Susac Syndrome is a rare auto-immune endotheliopathy that rarely presents with the full triad of branched retinal artery occlusion, encephalopathy and sensorineural hearing loss. The diagnosis of Susac can be a challenge due to the variability in presentation, course and severity of disease.
Diagnosis of Susac requires a careful history, diagnostic procedures such as fluorescein angiography, audiometry and MRI, and most importantly - interdisciplinary teamwork, all of which aid in the diagnosis of this rare disorder.
A 38-year-old female with no cardiovascular risk factors developed sudden vision loss in the left eye. Extensive evaluations were negative thus prompting the diagnosis of amaurosis fugax. A few days later, she began experiencing flickers in the left eye with new onset blurring of vision in the right eye that progressed to loss of vision after 3 months, with associated headaches, paresthesias of the lips and extremities, and increasing fatigue. There was no loss of hearing.
Retina fluorescein angiography revealed multiple occlusions, hyper fluorescence and leakage from the retinal branches. MRI FLAIR sequence demonstrated several hyperintense lesions in the corpus callosum, corona radiata and centrum semiovale. After collaborative efforts, Susac Syndrome was entertained, and our patient received immunoglobulin and rituximab after relapse on pulsed methylprednisolone, with marked resolution of symptoms.
Only a small percentage of patients will present with the triad, however, it is most common to see only 2 out of the 3 as exemplified in our case. Collaborative efforts are required to come to a quick diagnosis. Excellent recovery is expected once diagnosis is made, and patients are commenced on immunosuppressants.
Susac syndrome, Diagnosis, Collaboration
Susac syndrome, first described in 1979 by Dr. John Susac, is a rare, immune-mediated microangiopathy that can cause stroke. The disease is characterized in its classic form by a triad of encephalopathy, branch retinal artery occlusion and low frequency sensorineural hearing loss [1]. The diagnosis can be challenging due to the variability in presentation, course and severity of the disease. Interdisciplinary collaboration is often required for rapid diagnosis and rapid immunosuppressant treatment to prevent irreversible damage in the organs involved.
A healthy 38-year-old woman presented initially to the ophthalmologist on account of sudden visual impairment in her left eye. She had no known illnesses and no known risk factors for visual loss. No complaints of hearing loss. Initial ophthalmologic assessment included visual field and fundoscopic examinations which were normal. Amaurosis fugax was considered and she was transferred to the neurological department for further assessment and work-up. Aside for impaired vision in the left lateral upper quadrant, the clinical examination was normal. All investigations were unremarkable, including - blood tests, ECG, Doppler ultrasound of the neck vessels and MRI stroke protocol.
About a week later, the patient experienced a new episode of blurred vision and flickering in the left eye followed by a mild headache. After 3 months, she presented again to the ophthalmologist with new loss of vision in the upper segment of the right eye. There were associated almost daily episodes of visual disturbances, paresthesia of the lips and intermittent paresthesia of the extremities with increasing fatigue. The symptoms impaired her activities of daily living. Eye examination now showed a deficit in the right upper field of vision of the right eye. Funduscopic examination revealed a pale retina on the lower right quadrant of the right eye which is compatible with infarction (Figure 1). There was lack of arterial filling and segmented blood vessels. Similar findings were also evident in the left eye. The diagnosis of branch retinal artery occlusion of the right eye was made and Aspirin 75 mg x 1, and Dipyridamole 200 mg HS was started. She was again referred to the neurologist and cardiologist to determine the aetiology. Neurological examination was again normal except for subjective fluctuating symptoms of paresthesia, blurred vision and photopsia. MRI at this time revealed multiple small changes in both hemispheres compatible with micro-infarcts of different ages (Figure 2). Further workup was directed towards ruling out usual causes of stroke in young adults; Cardiac embolic source, thrombotic tendency, and vasculitis. All investigations were normal except for slightly elevated spinal protein of 0.8 g/L and serology compatible with a recent cytomegalovirus (CMV) infection. The patient continued to experience persistent fatigue and episodes of photopsia, paresthesia and dizziness despite treatment with ASA, Dipyridamole and a short period with heparin. A fluorescein angiography of the right eye showed several occluded artery branches both peripherally and temporally, hypoperfusion and an occlusion medially (Figure 3a), while hyper-fluorescence and leakage was seen in the vessel wall from the superior temporal retinal arteriole of the left eye (Figure 3b). New MR T2 FLAIR sequences showed multiple small hyperintense lesions in the corpus callosum, corona radiata and centrum semiovale (Figure 4). Based on these findings, the diagnosis of probable Susac syndrome was considered. The patient was initially pulsed with high doses of intravenous methylprednisolone with initial improvement but then relapsed after 4 weeks while on oral prednisone. She was then switched to Immunoglobulin infusion and started on Rituximab with remarkable improvement.
