Background: Pregnancy-induced hypertension (PIH) demands swift diagnosis and treatment. However, in rare cases, severe PIH may result from an underlying secondary cause, necessitating comprehensive evaluation.
Case: A 30-year-old primigravid at 31 weeks of gestation was initially diagnosed ARDS and severe PIH at an external facility. Despite aggressive management, her blood pressure remained high. An incidental chest CT scan revealed overlooked coarctation of the aorta. Other secondary causes, like pheochromocytoma and renovascular hypertension, were explored.
Conclusion: This case highlights diagnostic challenges with severe PIH and the importance of considering secondary hypertension in pregnancy. Timely identification and management of secondary hypertension can improve outcomes.
Clinical significance: Prompt recognition of secondary causes in severe PIH is crucial for tailored management and better outcomes. Awareness among healthcare professionals is vital to optimize care to pregnant patients with severe hypertension, reducing potential risks and enhancing healthcare quality.
Coarctation of the aorta is a narrowing, commonly occurring beyond the left subclavian artery, raising upper body blood pressure, and causing upper extremity hypertension. Left unrepaired, it leads to premature coronary artery disease, ventricular dysfunction, aortic aneurysm/dissection, and cerebral vascular disease by the third or fourth decade [1].
Hypertensive disorders in pregnancy risk maternal and fetal health. From gestational hypertension to severe preeclampsia-eclampsia, prompt diagnosis and management are crucial.
A 30-year-old pregnant woman at 31 weeks presented with ARDS and pregnancy-induced hypertension (PIH). Despite early delivery for PIH, she continued to have refractory hypertension even on multiple antihypertensives.
Investigating the cause for secondary hypertension, possibilities such as pheochromocytoma, renovascular hypertension, and primary aldosteronism were considered. Incidentally, coarctation of the aorta was discovered during a chest CT scan done to find pulmonary complications.
This case highlights the importance of comprehensive diagnostics for severe hypertension in pregnancy, considering rare etiologies like coarctation of the aorta alongside the common causes. Early recognition and management are vital to prevent complications. Maternal complications encompass cerebral infarction, aortic dissection, aortic rupture, congestive heart failure, hypertensive crisis, and infective endocarditis. Meanwhile, fetal complications comprise growth retardation and premature birth, carrying an elevated risk of placental ischemia or abruption [2].
Moreover, initial concerns of ARDS were refuted by further evaluation, emphasizing the need for accurate diagnosis and treatment.
In conclusion, this case underscores the complexities in managing hypertensive disorders during pregnancy, necessitating a multidisciplinary approach. Timely recognition, accurate diagnosis, and proper intervention are essential for improved outcomes in pregnant women with hypertension.
A 30-year-old P2G1L1 pregnant female (POG 31 week) with no known comorbidity presented in our causality with the diagnosis of ARDS and PIH from outside hospital. She was intubated at outside facility in view of hypoxemia and managed with empirical antibiotics and thyroid replacement.
Upon examination at our facility, the patient was found to be sedated and paralyzed with an endotracheal tube in place. Her heart rate (HR) was 98 beats/minute, blood pressure (BP) was 220/110 mmHg, and blood oxygen saturation (SpO 2 ) was 100% with FiO 2 of 1.0. Bilateral coarse crepitations were heard on auscultation and fetal heart sounds were present. An obstetric ultrasound revealed a single live fetus at 31 weeks and 2 days. Intravenous loading of magnesium sulfate was initiated, followed by infusion of magnesium sulphate and labetalol to address accelerated hypertension and prevent eclamptic seizures. The patient's treatment plan also included intravenous antibiotics, oral antihypertensive medications (clonidine & amlodipine) and intravenous steroids for fetal lung maturity. Ventilatory management was adjusted to follow a lung-protective strategy for ARDS. Routine blood investigations revealed an elevated total leukocyte count (TLC). A 2D echocardiogram showed Left ventricular ejection fraction (LVEF) 55%, with no RWMA. The RA and RV were mildly dilated with moderate to severe tricuspid regurgitation (PASP of 68 mmHg). Urine analysis showed no signs of proteinuria.
On the same day, a bronchoscopy was performed, and BAL sample BioFire® analysis indicated the presence of Acinetobacter (NDM/OXA 48+). Consequently, the patient's antibiotics were modified. A caesarean section was carried out on the day two of admission. Despite different antihypertensive medications (amlodipine, clonidine, labetalol) along with intravenous infusions of nitroglycerin and IV sedation, her blood pressure remained uncontrolled. A conservative fluid strategy was implemented. Following the delivery, the patient's ventilatory parameters improved, leading to extubation on third day on NIV support. However, the blood pressure remained uncontrolled despite the current medications and then only alternative diagnoses were considered. Further investigations were planned, including urine vanillylmandelic acid (VMA) testing, renal doppler, and bilateral adrenal imaging, to explore the possibility of other causes of secondary hypertension. On day six, Chest X Ray followed by CT scan of the chest revealed complete collapse of the left lower lobe with mediastinal shift to the left side. The mediastinal and hilar margins were obscured, and the descending aorta appeared dilated.
