Dewinter's syndrome is a life-threating electrocardiographic (ECG) diagnosis, indicates a proximal left anterior descending artery (LAD) disease. It is rarely reported finding post blunt chest trauma and it requires an abruptly intervention. We report a young gentleman previously healthy that developed an anterior myocardial infarction following a blunt chest trauma and ECG was showing de winter syndrome.
Myocardial Infarction, Coronary Angiography, Electrocardiogram, Case report
De Winter Syndrome is considered equivocal for and ST elevation myocardial infarction. It has been reported to represent a proximal left ascending artery occlusion [1]. Simlar to ST elevation myocardial infarction underlying risk factors including diabetes, dyslipidemia and hypertension and the most presenting symptom being chest pain [2]. We report in this case of chest trauma and his electrocardiogram showing a de winter pattern.
A 36-year-old male smoker with no significant previous medical history presented to our emergency department 40 minutes after sustaining blunt trauma to his head and chest in a fight. His chief complaint was chest pain that began 10 minutes after the assault, described as a squeezing pressure on the left side of his chest, radiating down his left shoulder and arm, graded as intensity 7/10. On examination, the patient was conscious, oriented, and vitally stable with HR 110 bpm, BP 130/90 mmHg, RR 18 breaths/minute, and SpO 2 99%. Primary survey was negative. He was found to have a small contusion over ribs VIII-X anteriorly, with tenderness of the left costal arch and lower sternum present. His pulses were present and equal bilaterally. Extended FAST scan was negative. The patient’s ECG shows ST elevation in aVR, and ST depressions with symmetrical upright T waves in the anterior leads - de Winter waves (Figure 1).
