Molecular classification of breast cancer identified the basal like subtype, characterized by high heterogeneity and a very poor prognosis. These tumors are mainly triple negative, characterized by the expression of basal markers: CK5/6 and EGFR. In this study, we sought to investigate the features, outcome and therapeutic modalities of basal-like breast cancers (BLBC).
We retrospectively identified 90 BLBC patients diagnosed between January 2009 and December 2013 at the Department of Surgical Oncology of Salah Azaiez Institute.
The mean age of our patients was 50 years and 15.5% had a previous history of familial breast cancer. Mean tumor size was 43.8 mm. Histological examination revealed invasive ductal carcinoma in 88.9% of cases, metaplastic carcinoma in 5.6% of cases, medullary carcinoma and Adenoid cystic carcinoma in 2.2% of cases each. BLBC was most often associated with a high grade, grade III accounting for 55.3% and high Ki67 proliferative index. Vascular invasion was found in 31.1% of cases. Regarding lymph node involvement, 42.9% had positive lymph nodes and 7.9% featured distant metastases. Surgical treatment was possible in 85 patients. It consisted of conservative surgery in 40 cases and radical surgery in 45 cases. Neoadjuvant chemotherapy was administrated to 23 patients with a 13% complete pathologic response. The rates for overall survival and disease-free-survival at 3 years for localized stages were 74.4 and 75.9% respectively.
Basal-like breast cancers are aggressive tumors associated with poor prognosis. Thus, epidemiological and evolutive profile of these tumors needs to be investigated in prospective studies in order to identify novel prognostic factors and therapeutic targets.
Basal like carcioma, Immunohistochemistry, Prognosis
Breast cancer is the most common malignancy in women and second only to lung carcinoma in cancer mortality [1]. Transcriptome analyses of human breast tumors have revealed remarkably robust molecular subtypes with distinctive gene signatures and clinical outcomes [2].
Standard microarray-based transcriptional profiling is not currently feasible in the clinic. The use of immunohistochemistry to identify protein expression surrogates for gene signature of each subtype is a more practical strategy [3,4].
These intrinsic subtypes include luminal A and B, defined by the expression of genes in the luminal epithelial layer of the mammary gland, such as the estrogen receptor (ER) and its targets; human epidermal growth factor receptor2 (HER2/ErbB2), characterized by expression of the HER2 oncogene; Triple negative subtype defined by negative expression of hormonal receptors genes (ER, PR) and also lack high expression/amplification of HER2 [2]. Some Triple negative tumors express genes characteristic of the outer or basally located epithelial layer of the mammary gland, such as cytokeratins 5 and 17 and the epidermal growth factor receptor (EGFR/HER1) defining the Basal-like subtype [5].
This subtype of breast cancer is associated with an unfavorable clinical profile with a high risk of early metastatic relapse. Furthermore, Basal like tumors has currently no targeted treatment and the only validated systemic therapy is chemotherapy. Despite the use of recent patterns of chemotherapy, the prognosis remains poor. Therefore it represents a challenge in clinical practice [3].
The aim of our study was to determine the clinico-pathological, therapeutic and prognostic features associated with this type of breast cancer in the Tunisian population.
After reviewing data of the Salah Azaiez Institute of cancer, a total of 4120 breast cancer cases with complete immunohistochemical analysis was registered between January 2009 and December 2013. In this retrospective cohort study, we recruited 90 patients among 300 Triple-negative breast cancer (TNBC) patients diagnosed in this period.
We excluded from the study non-TNBC, TNBC not expressing basal markers (CK5/6) and decesced patients or those lost of sight before starting treatment. The epidemiological, clinico-pathological, therapeutic and evolutive data were analyzed.