Repeat echocardiogram revealed a severely narrowed proximal descending thoracic with maximum peak gradient across the distal thoracic artery was 76 mmHg, Moderate TR with pulmonary artery pressures of 78 mmHg. An aortogram and CT angiography of the aortic arch confirmed the findings of CT scan of coarctation of the distal aortic arch just below the origin of the left subclavian artery, with folding of the aorta at that level (Figure 1). The diameter of the narrowing was approximately 6.8 mm, while the post-stenotic dilation of the descending aorta measured 37 mm. The patient's symptoms improved with treatment and while definitive treatment for coarctation was being planned, the patient's relations planned to shift her to another facility. Subsequently she was discharged to a government hospital on nasal prongs with five different oral antihypertensives (amlodipine, clonidine, prazosin, labetalol, and telmisartan).
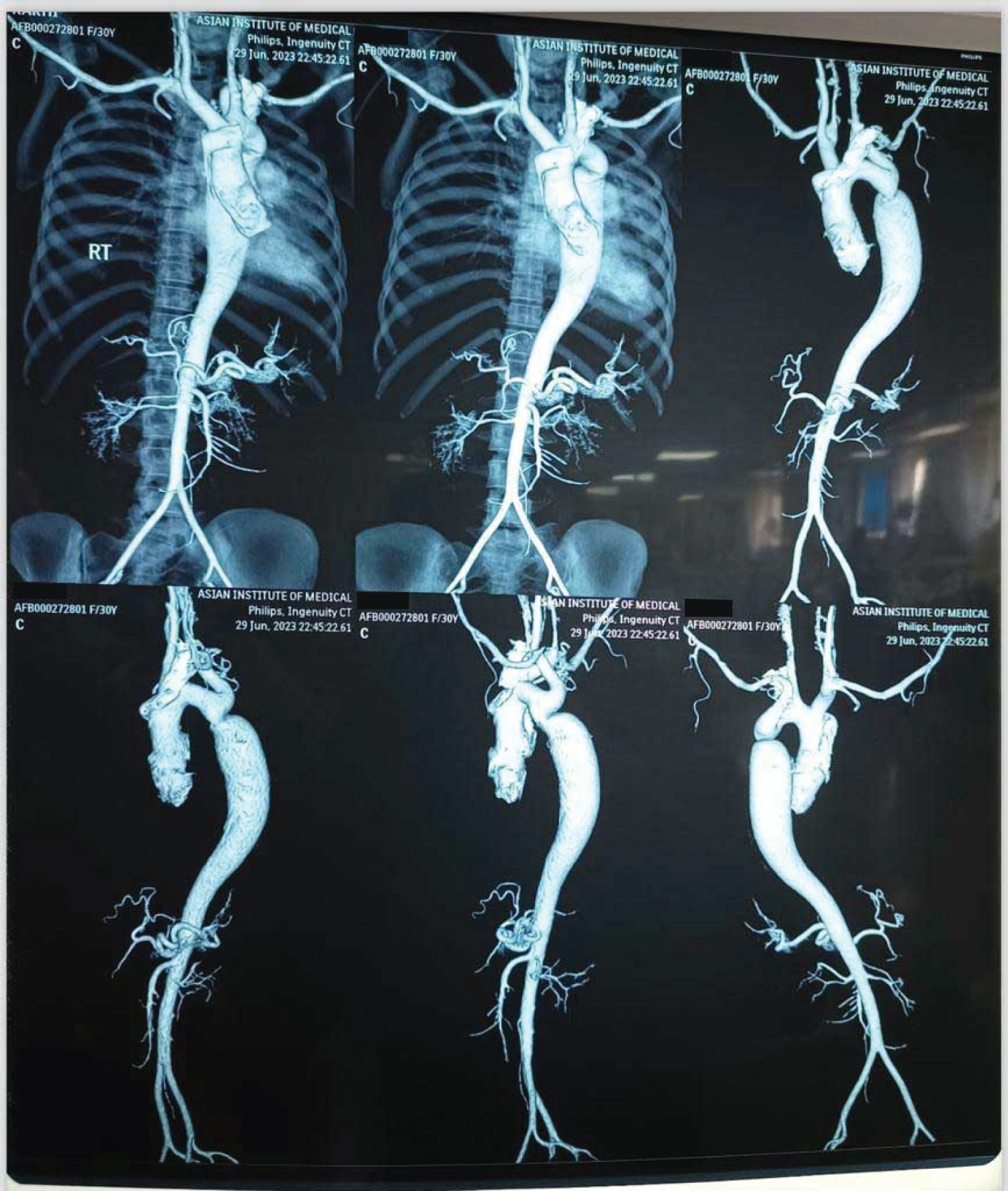 Figure 1: Aortogram CoA.