 Figure 1: Funduscopic examination showing a pale retina on the lower right which is compatible with infarction.
View Figure 1
Figure 1: Funduscopic examination showing a pale retina on the lower right which is compatible with infarction.
View Figure 1
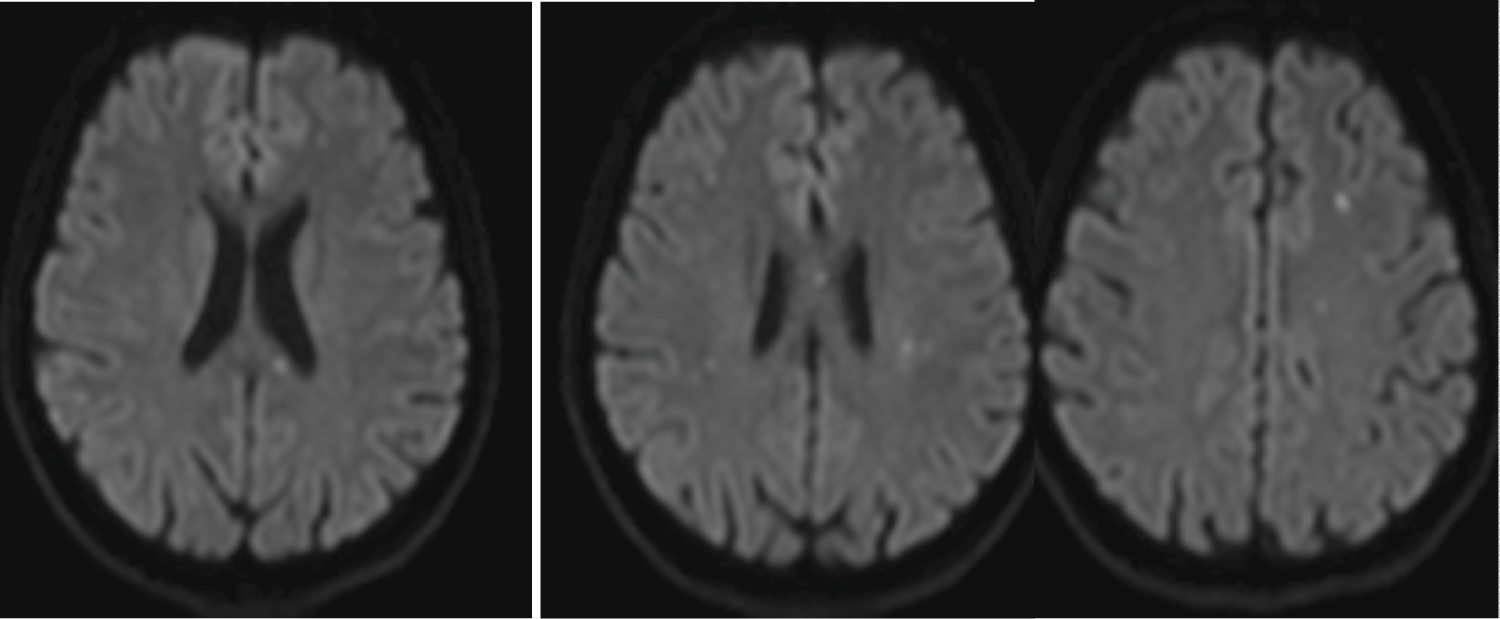 Figure 2: MRI DWI sequence demonstrating micro-infarcts of different ages in both hemispheres.
