Primary cutaneous CD4- positive small/medium T-cell lymphoproliferative disorder (PCSM-TCLD) is a low-grade cutaneous T-cell disorder, previously classified as a provisional entity [1] of primary cutaneous CD4+ small/medium pleomorphic T-cell lymphoma until 2016, when the terminology was changed during the revision of the classification of lymphomas by the World Health Organisation and the European Organisation for Research and Treatment of Cancer due to its uncertain malignant potential [1,2]. We report a case report with spontaneous regression after skin biopsy.
A 50-year-old female patient with no notable history. She presented with a nodular lesion of the face, painless and not very pruritic, evolving for 2 months, without improvement with topical treatments (dermocorticoid, antifungal and antibiotic). On examination, there was a single round, firm, nodular erythematous lesion, 2 × 2.5 cm in diameter, located on the chin (Figure 1A). There were no systemic symptoms or palpable adenopathies. Histological examination showed skin covering with an orthokeratotic stratum corneum and a thin, discretely papillomatous epidermis. The dermis was the site of an atypical, diffuse lymphocytic infiltrate infiltrating the dermis, reaching the subcutaneous layer and involving the perivascular tissue. The immunohistochemical study showed a predominance of CD3+ T cells with CD4+ immunopositivity and the presence of a few CD8+ T cells, without CD20 expression (Figure 2). Tests for Epstein-Barr virus and human T-cell lymphotropic virus were negative. This was consistent with primary cutaneous CD4+ small/medium T-cell lymphoproliferation. Paraclinical tests included normal liver and kidney function tests, serum protein electrophoresis and complete blood count. The cervico-thoraco-abdomino-pelvic CT scan came back without any abnormality. The course was marked by spontaneous regression of the nodule after skin biopsy, with flattening and total disappearance of the lesion and reduction of the erythema at 10 weeks (Figure 1B). No recurrence was observed during a 12-month follow-up.
 Figure 1: (A,B) Erythematous nodular lesion on the chin and its regression after skin biopsy.
View Figure 1
Figure 1: (A,B) Erythematous nodular lesion on the chin and its regression after skin biopsy.
View Figure 1
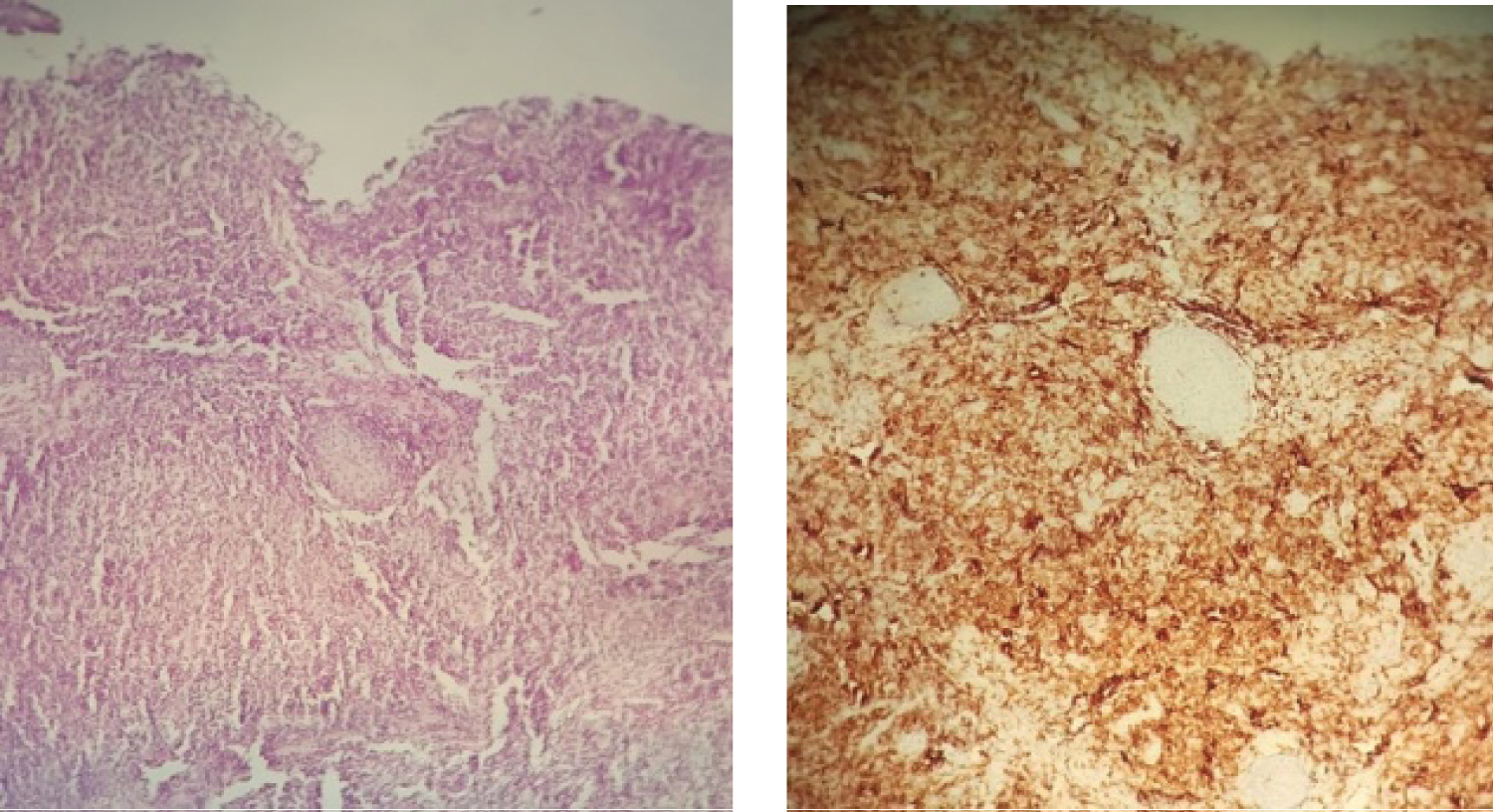 Figure 2: Histological and immunohistochemical appearance showing a diffuse dermal inflammatory infiltrate of atypical lymphocytes with a predominance of TCD3+, CD4+ cells and the presence of a few TCD8+ cells.
View Figure 2
Figure 2: Histological and immunohistochemical appearance showing a diffuse dermal inflammatory infiltrate of atypical lymphocytes with a predominance of TCD3+, CD4+ cells and the presence of a few TCD8+ cells.
View Figure 2
Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (PCSM-TCLD) is a rare disease that represents about 2-3% of all primary cutaneous lymphomas [3,4]; it occurs most commonly in patients aged between 50 and 60 years with a median age at diagnosis of 51-53 years [3], but is occasionally seen in children [5] with a slight male predominance [6,7].
Clinically, it usually manifests as an asymptomatic, erythematous, or purplish papule, plaque, nodule or single tumour on the face, neck or upper trunk [4-7]. However, it may rarely occur in other areas, taking on a multi-nodular or multifocal form or accompanied by symptoms such as pain [2-7] or ulceration of lesions [8].
Histologically, it is characterised by a dense nodular or diffuse T-cell infiltrate, mainly located in the dermis. This infiltrate is composed of small to medium-sized pleomorphic CD4+/PD1+ T lymphocytes, associated with B lymphocytes, plasma cells, small CD8+ T cells, histiocytes and eosinophils [3-5,9]. There is a small proportion of large pleomorphic cells, up to 30%.
Epidermotropism may be present focally [1,4] with occasional perivascular and periannexal involvement, but epidermotropism or folliculotropism are not significant [9]. In most cases, the T cells involved express a CD3+3/CD4+/ CD8-/CD30-/PD1+ profile, but CD8+ cases have been described [4,5,10]. The Ki-67 proliferation index is generally low, and loss of CD5 and CD7 is uncommon [3]. It is interesting to note that CD20+ B cells are numerous and represent around 10-60% of the infiltrate [3,9].
The prognosis is generally excellent, especially for single lesions where the 5-year survival rate is over 90% [3,4,7]. In the case of multifocal presentation, the prognosis worsens, with a 5-year survival of 60-80% [1,3,4,6]. The prognosis depends on the size of the tumour, the presence of multiple nodules and differentiation [5]. An association has been proposed by Garcia-Herrera, et al. [11] between rapidly growing lesions, highly proliferative tumours and a low infiltrate of CD8+ cells with a poor prognosis.
Although there is no specific consensus regarding treatment. The conservative approach is an option, as cases of spontaneous remission after partial biopsy have been reported [6,12-16]. For patients with persistent lesions, the preferred treatment choices include corticosteroids (topical or intralesional), surgical excision and low-dose radiotherapy [3,5]. Doxycycline represents an alternative treatment [3,10] with its antineoplastic actions through inhibition of proliferation, induction of apoptosis and inhibition of angiogenesis.
Primary cutaneous CD4+ small/medium T-cell lymphoproliferative disorder (PCSM‐TCLD) is a rare and provisional entity of cutaneous lymphomas, which generally presents an indolent clinical course with uncertain malignant potential.