Hyperosmolar Hyperglycaemic State (HHS) is a diabetic emergency which requires prompt restoration of haemodynamic stability due to high early mortality. There is currently no study which recommends the use of oral hypoglycaemics to lower blood glucose levels, due to the high efficacy of parenteral Insulin. We report a case of our management of HHS using oral hypoglycaemics (Metformin and Gliclazide) due to the absence of parenteral Insulin in a rural setting, with remission of symptoms, stabilization of vitals and a significant decline in Random Capillary Blood Glucose (RCBG) levels in our patient.
Diabetes mellitus, Diabetic emergencies, Metformin, Gliclazide
Hyperosmolar Hyperglycaemic State (HHS) is one of the most serious complications that can arise in diabetes mellitus [1]. It is characterized by profound hyperglycaemia (glucose > 33 mmol/l), hyperosmolality (effective serum osmolality ≥ 320 mmol/kg), and dehydration in the absence of ketoacidosis [2].
Emergency treatment to restore haemodynamic stability is required due to high early mortality, with a reported mortality of 10-20%, which is about 10 times higher than the mortality for Diabetic Ketoacidosis (DKA) [1]. According to the American Diabetes Association (ADA) guidelines [3], treatments of diabetic emergencies include fluid resuscitation, insulin administration, and correction of underlying electrolyte imbalances and acidosis. The principle of management of adults with HHS is described in Figure 1.
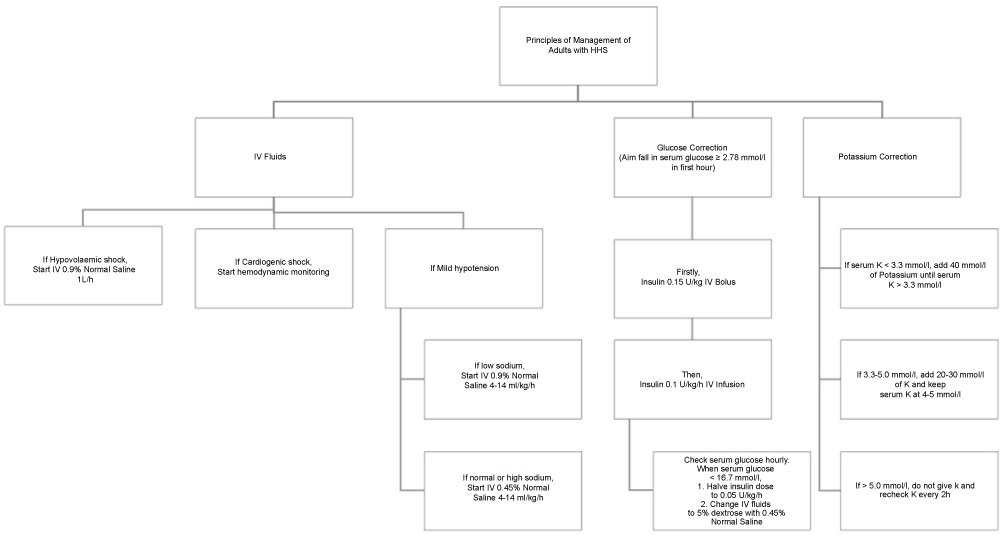 Figure 1: Principles of management of adults with HHS. View Figure 1
Figure 1: Principles of management of adults with HHS. View Figure 1
There is currently no guideline which recommends the use of Metformin and Gliclazide for treatment of HHS. We report a case of management of HHS using oral hypoglycaemics (Metformin and Gliclazide) due to the unavailability of parenteral Insulin in a rural setting.
We report a case of a 56-year-old Burmese male with history of type 2 diabetes mellitus (T2DM) and recently diagnosed tuberculosis (TB) who presented to our mobile clinic in Loon Htoe Monastery, Kalaw City with a one week history of polyuria, polydipsia, generalized weakness and bilateral blurring of vision. This is on a background of a one month history of glove and stockings distribution of paraesthesia of the limbs.
He was not taking any medication for his T2DM but was placed on anti-TB medications: Rifampicin, Isoniazid, Ethambutol and Pyrazinamide (RHEZ) two months ago. His other medical history includes hypertension.