View Figure 2
Figure 2: MRI DWI sequence demonstrating micro-infarcts of different ages in both hemispheres.
View Figure 2
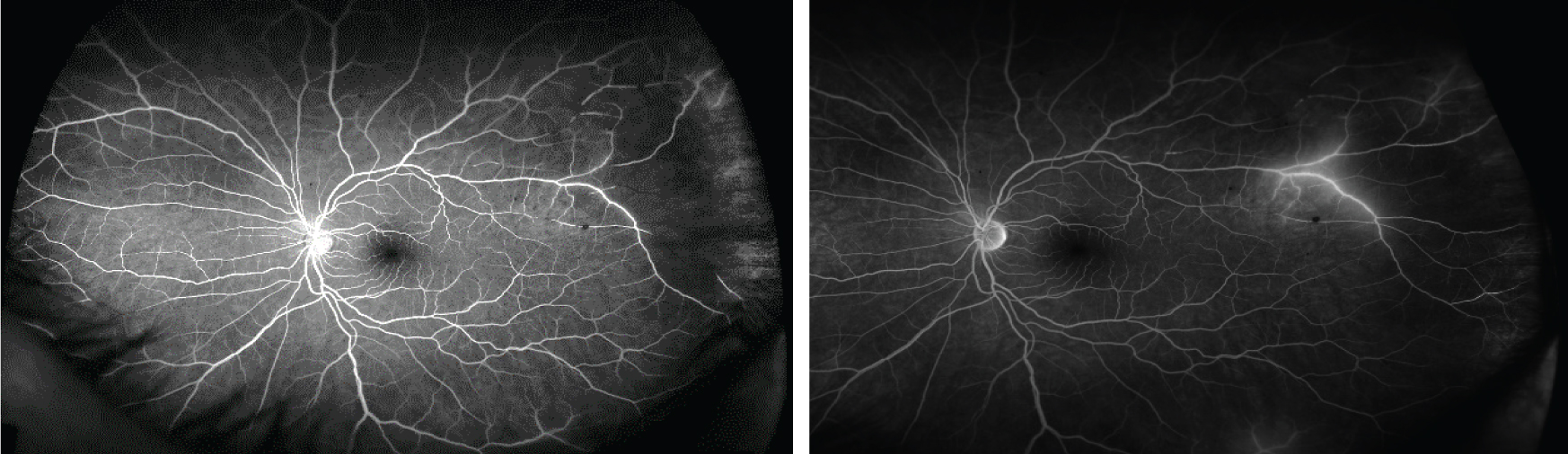 Figure 3: (a) Fluorescein angiography of the right eye revealed several occluded artery branches both peripherally and temporally in the upper eye, as well, hypoperfusion and an occlusion medially; (b) Hyperfluorescence in the vessel wall and leakage from the superior temporal retinal arteriole of the left eye.
View Figure 3
Figure 3: (a) Fluorescein angiography of the right eye revealed several occluded artery branches both peripherally and temporally in the upper eye, as well, hypoperfusion and an occlusion medially; (b) Hyperfluorescence in the vessel wall and leakage from the superior temporal retinal arteriole of the left eye.
