Neurocysticercosis, Taeniasis, ELISA, Headache, Seizures
DTR: Deep Tendon Reflexes; RLE: Right Lower Extremity; MRI: Magnetic Resonance Imaging; EEG: Electroencephalogram; NCC: Neurocysticercosis; IDSA: Infectious Disease Society of America; PCP: Primary Care Physician; ID: Infectious Disease; CSF: Cerebrospinal Fluid; ELISA: Enzyme-Linked Immunosorbent Assay
A 50-year-old Hispanic female presented to her primary care physician with a progressively worsening headache over a week, associated with visual disturbances, prosopagnosia and episodes of disorientation. Outpatient workup with head CT showed abnormality in the ventral aspect of the left thalamus showing 1.2 × 1 cm low density cyst with approximately 2-3 mm right-left midline shift locally. Left basal ganglia showed multiple well-defined foci of low density measuring up to 3 mm reflecting edema. On admission, pertinent physical exam findings were left sided nystagmus, positive deep tendon reflexes (DTRs) in the right lower extremity (RLE), positive Babinski on the right foot, and mild endpoint tremor dysmetria. MRI showed multiple cystic structures (Figure 1) with eccentric nodularity suggesting a scolex, with calcifications and surrounding edema (Figure 2). The largest was localized near the left anterior aspect of the third ventricle measuring 15 mm with vasogenic edema extending to left temporal lobe (Figure 3). EEG showed focal cortical disturbance (transient triphasic sharp morphology) on the left hemisphere localizing to the central temporal region, corresponding with the area of vasogenic edema and potential for epileptogenesis (Figure 4). Travel history was significant for a family vacation in Punta Cana 3 years prior, where they ate at local restaurants and street vendors. Family members also lived in close proximity, often preparing meals together. Serum antibody detection ELISA assays for Taenia solium cysticercosis (T. solium) was negative. Serum testing for Toxoplasmosis, HIV and CMV were also unrevealing. A diagnosis [1] of Neurocysticercosis (NCC) was established based on 2 Major Neuroimaging criteria: presence of cystic lesions and enhancing lesions paired with 1 Minor criteria: Clinical presentation. Treatment [2] was started as per IDSA guidelines with albendazole, praziquantel (though delayed due to lack of supply in hospital), anti-epileptic and dexamethasone. Recommendation was given for family members to be evaluated and treated upon discharge. Repeat MRI brain after one month of treatment initiation, showed a decrease to 13 mm for the largest cyst. Patient was instructed to follow up with her PCP and ID specialist for monitoring.
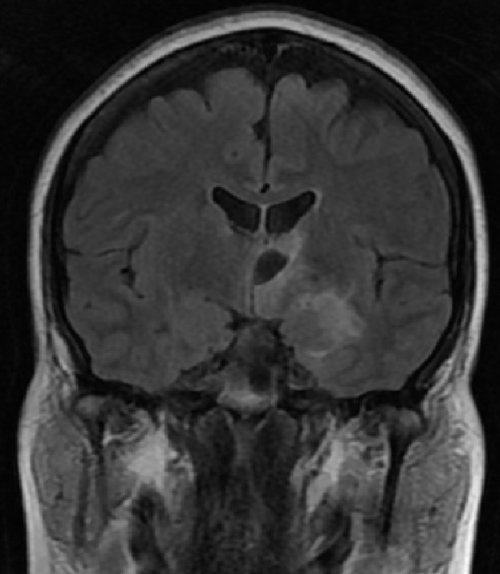 Figure 1: MRI, Coronal section showing multiple cystic lesions with surrounding vasogenic edema. View Figure 1
Figure 1: MRI, Coronal section showing multiple cystic lesions with surrounding vasogenic edema. View Figure 1
 Figure 2: Axial DWI (MRI) image: Dot sign in the left thalamus. Scolex is visible as an invagination in the cystic structure. View Figure 2
Figure 2: Axial DWI (MRI) image: Dot sign in the left thalamus. Scolex is visible as an invagination in the cystic structure. View Figure 2
 Figure 3: Axial view, T2 FLAIR (MRI) revealing a focus of low signal intensity measuring 15 mm in third ventricle. View Figure 3
Figure 3: Axial view, T2 FLAIR (MRI) revealing a focus of low signal intensity measuring 15 mm in third ventricle. View Figure 3
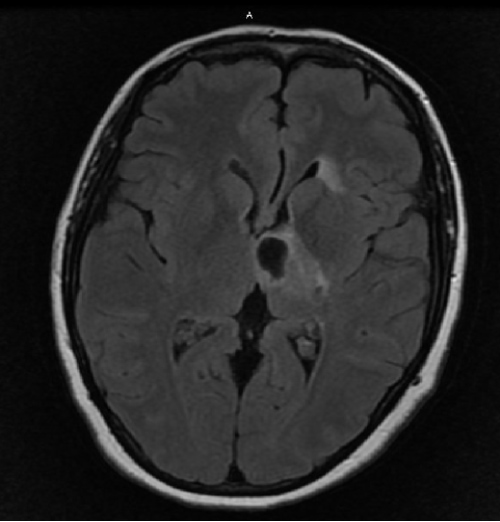 Figure 4: Axial view, T2 FLAIR (MRI) image: hypodensity surrounding the vesicular cyst is the edema. View Figure 4
