A scarcity of literature exists on papillary muscle hypertrophy. The reported incidence of 0.4% is based on a single study of 6731 patient echos that were reported in 1990. The importance of this condition is substantial as patients are often asymptomatic and it has been postulated as a potential cause of sudden cardiac death. A 43-year-old lady presented to our care that had an incidental finding of papillary muscle hypertrophy in the context of chronic rheumatic mitral valve disease. The clinical significance of this rare condition is based on the foundation of a high quality cardiac MRI study to differentiate a myriad of causes.
Papillary muscle hypertrophy is defined as a diameter in the horizontal or vertical axes of > 1.1 cm in either one or both of the papillary muscles [1]. A scarcity of literature exists on papillary muscle hypertrophy and the reported incidence of 0.4% is based on a single study of 6731 patient echos reported in 1990 [1]. The disorder is described as a variant of hypertrophic cardiomyopathy, a consequence of chronic rheumatic mitral valve disease and glycogen storage disorders [2]. We present a case of a young woman with rheumatic mitral valve disease and an incidental finding of papillary muscle hypertrophy.
A 43-year-old lady presented to a peripheral hospital with a right lower limb swelling diagnosed as compartment syndrome. She was transferred to the Mercy University Hospital under the care of the vascular surgical team for fasciotomy. During examination she had a right iliac fossa mass. A CT abdomen/pelvis was performed to evaluate this finding with particular focus on iliac vein drainage to rule out an iliac vein DVT.
A 21 mm low attenuation filling defect was incidentally found in the left ventricle, abutting on the mitral valve. Two "metallic" density artefacts were seen adjacent to this at the left ventricular aspect of the septum suggesting prior cardiac intervention. At this point a working diagnosis of adherent thrombus was proposed.
We discovered that she had a background history of Wolff Parkinson White syndrome with prior catheter ablation of the bundle of Kent. She also had a history of extensive travel in childhood and of rheumatic heart disease affecting the mitral valve with mild mitral stenosis on a most recent echo carried out 2 years prior. She had no family history of sudden cardiac death, hypertrophic cardiomyopathy (HCM) or other genetic disorder. Her inpatient ECG was sinus rhythm with a left atrial abnormality.
She had an echocardiogram carried out during her admission which showed unusual hypertrophy of the postero-medial papillary muscle (Figure 1). This measured 1.45 cm × 1.98 cm. There was no focal hypertrophy of any of the other segments of the left ventricular wall. There was heavy nodular calcification of the left ventricular cordae tendinae at the basal septum which explained the "metallic" density artefacts on CT. She had mild to moderately thickened mitral valve leaflets with a rheumatic appearance. There was a moderate anteriorly directed mitral regurgitant jet.
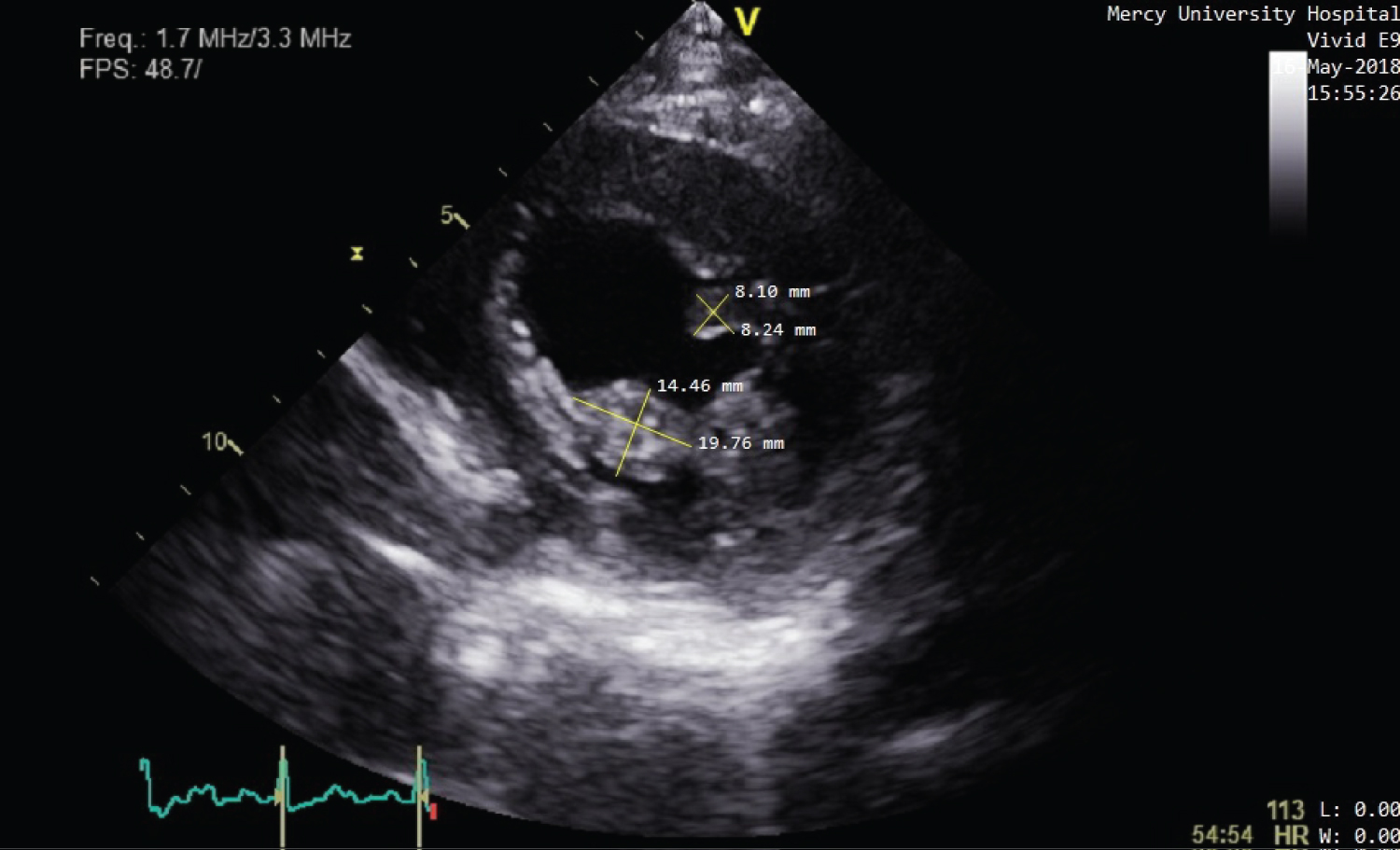 Figure 1: Echocardiogram showing parasternal short axis view of the left ventricle at the level of the papillary muscles. The posteromedial muscle is 1.98 cm × 1.45 cm and for comparison the anterolateral muscle is 0.82 cm × 0.81 cm. View Figure 1