The Basal like tumors in our study were defined by an association of RE at 0%, RP at 0%, and HER-2 not over-expressed, a score of HER-2 at 0, 1 or 2 with negative FISH. We used the TNM classification 2002 modified in 2003. TNM staging was based on pathological findings in patients who had undergone upfront surgical treatment, while it was clinical and radiologic staging in patients who had received neoadjuvant chemotherapy. Histological tumor grading was performed using the Scarff Bloom and Richardson (SBR) histological system. Sataloff and Chevalier classifications were chosen as primary endpoint to assess histological response in both the mammary gland and axillary lymphnodes.
OS was defined as the length of time from the date of diagnosis until either the date of death (regarless of cause) or the date of last follow-up. DFS was determined as the length of time from the date of diagnosis of this disease to the date of the first signs of progress confirmed by the investigator in the medical record, or the date of death or date of latest news when the patient is censored. The statistical analysis was performed by SPSS 21.0 software. Descriptive of clinical data was expressed in percentages for the qualitative variables and median or mean standard deviation for the quantitative variables, the minimum and maximum were also presented. An estimation of the global and free disease survival functions S (t) at 3 and 5 years was performed according to the Kaplan-Meier analysis and the log-rank test to estimate the outcome, with stratification of our study population into 2 groups: localized and metastatic disease.
Three hundred female patients over 4120 diagnosed and treated for breast cancer in the Department of Surgical Oncology of Salah Azaiez Institute (11.3%) were defined as having triple negative disease. Ninety patients of the triple negative samples (30%) expressed basal-like markers on immunohistochemistry.
Risk factors for breast cancer of our study population are shown in Table 1. The median age at diagnosis was 50 years and was ranging from 24 to 91 years Figure 1.
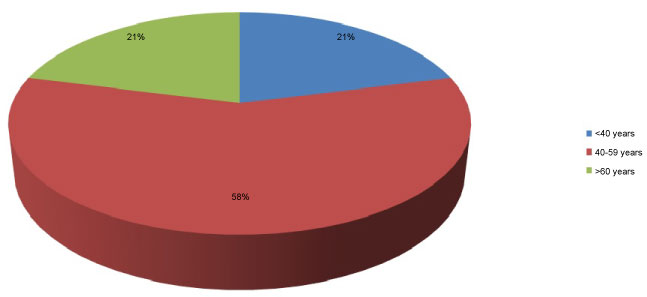 Figure 1: Population distribution by Age.
View Figure 1
Figure 1: Population distribution by Age.
View Figure 1
Table 1: Risk Factors for Breast Cancer. View Table 1
Forty-four patients were menopausal (48.9%). Fourteen patients reported having at least one-first or second-degree relative with breast cancer. The identification of BRCA mutation was not performed in any patient.
Table 2 illustrates the main clinicopathological characteristics of the study population.
Table 2: Clinical and Histopathological characteristics (90 patients). View Table 2
Combined mammography and ultrasound showed abnormalities in 97.5% of patients, of whom 72.5% had lesions that were highly suspicious of malignancy (ACR/ BI-RADS category 5: American College of Radiology Breast Imaging-Reporting and Data System category 5). Only 2.5% were shown to be probably benign lesions (ACR 3) and were then reclassified.
For the AJCC staging 10.1% were classified stage I, 53.9% stage II, 28.1% stage III and 7.9% (N = 8) were metastatic at first diagnosis. Almost half of the patients (51.1%) had a T2 tumor.
The metastases were especially visceral in first position. Bone metastases accounted for 25%.
The majority of patients (85.6%) had an infiltrating ductal carcinoma, 2.2% had medullar carcinoma, 5.6% had metaplastic carcinoma and others histologic subtypes were identified in 6.6% of cases. Tumors were poorly differentiated according to the SBR (Scarff-Bloom-Richardson) staging and presented with a high index of proliferation. In fact, Forty seven cases (55.3%) were grade III and thirty eight cases (44.7%) were grade II, with a mean Ki-67 index of 49%. Regarding lymph node involvement, 42.9% of patients had positive lymph nodes at initial diagnosis and a lymphovascular invasion was found in 31.1% of cases.
