Morbihan disease (MD) is a rare entity. Its nosography is poorly understood, and its therapeutic management is difficult. We report a new case of MD. We report the case of a 39-year-old patient consulted in our department for a year with facial edema, erythema and papules reported by him, for which the patient was treated with cyclines, local and general corticosteroid therapy, without improvement. Clinical examination reveals significant edema of the forehead and eyelids with erythema of the cheeks covered with some telangiectasia. Clinical, biological, and histological findings lead to the diagnosis of Morbihan disease after exclusion of other diseases. Due to previous treatment failures, the patient was placed on duiretics with slight improvement. The particularity of our observation lies in the rarity and especially in the therapeutic difficulties encountered during this disease.
Chronic erythematous edema of the face, Morbihan, Rosacea
Morbihan disease is a rare condition of uncertain nosology. It is also known as persistent solid facial edema or lymphedematous rosacea [1]. Described for the first time in 1957 by the French dermatologist Robert Degos to a farmer from Morbihan (north-west of France), its pathogenesis is not entirely known, its therapeutic management is difficult [2], we report a case of Morbihan disease.
This is a 39-year-old patient with no notable pathological history. His history of the disease goes back 1 year, or the patient presented facial lesions for which he consulted a private dermatologist who put him under treatment. Topical without improvement then he consulted our training for treatment. The dermatological examination revealed an asymmetrical facial edema more accentuated in the right suborbital area associated with erythema, on dermoscopy (Figure 1). We noted the presence of an erythematous background, telangiectasias, the tails of the demodex, the patient benefited from an ophthalmic examination returning normal, a skin biopsy showing dermal edema associated with a mild papillary and peripilary inflammatory infiltrate made up of lymphocytes, polynuclear and eosinophils and macrophage without formation of epithelioid granuloma with presence of intrafollicular demodex conclusive to rosacea, given the absence of systemic signs and a muscular deficit we considered Morbihan disease (Figure 2). The patient was initially put on: Anti-redness cream, metronidazole, topical and oral, photoprotection. The evolution was marked by the disappearance of the erythema with a slight regression of the edema then the patient was put on diuretics.
 Figure 1: Asymmetrical facial edema more accentuated in the right suborbital area associated with erythema.
View Figure 1
Figure 1: Asymmetrical facial edema more accentuated in the right suborbital area associated with erythema.
View Figure 1
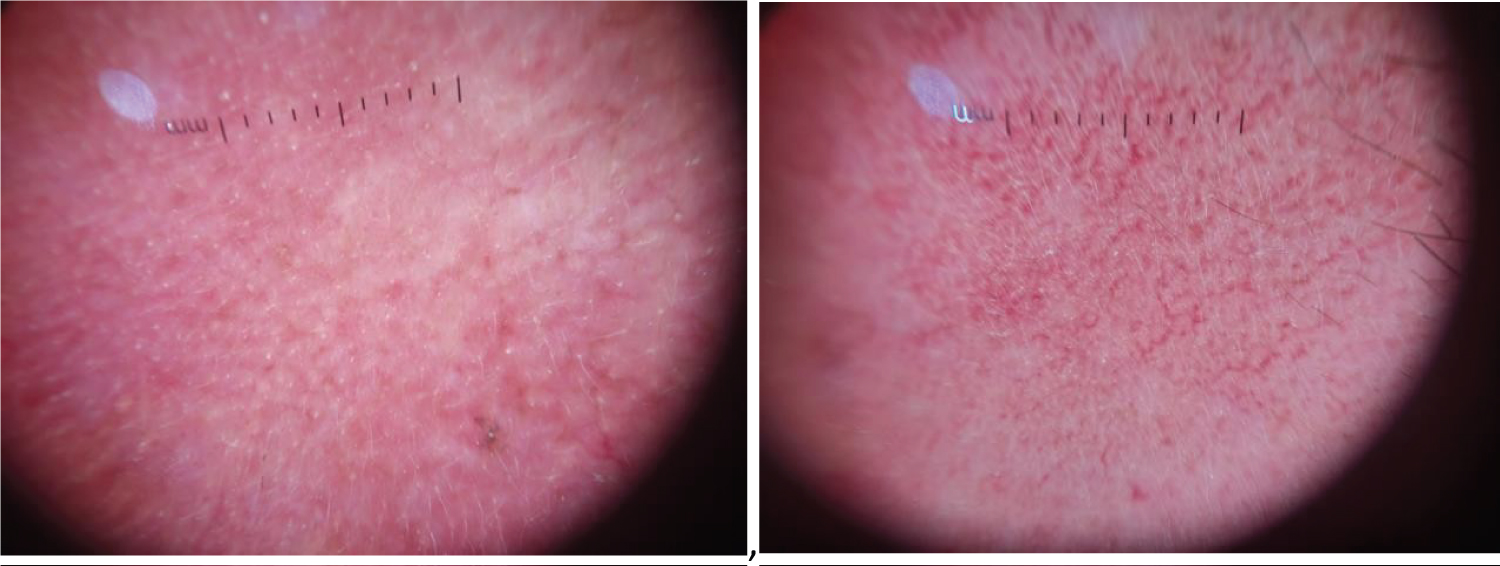 Figure 2: Presence of an erythematous background, telangiectasias, the tails of the demodex.
View Figure 2
Figure 2: Presence of an erythematous background, telangiectasias, the tails of the demodex.
View Figure 2
Rare condition considered as a subtype or late complication of rosacea. It may correspond to a particular clinico-pathological form of lymphedema [3]. Its pathophysiology remains poorly understood. Different hypotheses have been put forward. Some authors believe that the destruction of the perivascular connective tissue of the dermis, in particular elastin, leads to a loss of integrity of the vascular walls with transudation of fluids causing edema. Others suggest that mast cells present in the perivascular infiltrate play a role in the development of edema. Indeed, this edema could be secondary to the permanent obstruction of the dermal lymphatics by mast cells or linked to dermal fibrosis induced by these cells [4]. Clinically, chronic erythematous asymmetric edema of the upper two thirds of the face generally affects the forehead, glabella, eyelids, nose, and cheeks, associated with telangiectasia, facial redness, papules, pustules, nodules [5]. It poses a problem of differential diagnosis mainly with chronic lupus erythematosus, Merkelson-Rosenthal syndrome in its atypical form, dermatomyositis [6]. The histology is non-specific, the images observed are characterized by a discreet hyperkeratosis with epidermal atrophy, a discreet edema of the middle and deep dermis, an inflammatory infiltrate of lymphocytes, histiocytes and neutrophils in the perivascular and perifollicular areas, capillary dilations, edema stromal and additional features in some cases including perilymphatic granulomas, perivascular visible mast cells, chronic folliculitis, and superficial perivascular chronic inflammation, primarily comprising lymphocytes [7].
Management is difficult and not very specific. There is no definitive treatment modality or regime [8]. Several treatments have been tried: Corticosteroids, metronidazole Ketotifen, Triamcinolone injection, Retinoids, thalidomide [9], Omalizumab [3], Diuretics [5]. Blepharoplasty by CO 2 laser [10], Reduction surgery [11], some authors recommend combined treatments [12].
The particularity of our observation lies in the rarity of the pathology and especially in the therapeutic difficulties encountered.
Diagnosis and treatment of Morbihan syndrome can be difficult, due to nonspecific laboratory findings and, in most cases, resistance to clinical treatment.
Nil.
The authors declare that they have no conflicts of interest.