Figure 4
Figure 4: Chest CT scan showing left lung consolidation with cavitation, solitary left lung nodule and a right para-pneumonic effusion.
View Figure 4
 Figure 5: Showing multiple whitish deposits (tubercules) in the colon on colonoscopy.
View Figure 5
Figure 5: Showing multiple whitish deposits (tubercules) in the colon on colonoscopy.
View Figure 5
Despite the availability of effective therapy and improved general living conditions, Tuberculosis is still endemic in large parts of the world including sub-Saharan Africa. The potential of Tuberculosis to trigger reactive manifestations even when subclinical is important to note as occurred in our patient [1]. Joint inoculation by tubercule bacilli is mainly monoarticular with predilection for the hip and knee joints. This is referred to as tuberculous arthritis. An objective demonstration of the presence of the bacilli in the affected joint is mostly present and radiographic changes such as peri-articular osteoporosis, peripherally located osseous erosions and gradual joint narrowing are often present without the classic features of inflammation. The presentation of our patient makes this kind of arthritis unlikely as he had a polyarticular involvement with classic features of inflammation and failure to objectively identify the presence of the tubercle bacilli in affected joints.
Although polyarticular septic arthritis was initially entertained as a diagnosis for our patient especially following the aspiration of frank pus from the affected joints, it was later thought less likely. The failure to culture any organisms from the joint aspirate and blood, the lack of response to optimum doses of parenteral antibiotics as well as the findings on colonoscopy made a septic arthritis less likely. Even though polyarticular septic arthritis forms 20% of all septic arthritis, it is not sufficiently recognized as a possibility [2]. It often occurs in patients with sepsis or an underlying rheumatoid arthritis or may be a presenting manifestation of an infective endocarditis [3]. A definitive diagnosis of septic arthritis may be made in the setting of positive synovial fluid Gram stain and/or culture. It is noteworthy that the sensitivity of Gram stain is around 30% to 50% and that of synovial fluid culture is more than 60% for non-gonococcal septic arthritis [4]. Blood cultures are positive in approximately 50% of septic arthritis from haematogenous seeding. The above sensitivities of these tests raised questions about the possibility of our patient having polyarticular septic arthritis due to a bacterium that was not identified by any of these tests.
Much like our patient, a case was published in the international journal of advances in Medicine in 2015, of a 17-year-old girl who presented with polyarticular arthritis and a low-grade fever of two weeks' duration that did not identify any organisms from blood or joint aspirate. Radiographs of the joints showed essentially normal bone and joint morphologies. ANA, anti-CCP and Rheumatoid factor were all negative. ESR was elevated with a strongly positive Mantoux test, so patient was managed as Poncet's disease with anti-Tuberculosis therapy showing marked symptom improvement in 2 weeks and complete resolution in 6 weeks. Mantoux was not considered as a viable investigatory test because of the endemicity of Tuberculosis in our setting and the widespread positivity in our general population to Mantoux testing.
Poncet's disease, otherwise known as tuberculous rheumatism, is aseptic, often polyarticular and considered reactive to the presence of active Tuberculosis elsewhere in the body [5]. There is no definite microbial evidence of the presence of the Mycobacterium in the affected joints [6]. Response to anti-Tuberculous therapy is prompt and often leaves no residual joint damage. Involvement of the sacro-iliac joint raises doubt about the diagnosis, there have however been two reported cases of Poncet's disease with sacro-iliac joint involvement. It is essentially a diagnosis of exclusion. Sharma, et al. proposed a diagnostic criterion for Poncet's disease with essential, major, and minor criteria. Our patient largely fulfilled all the necessary criteria to be a definite Poncet's disease however we find it inexplicable that the aspirate from the affected joints was purulent as that is not typical of Poncet's disease in which case the joint effusion is aseptic. Could there have been Poncet's arthritis with a superimposed bacterial infection? No such case was found in existing literature, and we could not objectively identify any superimposed bacteria either (Table 1).
Table 1: Criteria for diagnosing Poncet's disease proposed by Sharma, et al. View Table 1