Based on the immunohistochemical study, all the tumors had triple negative-Basal like (TNBL) phenotype defined by lack of expression of the steroid hormone receptor (estrogen and progesterone) and the Human Epidermal Growth Factor Receptor-2 (HER-2) with positive staining for cytokeratin 5/6.
FISH test was needed in 12 cases to confirm the HER2 status and we found a positive expression of Androgen Receptor only in five cases.
As for treatment modalities, Eighty five patients received surgery (94.4%). Forty patients (48.8%) had conservative surgery (tumorectomy with axillary lymph nodes). The remaining patients (51.2%) received radical mastectomy with axillary lymph nodes dissection (Patey type mastectomy). All patients with local disease, who were operated, received optimal surgery with free histological margins. Twenty-three patients with advanced tumors or inflammatory breast cancer have received neoadjuvant chemotherapy before surgery. Nineteen patients (82.6%) had Anthracycline based chemotherapy and four patients (17.3%) received Anthracycline and taxane based protocol. Only three patients (13%) had pathologic complete response (PCR) to neoadjuvant chemotherapy according to Sataloff and Chevalier classification. Seventeen (25%) patients over 68 received adjuvant chemotherapy, 17 had Anthracycline based chemotherapy, 35 (51.5%) had sequential Anthracycline and taxane. Eight patients with metastatic disease received anthracycline-based regimen in the first line metastatic chemotherapy.
Radiation therapy was indicated in 69 non-metastatic patients. Palliative radiotherapy was delivered in two patients with painfull bone metastasis.
After a median follow up of 49 months, twelve among the 82 non metastatic patients experienced locoregional relapse and nineteen patients had metastatic recurrence. The maximum of recurrence occurred between the first and second year from diagnosis with a median of 21 months (Figure 2) and 24 patients died.
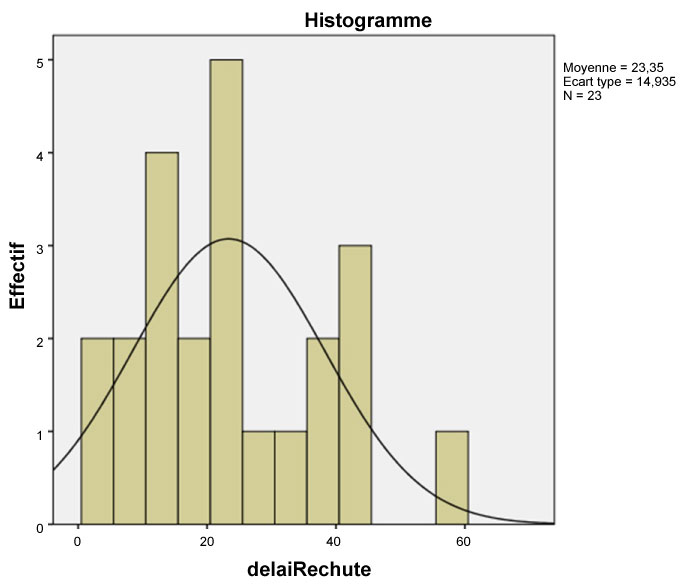 Figure 2: Population distribution by relapse period.
View Figure 2
Figure 2: Population distribution by relapse period.
View Figure 2
Six patients among the 8 with metastatic disease at diagnosis, experienced progression and two patients responded to palliative treatment with tumoral stability and than progression. All the metastatic cases died with median survival of 12.5 months (range 7-20).
Overall survival (OS) at 3 and 5 years were respectively 74.4% and 61.9% (Figure 3).