View Figure 3
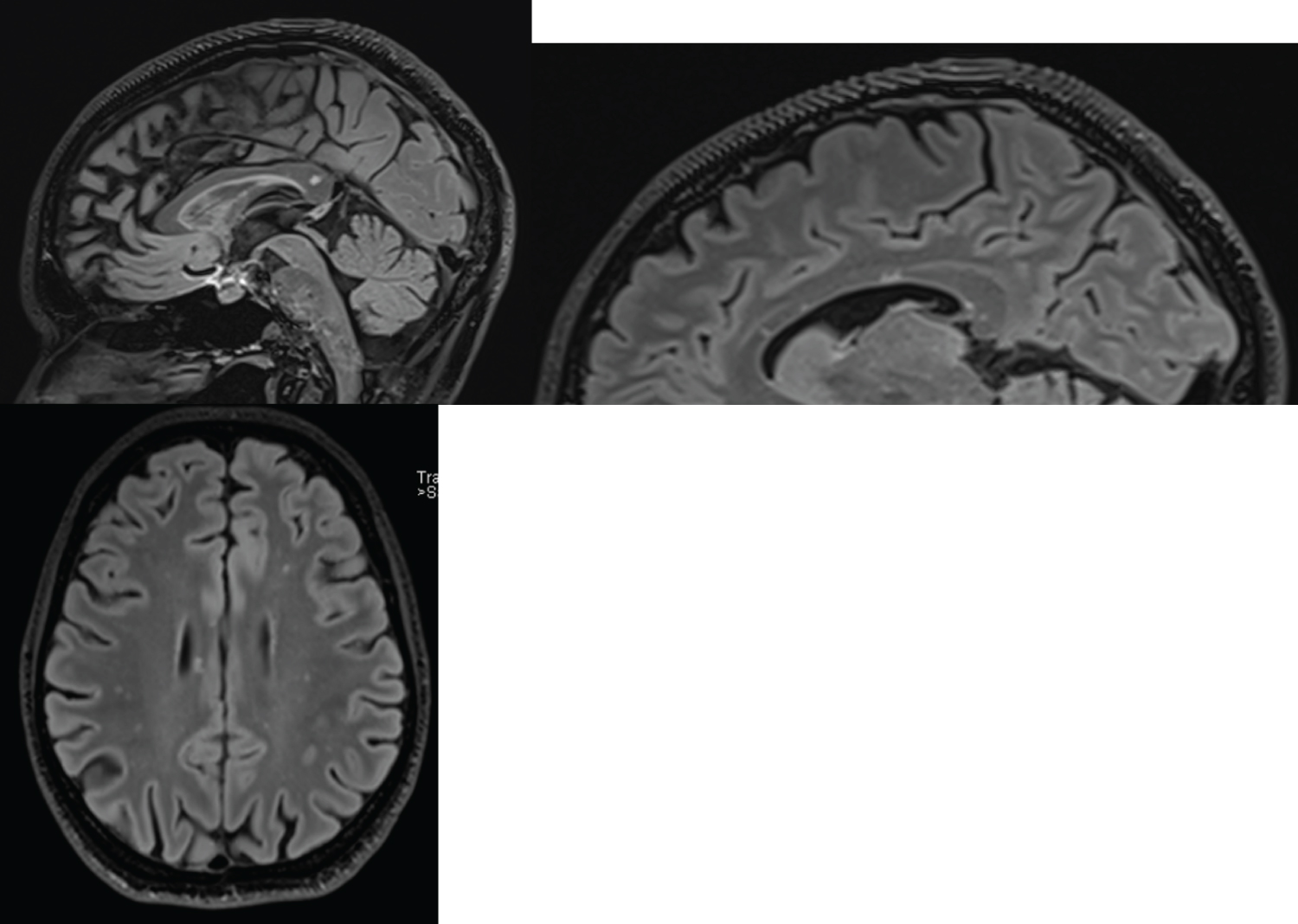 Figure 4: MR T2 FLAIR with multiple small hyperintense lesions in the corpus callosum, corona radiata and centrum semiovale.
View Figure 4
Figure 4: MR T2 FLAIR with multiple small hyperintense lesions in the corpus callosum, corona radiata and centrum semiovale.