Figure 4: Axial view, T2 FLAIR (MRI) image: hypodensity surrounding the vesicular cyst is the edema. View Figure 4
High on the differential diagnosis is central nervous system tuberculosis. Clinical tuberculoma arises as an early post primary infection event and typically presents as a single large, dense mass as compared to multiple cystic lesions in NCC. Oncologist also evaluated the imaging and suggested that though cancer cannot be ruled out, presence of multiple cysts with history of travel to endemic country points towards an infectious etiology.
Taenia solium infections can cause two diseases: Taeniasis and Cysticercosis. Taeniasis denotes intestinal infection with the adult tapeworm resulting from eating raw or undercooked pork containing the egg or proglottid which mature into oncospheres and finally the adult tapeworm. Cysticercosis results from fecal-oral ingestion of T. Solium egg or proglottid shed by the tapeworm. The resulting oncopheres hatch and migrate to any organ, finally forming cysticerci. Cysticercosis is endemic to Mexico, the Philippines, Central and South America, Sub-Saharan Africa, Asia, Indian subcontinent [3].
Intraventricular cysticerci are relatively rare [4] which account for only 10-20% of the cases. The symptoms may be a result of obstructive hydrocephalus from blockage occurring in the CSF drainage system. Associated symptoms are those of elevated intracranial pressure such as headache, nausea, vomiting, altered mental status, decreased visual acuity (papilledema). Seizures and focal neurological signs are less frequent in such cases. But, most cases of NCC (70-90%) present with seizures [5].
ELISA (using unfractionated antigens) should not be used, as these have performed poorly in comparative studies (both high false-positive and false-negative results) [6]. A negative serology for T. solium should not exclude the diagnosis of NCC when characteristic image findings are present [7]. In cases with multiple lesions as in our patient, the anti seizure medication should be continued for at least 24 months. Use of corticosteroid during antiparasitic therapy is associated with fewer seizure episodes [8]. Therapeutic response is important to be monitored for neurocysticercosis (a follow up MRI in this case). Repeat neuroimaging is warranted every 6 months following initial antiparasitic therapy until resolution of cystic lesion. A persistent viable or enhancing lesions on follow-up imaging warrant a repeat course of antiparasitic therapy. Improvement in neuroimaging was visible within a month of combination therapy (albendazole + symptomatic therapy) as documented in literature [9]. Screening for tapeworm infection in the stool of exposed family members and especially for family members involved with food preparation should be done to prevent new cases of cysticercosis.
In this case of NCC, risk factors for Taeniasis such as travel to endemic areas with feco-oral transmission possibly from the food handlers (family members) led to concerns of intrafamilial transmission of T. solium egg. Our patient met the diagnostic criteria by imaging (Absolute criteria) and presentation with risk factors, which allowed identify a rare disease in the United States of America, as well as a leading preventable cause of adult onset seizures.
All authors listed above have contributed equally to the case report.
This case report has been reviewed and is accepted to be presented at LMSA, Edinburgh, Texas.