Figure 1: Echocardiogram showing parasternal short axis view of the left ventricle at the level of the papillary muscles. The posteromedial muscle is 1.98 cm × 1.45 cm and for comparison the anterolateral muscle is 0.82 cm × 0.81 cm. View Figure 1
In order to rule out an unusual form of HCM cardiac MRI was performed. Again there was hypertrophy of the postero-medial papillary muscle with a diameter of 1.1 cm. There was no gadolinium enhancement. There was mixed mitral stenosis/regurgitation and the mitral valve leaflet had a rheumatic appearance.
The plan was conservative management with imaging surveillance of her mitral valve stenosis/regurgitation and annual follow-up in cardiology outpatients. One would anticipate that in the future she may require a surgical valve replacement as the level of calcification involved in the mitral apparatus even at this stage is significant.
Isolated papillary muscle hypertrophy has seldom been documented in the literature. It has been described as a variant of (HCM) with hypertrophy of the papillary muscles in the absence of typical eccentric LV hypertrophy [1]. It has been associated with chronic rheumatic mitral valve disease and is also quite rare [3]. However, reports of the association of papillary muscle hypertrophy in the setting of rheumatic heart disease are rare in contemporary literature, most likely reflecting the decreased prevalence of this condition.
In our patient the presence of rheumatic valve disease and absence of family history of HCM would suggest the former as a cause. Also, by carrying out a cardiac MRI we demonstrated absence of myocardial fibrosis as is frequently found in patients with HCM. Furthermore, her ECG showed no typical features of HCM. Furthermore there were no giant negative T waves or U waves that have been associated with posterior papillary muscle hypertrophy [4].
The pathophysiology of papillary muscle hypertrophy, related to rheumatic valve disease, is thought to be as a result of derangement of the valve apparatus. The stress that this exerts on the papillary muscles may account for hypertrophy over time [3].
Papillary muscle hypertrophy that is isolated to a single papillary muscle is unusual, and one can only hypothesise that the presence of nodular calcification adjacent to the affected papillary muscle may be causative, or reflective of a common pathophysiology. As mentioned above, they may reduce the compliance of the associated corda tendina, placing excessive strain on the postero-medial papillary muscle.
Although she had no findings on her ECG, an important learning point echoed by this case is that patients with papillary muscle hypertrophy may not fulfil ECG criteria for LVH [5]. Solitary papillary muscle hypertrophy has been associated with increased risk of sudden cardiac death [6]. This may be due to dynamic LV pressures, as demonstrated in a case report by Sung, et al. [7] where the subject exhibited papillary muscle hypertrophy without typical HCM features.
Very few cases of rheumatic mitral valve with associated papillary muscle hypertrophy have been reported and little is known about how the condition behaves in the long term. Papillary muscle hypertrophy is most often discovered incidentally. It has been linked to an increased risk of sudden cardiac death and may be elusive as patients are asymptomatic and can have a normal ECG. Importantly HCM as a cause must be ruled out and thus patients should have a cardiac MRI to look for myocardial fibrosis.