View Figure 4
Susac syndrome particularly affects young people between the ages of 20-40, with a predominance of women and is a rare cause of stroke. With only about 400 cases of SUSAC reported worldwide, this uncommon but possibly underdiagnosed disease can present with a typical triad of- neurologic signs, branch retinal artery occlusion and sensorineural hearing loss [1-3]. However, less than 15%-20% of cases have all three symptoms at presentation [2-4]. Our patient presented with only 2 features (visual and neurological), this can make the diagnosis quite difficult. Given the complexity of skills required to make a proper diagnosis, interdisciplinary teamwork is required.
Neurologic signs can be fluctuating headache, fatigue, dizziness, cognitive dysfunction, behaviour changes, paresthesia and possibly paralysis and seizures [1]. These symptoms are accompanied by T2 FLAIR parenchymal enhancement showing small multifocal "snowball" lesions typically found in the corpus callosum with or without leptomeningeal enhancement [1-3] [5]. Eye symptoms consist of visual field loss and other visual disturbances such as flashes of light or photopsia, flickering or colour spots. Fluorescein angiography shows occlusion of small retinal branch arteries and enhancement of the artery wall near the obstruction. Though CMV serology was positive in our patient and CMV infection of the eyes may present with floaters and vision loss. Fundoscopic examination did not reveal the classical 'pizza pie' appearance and relative afferent pupillary defect, and she did not have any clinical features to suggest immunosuppression [6]. Vestibulocochlear symptoms are in the form of hearing loss, tinnitus or dizziness accompanied by pathological audiogram or vestibular tests. Our patient had 2 of the 3 features and this is the most common type of presentation [1,2,5]. In our case, the patient was initially diagnosed with possible Migraine with Aura, thereby delaying treatment. Given the varied presentation of Susac and the involvement of different organs, a multi disciplinary approach is recommended when Susac is suspected [7]. Interdisciplinary cooperation between Neurology, Ophthalmology and ENT may help come to a quick diagnosis [7]. The pathology behind Susac is thought to be caused by an autoimmune inflammatory response on the endothelium of small blood vessels, with edema of endothelial cells, leakage, thrombus formation and possible micro infarcts [1,3,6]. This is supported by the fact that in many patients, autoantibodies to endothelial cells can be found in the serum. It is speculated that the disease can sometimes be triggered by a viral infection [4].
The disease is perceived as self-limiting within a few years, but the exact duration is difficult to predict. Relapses have been seen after several years [3,5,8]. Sequelae are common, such as fatigue, cognitive impairment, paresis, hearing and vision loss [3,8].
However, early and aggressive immunomodulatory treatment provides a good prognosis [2]. Treatment recommendations are based on clinical experience and observational studies, there are no randomized controlled trials [3,5,8]. Most experts agree that treatment should be early, aggressively and for a long enough period to prevent relapses. The first choice in treatment is high-dose steroids, but some patients do not respond well enough, as seen in our case, therefore, additional treatment is recommended [4,5]. It must be emphasized that patients need to be followed closely to detect treatment failure and the consequent permanent sequelae. Most people recommend intravenous immunoglobulin in case of disease breakthrough on steroids with treatment being given each month over a period of time. Possibly combined with other immunomodulatory agents such as Azathioprine, Mycophenolate Mofetil, Cyclosporin A, Rituximab and/or cyclophosphamide [3,5,8,9]. In very rare cases in which there is severe, refractory disease which does not respond to treatment, hematopoietic stem cell transplantation has been done with success [9]. As well, it is recommended to give Aspirin [5].
Susac syndrome is a rare autoimmune disease that can cause damage in the brain, retina and cochlea of young patients. Although only a small percentage of patients present with involvement of all 3 organs. A careful history, interdisciplinary teamwork with diagnostic procedures such as fluorescein angiography, audiometry and MRI can aid diagnosis. Optimal outcome requires rapid and complete disease suppression with immunosuppressants and close follow-up. All treatment recommendations are based on expert opinions due to the lack of randomized controlled trials.
None declared.
None declared.