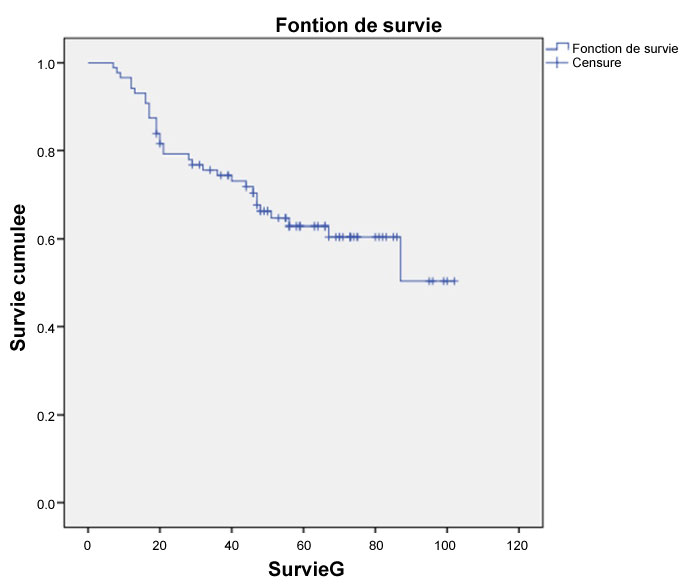 Figure 3: OS of the study population.
View Figure 3
Figure 3: OS of the study population.
View Figure 3
After exclusion of patients diagnosed at a metastatic stage OS raised to 81.9% at 3 years and 67.2% at 5 years (Figure 4).
 Figure 4: OS after exclusion of metastatic patients.
View Figure 4
Figure 4: OS after exclusion of metastatic patients.
View Figure 4
Disease Free survival (DFS) for patients with localized disease was 75.9% at 3 years and 67% at 5 years (Figure 5).
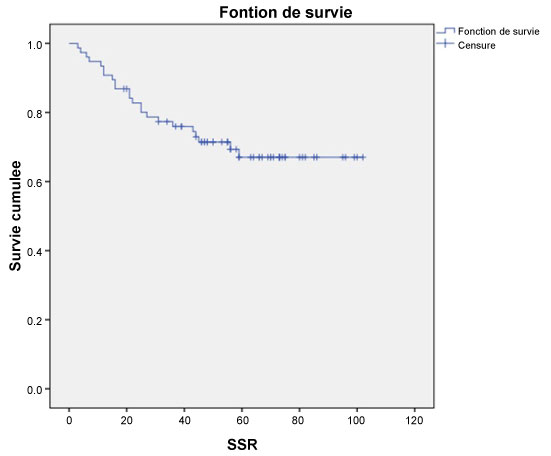 Figure 5: DFS for non-metastatic patients.
View Figure 5
Figure 5: DFS for non-metastatic patients.
View Figure 5
This study analyzed the epidemiological, clinical, and therapeutic characteristics of Basal like breast cancer in Tunisan population. Most of demographic and clinical features of our study group are in accordance with previous findings in the literature [6-9]. The frequency of TN breast cancer reported in the present work (11.3%) is consistent with literature data (10-17%) [7]. In the Chinese population, approximately 12.9% of breast cancers are TNBC [10]. However, The basal like phenotype represented only 30% of the triple negative carcinoma, which is not in accordance with literature data. In fact 80% of TNBC have a basal like phenotype (TN-BL) and the remaining 20% are defined as TN non basal like (TN-non BL) tumors [11]. Basal like carcinoma are associated with a younger age at presentation, having a mean age of 58-years-old, compared to 58-years-old for other subgroups in a study reported by Dent, et al. In our study population, the median age at diagnosis (50 years) was younger than the average age mostly reported in the United States but maybe comparable to the median age in Hispanic patients [6,9,12].
More than half of the population (59%) were 40 to 59-years-old, suggesting that there might be predisposing factors to development of this disease. Basal Like cancer occurs more frequently in premenopausal women compared with other breast cancer subtypes [13]. In the current study, patients were non menopausal in 51.1% of cases. This study found 15.5% of family history of breast cancer. Unfortunately, the research of a BRCA1/2 gene mutation was not performed due to its non availability. Given that in the literature 20% of BLBC had mutations of BRCA, the BL type maybe used as a criterion for genetic screening to improve the prognosis of this aggressive molecular subtype through a diagnosis at an early stage and the sensitivity of TN-BL breast cancer mutated BRCA1 to PARP inhibitors [3,14,15].