On examination, he had dry mucous membranes, sunken eyes and diaphoresis. He also had a generalized abdominal tenderness without rebound tenderness or rigidity. Vitals were as follows: tachycardic (120 beats/min), tachypneic (20 breaths/min), hypotensive (90/69 mmHg) and Glasgow Coma Scale (GCS) of 14/15 due to confusion. Examination of other systems were unremarkable.
On further investigation, his RCBG was noted to be significantly raised at 27.8 mmol/l. Urine dipstick for ketones and serum osmolality testing were not performed due to the lack of resources in a rural setting.
Our initial differential diagnosis included HHS or DKA precipitated by the recent TB infection or the lack of diabetic medications. As such, we have decided to initiate treatment as for a diabetic emergency.
At 0 min (RCBG 27.8 mmol/l), the patient was initiated on fluid resuscitation with 1 litre of 0.9% Normal Saline IVI over 1 hour and placed on a half-hourly monitoring.
At 30 min, the RCBG level rose to 31.3 mmol/l. This was attributed to the general progression of the disease. In view of the rising blood glucose and the absence of Insulin, Metformin 500 mg PO was administered (Figure 2).
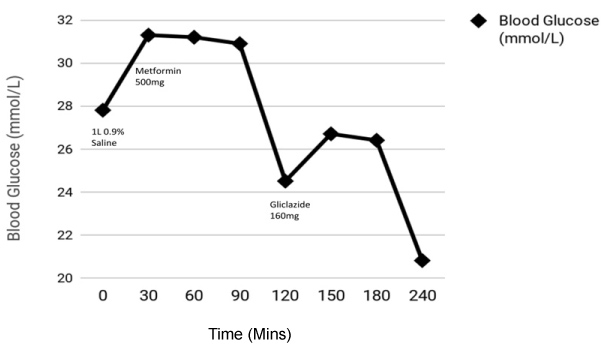 Figure 2: Graphical representation of the patient's blood glucose levels and medications administered at varying time intervals. View Figure 2
Figure 2: Graphical representation of the patient's blood glucose levels and medications administered at varying time intervals. View Figure 2
At 90 min, the RCBG level declined slightly to 30.9 mmol/l. This was attributed to the possible dilution effect of the 0.9% Normal Saline IVI, as this was before the onset of action for Metformin, which takes 90 mins.
At 120 min, the RCBG level declined significantly to 24.5 mmol/l. This was attributed to the possible effect of Metformin as this occurs after the onset of action for Metformin. In view of the still elevated glucose, Gliclazide 160 mg PO was administered.
At 150 min, the RCBG rebounded slightly upwards to 26.7 mmol/l.
At 240 min, the RCBG then dropped significantly to 20.9 mmol/l. The patient also improved very well clinically, with resolution of the symptoms and normalization of vital signs - heart rate (94 beats/min), respiratory rate (20 breaths/min), blood pressure (112/74 mmHg). The blood pressure was stabilized over a 3-hour period (Figure 3). His GCS has also recovered to 15/15. Complications of lactic acidosis: abdominal pain, fatigue and general discomfort, from the use of oral hypoglycaemics were not observed either.
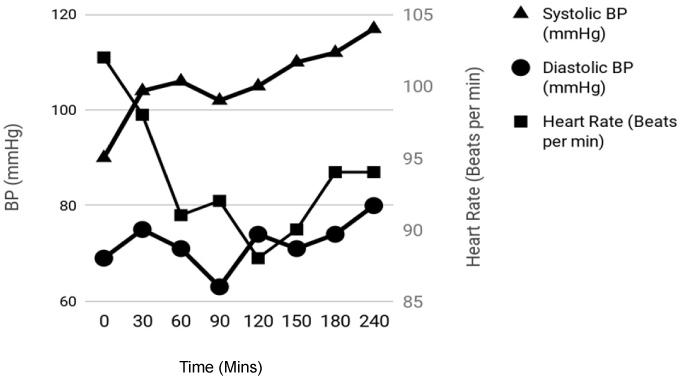 Figure 3: Graphical representation of the patient's systolic BP and heart rate at varying time intervals. View Figure 3
Figure 3: Graphical representation of the patient's systolic BP and heart rate at varying time intervals. View Figure 3
Considering the patient's significant improvement, along with the patient's refusal for further treatment at the clinic, a clinical decision was made to discharge him after a last dose of Metformin 500 mg PO, with further instruction to take Gliclazide 160 mg PO after 3 hours on the same day.