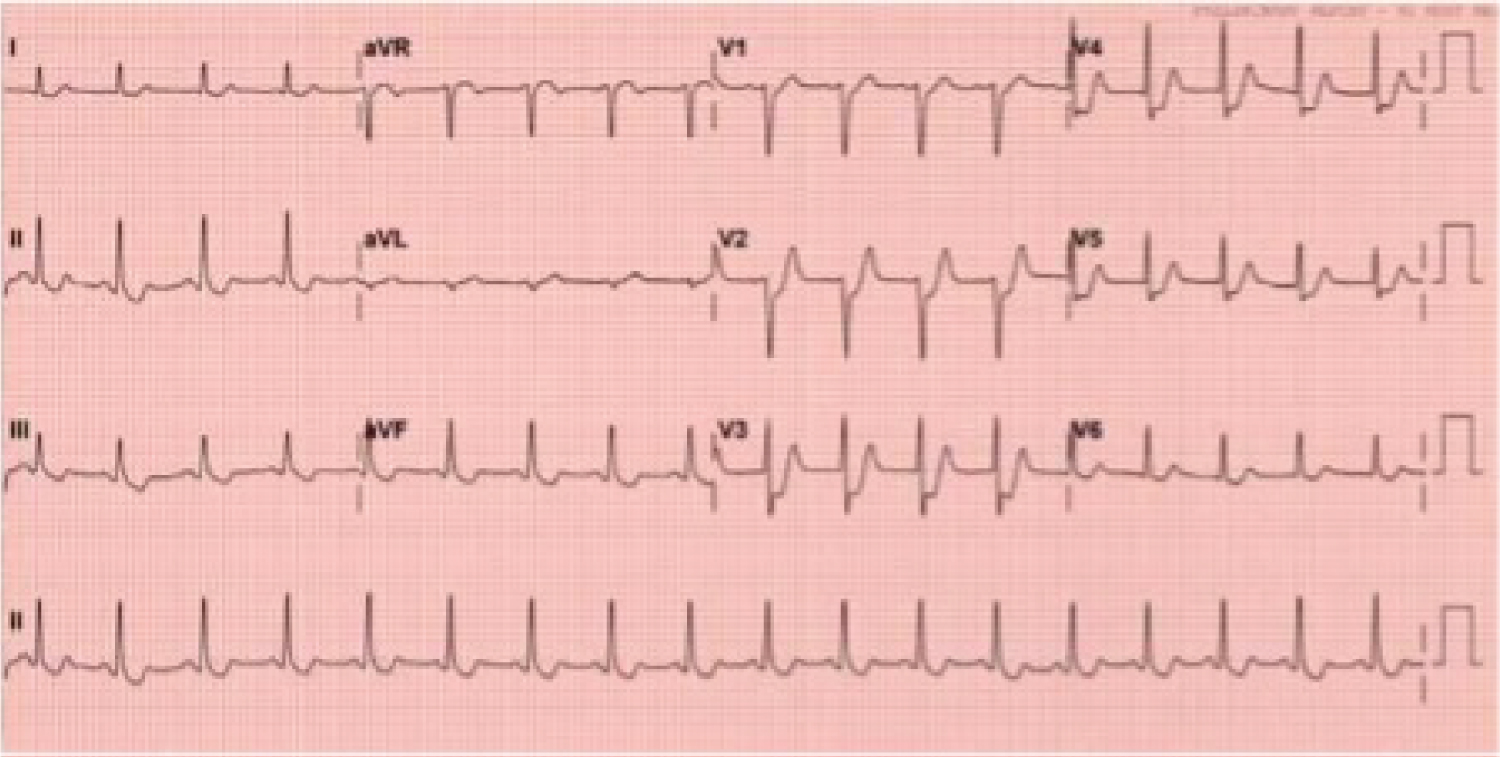 Figure 1: Patient's ECG showing de-winter waves.
View Figure 1
Figure 1: Patient's ECG showing de-winter waves.
View Figure 1
Echocardiography demonstrated an ejection fraction of 30-40%, hypokinesia of the interventricular septum, and a dilated ascending aorta without aortic regurgitation. A CT polytrauma scan was done to assess for traumatic aortic dissection before primary percutaneous coronary intervention could be considered, and it was found to be within normal limits. Laboratory values were regular save for elevated levels of LDL cholesterol (159 mg/dL) and total fasting cholesterol (206 mg/dL). Cardiac enzymes 30 minutes after chest pain began were insignificant with troponin measuring 9 ng/L and CKMB measuring 2.1 ng/mL.
The patient was taken for an urgent coronary angiography that showed a proximal total occlusion of the left anterior descending artery (LAD). One drug-eluted stent was placed with positive outcome. The patient was discharged 3 days later in a stable condition and pain-free (Figure 2a and Figure 2b).
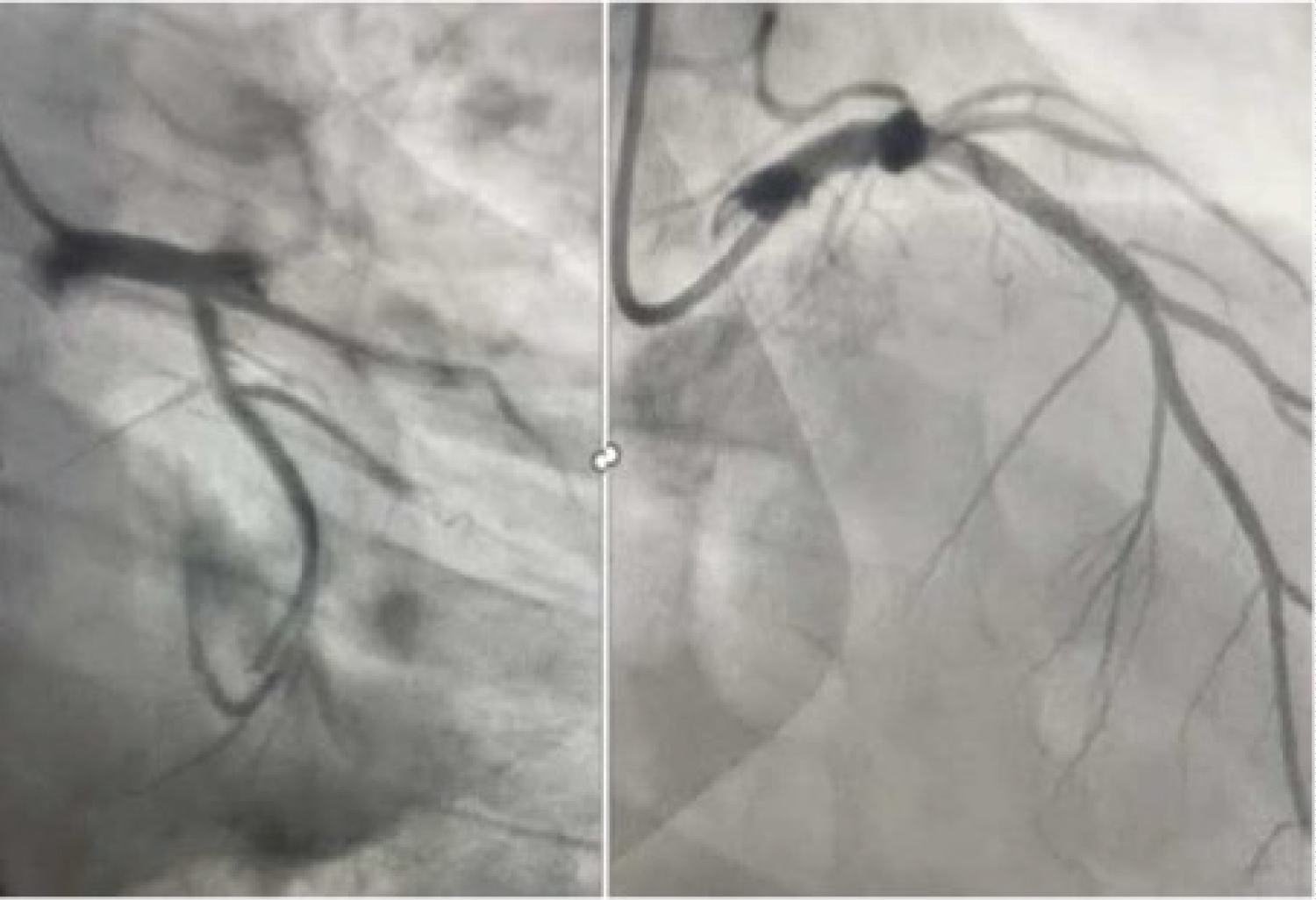 Figure 2: Patient's coronary angiography showing proximal total occlusion of the left anterior descending artery.
View Figure 2
Figure 2: Patient's coronary angiography showing proximal total occlusion of the left anterior descending artery.
View Figure 2