Clinically, BLBC patients presented large tumors with mean tumor size of 43.87 and a high rate of nodal involvement (42.9%). Rare scientific data indicate that reduced incidence of microcalcifications and peritumoral ductal carcinoma in situ (DCIS) represent typical mammographic characteristics comprise [16,17]. Consistent with its more aggressive biology, this BC subtype very often manifests itself as an interval cancer (diagnosed between screening mammograms) [18]. Histologically, BL tumors are characterized by high frequency of ductal histology (88.9%), greater histological grade (55.3%) and lympho-vascular invasion (31.1%). These results are in accordance with literature data [3,5,19,20].
Currently there is no approved targeted therapy available for BLBC. Both adjuvant treatment and palliative therapy are limited to chemotherapy. TNBC has generally higher pathologic complete response (pCR) rates than non-TNBC, and also had better survival compared to TNBC patients who don't achieve pCR [21]. The higher response rate to neoadjuvant chemotherapy may reflect the typically high tumor grade and mitotic index of BLBC [3,22]. However, it seems that only TN-non-BL tumors achieve high pCR rate [14]. In fact, in our serie PCR rate was 13% after neoadjuvant chemotherapy, based on the classification of Sataloff and Chevalier.
Prognosis for BLBC remains pejorative comparatively to other subtypes. TNBL tend to exhibit aggressive metastatic behavior [10]. These tumors respond to conventional chemotherapy but relapse more frequently than hormone receptor positive, luminal subtypes and have a high mortality rate [7]. In our series, OS was respectively 81.9% and 67.2% at 3 and 5 years. These results are similar to those described by the study conducted by Liedtka, et al. in 1118 patients over a 20-year-period (1985-2004) [23]. BLBC is also associated to a higher risk of relapse than other molecular type, especially during the first 2-3 years of follow up [24]. Dent, et al. [7] reports that the pattern of distant recurrence was different between cancer subgroups. In patients with BL phenotype, the risk of any recurrence rose sharply from date of diagnosis, peaked 1 to 3 years, and dropped quickly there after. According to Liedtka, et al. DFS at 1 and 3 years were 81 and 63% for BLBC in localized stages compared to 90 and 76% for other molecular subgroups [25]. In our study population, DFS at 3 and 5 years were respectively 75.9% and 67%.
In metastatic setting, the prognosis is extremely worse. It represented an aggressive entity associated with mortality and an according very-high-progression. BLBC has a distinctive pattern of organ specific distant metastases, with the lungs, liver, and central nervous system as the preferred sites [26].
Some authors suggested that in the BL subtype, cell cycle and DNA damage response are highly activated, and tumor cells are defects in the homologous recombination repair system. Therefore, they are vulnerable to platinum salts or PARP inhibitors [14,27]. However, we have to wait for the outcome of several current clinical studies in order to define the correct strategy for the management of BLBC [15,28,29].
Our results suggest that most BLBC characteristics in Tunisian patients are in accordance with literature data, especially concerning young age at diagnosis, high grade tumors, advanced stage at diagnosis, and short time to relapse.
This subtype carries poor prognosis and high incidence of early metastatic recurrence. Furthermore, no target therapy can be defined up to now in this subtype. Thus, identification of new target therapy and prediction of tumoral response to various treatments could help in the global understanding of patients affected by this particularly aggressive type of breast cancer.
Studies have demonstrated that the heterogeneity of BLBCs extends beyond the classic immunohistochemistry. Although several clinicopathological features have been used to discriminate between low- and high-risk patients, the identification of novel biomarkers with prognostic value remains an urgent need for improving breast cancer management.
The importance of defining groups-at-risk of BLBCs is reflected in the impact of survival-related features in clinical settings and, more importantly, in therapy response.