HHS is one of the most serious complications that can arise in diabetes mellitus. The ADA guidelines [3] recommend parenteral Insulin as the drug of choice to treat hyperglycaemia. Oral hypoglycaemics like Metformin and Gliclazide are not routinely used in diabetic emergencies.
There is currently no literature which measures the efficacy and safety profiles of Metformin and Gliclazide in HHS. A well-established reason behind the extensive use of parenteral Insulin is that it is not subjected to the first pass metabolism that oral hypoglycaemics undergo. Therefore, its therapeutic concentration would be easier to control and time of onset is also quicker - at 15 mins, compared to Metformin (60-180 mins) [4] and Gliclazide (120-480 mins) [5].
Furthermore, one of the rare but serious side effects of Metformin is Lactic Acidosis (LA), which could exacerbate the acidosis in DKA patients [6-8]. However, a recent 2010 Cochrane review of 347 articles showed that there was insufficient evidence that Metformin has a higher risk of LA compared to other oral hypoglycaemics in the treatment of hyperglycaemia. In fact, there were no fatal or non-fatal LA in 70,490 patient-years of metformin use [9]. Other studies have also shown that there was a low incidence of Metformin-associated LA or any mortalities from Metformin alone [10,11].
For our HHS patient, due to the lack of insulin in the rural settings and his refusal for hospitalisation, he was treated with oral hypoglycaemics Metformin and Gliclazide instead of the conventional parenteral Insulin. Despite that, we were successful in reducing his RCBG significantly from 30.9 mmol/l to 20.8 mmol/l without any complications or side effects. Notably, the time of onset of metformin of 90 min coincides with the sharp decline in RCBG from 30.9 mmol/l to 24.5 mmol/l at 120 min (Metformin was given at 30 min), suggesting that a strong correlation between Metformin and the large decline in RCBG. Additionally, the use of Gliclazide contributed to the further drop in RCBG from 24.5 mmol/l to 20.8 mmol/l (Gliclazide was given at 120 min). As such, we have shown that these oral hypoglycaemics have possibly contributed significantly to the clinical improvement of our patient.
Hypophosphatemia and hypomagnesaemia are common findings in HHS [12]. There is no evidence that treatment with phosphate infusion will benefit patients. However as these patients are often elderly and may be malnourished, thus the re-feeding syndrome could be initiated when the person starts to eat. In the case when hypophosphatemia extends beyond the acute phase of treatment of HHS, oral or IV replacement should be used. Similarly, there is insufficient evidence that magnesium replacement will provide any real benefits and should only be considered if the patient is symptomatic or has symptomatic hypocalcaemia.
However, there are some limitations to the study. Firstly, due to the lack of resources to objectively quantify the ketone levels and serum osmolality, it was not possible to definitively diagnose HHS over DKA. However, the patient had T2DM and signs of significant dehydration and confusion, which would lend weight towards the diagnosis of HHS over DKA [13].
Secondly, the patient was only observed for a short period of time (240 mins) and was discharged home with a still raised albeit significantly declined glucose level (from the highest of 31.3 mmol/l to 20.8 mmol/l). Therefore, it was not possible to ascertain if the glucose levels have eventually been normalized with the use of oral hypoglycaemics.
In summary, this discussion brings forth an important and common phenomenon in practicing medicine in a rural setting - the lack of resources. With the successful management of our HHS patient, it opens the door for clinicians to consider the use of oral hypoglycaemics in treating diabetic emergencies, especially in rural settings where resources are limited with unavailability of parenteral insulin.
In conclusion, oral hypoglycaemics like Metformin and Gliclazide are potential alternatives to parenteral Insulin in treating diabetic emergencies, especially in rural settings where resources are limited. However, further longitudinal studies will be necessary to evaluate their efficacies and safety profiles.
The authors declare that they have no competing interests.
None.
None required.
Consent was taken from the patient.
All three authors will be the guarantor for the article.