Vancomycin is frequently used to treat Methicillin-resistant Staphylococcus aureus infections and has a rare side effect of thrombocytopenia. Currently, it is predominantly used in the intravenous form but other formulations are frequently used depending on the clinical scenario such as oral form and drug eluting beads. In this case report, we present a patient who developed persistent thrombocytopenia caused by vancomycin-impregnated cement beads. This patient had a hip replacement that was complicated by a septic hip joint and the elution of the vancomycin from the cement beads resulted in thrombocytopenia that was refractory to treatment and persisted for a longer duration than expected. This case report highlights the potential for non-intravenous forms of vancomycin to induce thrombocytopenia.
Vancomycin is a glycopeptide protein that is commonly used in the treatment of gram positive infections such as Methicillin-resistant Staphylococcus aureus bacteria (MRSA) [1]. Vancomycin has many common adverse reactions that include: Nephrotoxicity, ototoxicity, red-man Syndrome and neutropenia. Past literature has brought to attention Vancomycin Induced Thrombocytopenia (VIT) as a commonly missed etiology for thrombocytopenia. Clinically vancomycin has many different modalities but the majority of cases addressing VIT describe when it is used in the intravenous form [1-3]. It has been proposed that the mechanism is induced by drug-dependent anti-platelet antibodies and laboratory assays detect these antibodies (IgM, IgG) in patient's serum allowing the diagnosis of VIT. In this report we present a case in which vancomycin-impregnated cement beads used in orthopedic surgery induced thrombocytopenia [3-5].
A patient initially presented to an outside hospital (OSH) concerning for a Septic Prosthetic Hip Joint. On initial presentation, both blood and hip aspirate cultures were obtained and patient was started on intravenous vancomycin and cefazolin.
Surgical intervention was pursued, and patient underwent partial resection of the arthroplasty with retention of the femoral cemented component and beads impregnated with both vancomycin and tobramycin were placed. During the admission, patient platelet count sharply decreased to 3,000/μL prompting transfer for higher level of care, and prior to transfer patient antibiotics were narrowed to daptomycin after cultures resulted for Methicillin-resistent Staphyloccus aureus (MRSA). On arrival to our institution, patient was afebrile, platelet count 1,000/μL, vancomycin trough 17.9 μg/mL and imaging of the patient's hip demonstrated the presence of the impregnated beads (Figure 1). The peripheral smear did not show schistocytes or platelet clumping, and coagulation studies were normal. On infectious workup, both HIV and hepatitis panel studies were negative, and IgG positive Helicobacter pylori (H. pylori). Heparin Induced Thrombocytopenia (HIT) was not pursued because patient never received any heparin products. There was a concern for Drug Induced Thrombocytopenia (DIT) and serology was sent for vancomycin antiplatelet antibodies which was positive for IgM antibodies. Patient was treated with Intravenous Immunoglobulin (IVIG) but had no improvement and pulse dose dexamethasone was then administered. Patient responded but platelet count declined after the steroid regimen was completed. Patient was given a second course of pulse dose steroids with minimal improvement, but counts remained relatively stable. Repeat imaging of patient's hip revealed smaller quantity of beads (Figure 1), indicating that the beads were eluting, supported by a vancomycin trough of 0.17.