First described in 2008 de winter, et al. found that 2% of 1532 patients had the “de winter syndrome” electrocardiogram (ECG) changes had on coronary angiography an anterior myocardial. De winter syndrome ECG criteria include 1-3 mm of ST-depression with upright, symmetrical T-waves [1]. Although a rare finding it has extensively reported to represent a proximal LAD occlusion especially as a number of case report showed progression of the ECG in patient to ST elevation myocardial infarction [2].
Several case reports have been published associating acute myocardial infarction to chest trauma secondary to aortic dissection or a preexisting aortic aneurysm [3,4]. Furthermore Kumar, et al. reported a case of young healthy male that deceased after sustaining a blunt chest trauma (BCI) and on autopsy was found to have a thrombus in the proximal LAD attributing it to a rupture of a plaque secondary to the BCI [5]. To the authors knowledge, this article is the first to report a case of a young male sustaining an acute myocardial infarction requiring stenting with no underlying aortic dissection or aortic aneurysm secondary to a BCI. Our patient had no history suggestive of stable angina prior to presentation hence we suggest that the triggering factor for his acute myocardial infarction is a rupture of a preexisting plaque secondary to the chest trauma he got.
Furthermore, it is crucial to emphasize on the recommendation of the eastern association for surgery that all blunt cardiac injury patient should undergo an ECG, cardiac monitoring and laboratory cardiac enzymes testing to rule out myocardial injury; as seen in the above-described case [6].
No funding source was for this manuscript.
Authors have no relationships relevant to the contents of this paper to disclose.
None.