View Figure 1
Figure 1: Aortogram CoA.
View Figure 1
American College of Obstetricians and gynaecologists(ACOG) defines hypertension in pregnancy as systolic blood pressure(SBP) ≥ 140 mmHg and/or diastolic blood pressure(DBP) ≥ 90 mmHg (measured ≥ 4 hrs apart). Severe hypertension is classified as SBP ≥ 160 mmHg and/or DBP ≥ 110 mmHg (measured ≥ 4 hrs apart). Chronic/pre-existing hypertension refers to hypertension before conception or < 20 weeks gestation. Gestational hypertension is characterised as onset after 20 weeks, resolves after childbirth. Preeclampsia-eclampsia is defined as new-onset hypertension after 20 weeks + proteinuria and/or maternal/uteroplacental dysfunction [3].
Our patient, without prior hypertension history, presented at 31 weeks of pregnancy with high blood pressure. Her husband revealed she had hypertension in her previous pregnancy, but we lacked inter-pregnancy blood pressure data. Despite severe hypertension (BP > 160 mmHg), neither of urine protein, organ dysfunction, thrombocytopenia, neurological complications, or uteroplacental dysfunction was found, ruling out preeclampsia. Due to uncontrolled hypertension, we opted for early delivery to manage severe pregnancy-induced hypertension (PIH). However, post-delivery, her blood pressure remained persistently high, unresponsive to multiple antihypertensive medications.
Pheochromocytoma is a significant threat during pregnancy, with high morbidity and mortality if undiagnosed. So, ruling it out is crucial when dealing with severe hypertension in pregnant women. For chronic hypertension, assessing signs of target-organ damage (e.g., left ventricular hypertrophy, hypertensive retinopathy, and azotemia) is also essential [4].
Our diagnostic workup was focused on investigating the possibility of pheochromocytoma, renovascular hypertension, and primary aldosteronism. However, we did not include clinical examination or diagnostic tests specifically targeting the diagnosis of coarctation of the aorta. The decision to perform a CT scan of the chest was primarily intended to rule out any lung-related issues such as consolidation or pulmonary congestion. The identification of coarctation of the aorta was an incidental finding during the imaging process.
Receiving mechanical ventilation with an ARDS lung protective strategy, the patient's static lung compliance improved and oxygen requirement decreased. Her chest X-ray showed noticeable improvement after bronchoscopy. Despite persistent high blood pressure suggesting a condition other than sepsis, her elevated procalcitonin level (5.0) and the BAL sample's BioFire® analysis indicated Acinetobacter growth.
On the first day of admission, the 2D echocardiography missed the finding favouring the diagnosis of coarctation of aorta. Several other important aspects such as Bilateral lower limb doppler studies were not performed to assess for deep vein thrombosis or pulmonary embolism. Furthermore, we had missed the assessment of blood pressure discrepancy between the upper and lower limbs, which could have provided valuable diagnostic clues.
Coarctation of the aorta was not initially identified rather it was incidentally discovered through a chest CT scan performed to rule out pulmonary complications.
Most cases of chronic hypertension in pregnancy are attributed to essential hypertension. However, it is important to consider secondary causes of hypertension, such as intrinsic renal disease, renovascular hypertension, primary aldosteronism, Cushing's syndrome, and pheochromocytoma, especially in cases where blood pressure is exceptionally high [5].
This case highlights the complexity of diagnosing severe hypertension in pregnancy. The case underscores the importance of considering secondary causes of hypertension and conducting comprehensive diagnostic workups in pregnant patients with uncontrolled blood pressure. It emphasizes the need for thorough evaluation to avoid overlooking rare but potentially life-threatening conditions during pregnancy.
In this case study, we presented the complex medical management of a 30-year-old pregnant woman at 31 weeks of gestation with severe hypertension and acute respiratory distress syndrome (ARDS). Despite initial treatment for suspected ARDS and pneumonia, the patient's condition did not improve, prompting further investigations.
Upon a series of diagnostic examinations, including echocardiography and CT imaging, the patient was incidentally diagnosed with coarctation of the aorta, a condition causing narrowing of the aorta, leading to elevated blood pressure. This diagnosis explained the persistent and unresponsive hypertension experienced by the patient throughout her admission.
The case highlights the importance of considering secondary causes of hypertension during pregnancy, even in the absence of prior hypertension history. Additionally, it underscores the need for a comprehensive diagnostic workup, especially when managing complex medical conditions in pregnant patients. Early identification of coarctation of the aorta allowed for timely intervention and appropriate management, leading to an improvement in the patient's symptoms and her subsequent discharge with multiple oral antihypertensive medications.
Clinicians should remain vigilant for rare or incidental findings during diagnostic imaging and consider all potential causes of severe hypertension in pregnant patients to ensure timely and effective care.
We have no conflicts of interest to disclose.