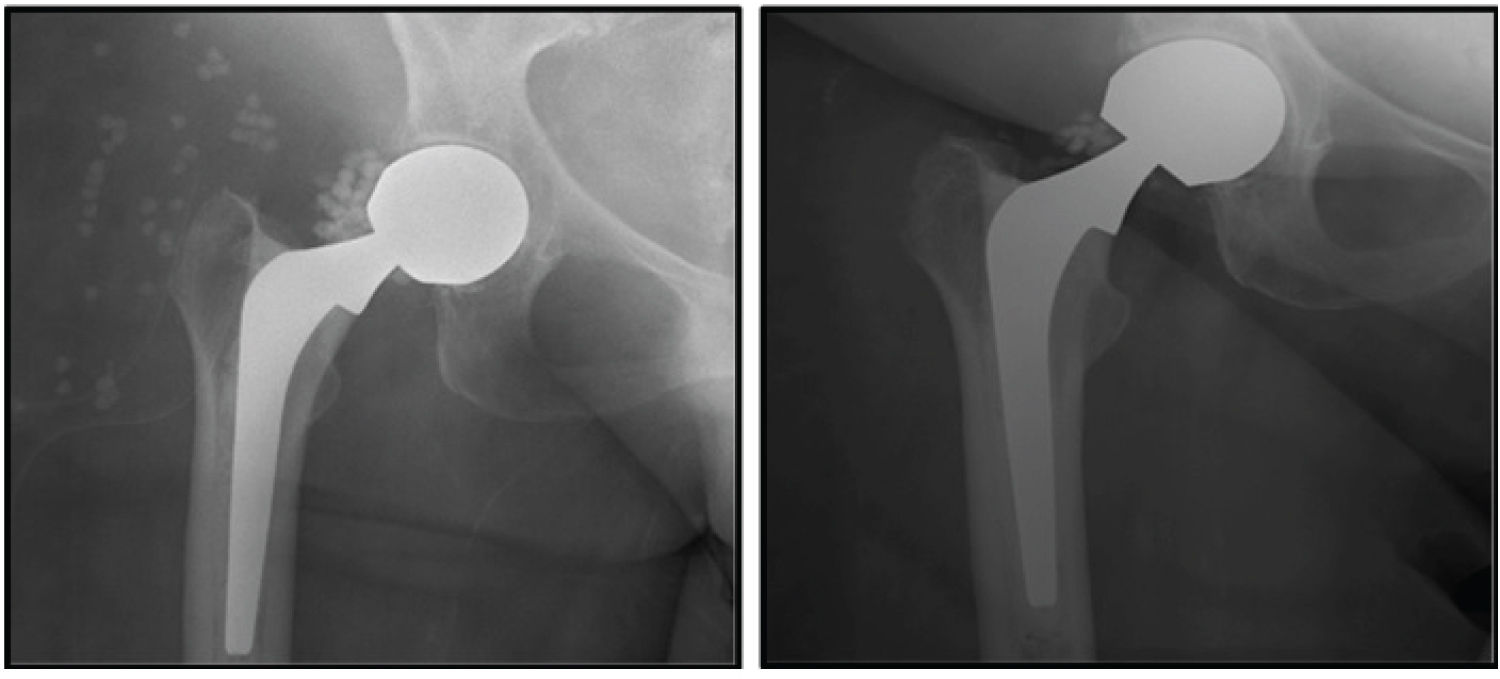 Figure 1: The X-ray on the left illustrates the right hip prosthesis and numerous impregnated beads (represented by the circular opacities) can be seen. On the repeat X-ray of the right hip, a significant decrease in beads can be appreciated. View Figure 1
Figure 1: The X-ray on the left illustrates the right hip prosthesis and numerous impregnated beads (represented by the circular opacities) can be seen. On the repeat X-ray of the right hip, a significant decrease in beads can be appreciated. View Figure 1
This case discusses a patient with vancomycin-induced thrombocytopenia associated with vancomycin-impregnated cement beads. Patient's thrombocytopenia was treated with IVIG, but had inadequate response. For ITP, it is expected that the platelet count would increase in response to IVIG within 24-48 hours [6]. However, the clinical course of the patient and positive IgM vancomycin antibodies pointed to vancomycin being the likely culprit for the thrombocytopenia.
Typically, for a patient with no prior exposure to vancomycin, previous studies have demonstrated a decrease in platelet count by 93% that occur after 6 days of vancomycin administration [2]. When VIT is recognized and vancomycin administration is stopped the platelet count gradually recovers with resolution of thrombocytopenia in approximately 7 days [7]. In some cases in which a patient was previously sensitized to the medication, the platelet count can decrease rapidly within 2 to 3 days [7]. With regards to this patient, the platelet count decreased rapidly within three days indicating that patient was likely exposed to vancomycin previously - resulting in sensitization [8]. As a result, when the intravenous formulation was administered there was significant decrease. It should be expected that the platelet count gradually improves after cessation of intravenous-vancomycin but it remained below baseline for a longer duration of time than expected. Given that had a small quantity of vancomycin that remained measurable, it is likely that the vancomycin beads eluted small quantities of vancomycin resulting in a detectable level after the IV formulation was stopped. When determining the best treatment for vancomycin induced thrombocytopenia, the most important factor is vancomycin cessation [1,7]. For this patient, the risk of removing the vancomycin source was not achievable immediately given the route of administration. One of the main criticisms of the case report is that the patient's platelet count was not trended from the nadir back to baseline. However given the specificity for patient's positive vancomycin IgM antibodies, VIT is the most likely diagnosis.
Within recent time, more information has come to light about VIT. Most recent papers regarding the route of administration has been via intravenous route. In the literature, VIT has been reported in cement infused orthopedic equipment [9], but there paucity in the literature and given the rarity of these cases, it should remain in the differential diagnosis, as it is possible small concentrations can elute into the serum resulting in thrombocytopenia as its counter-part with IV formulations.
None.
No financial conflicts of interest.
All authors have had equal contribution to this submission.