Background: Colorectal cancer is very rare in children. Therefore, the diagnosis is generally established at advanced disease. This is a presentation of two cases of colorectal treated at Habib Bourguiba Hospital University.
Case presentation: Two adolescents, 14-year-old and 16-year-old were treated for CRC between 2006 and 2022 in our department. Both complained about abdominal and pelvic pain few months ago. The first patient, with no personal or family history of digestive pathology, was admitted for peritonitis. The exploration noted advanced rectal tumor, peritoneal carcinomatosis and bone metastasis. She had one cycle of palliative FOLFIRI chemotherapy and died. The other one was admitted for complicated appendicitis. Per operative exploration noted localized sigmoid tumor which was resected. She had 12 cycles of adjuvant FOLFOX chemotherapy and she was alive and free failure for 13 years. Her paternal uncle had yet rectal cancer at 40 years and her father developed later metastatic colon cancer. Lynch syndrome was established.
Conclusions: Colorectal cancer is rare in children. It can be sporadic or hereditary cancer. Diagnosis is often tardive. The prognosis is tightly correlated to stage so any children presenting with chronic pain in abdomen with doubtful history of constipation and rectal bleeding should be carefully examined.
Cancer, Colorectal, Children, Genetic factors, Sporadic
Gastrointestinal malignancies are rare in children and represent 2-5% of all children cancer [1,2]. Colorectal (CRC) cancers are the most common primary solid malignancy of the gastrointestinal tract among children, with annual incidence of about one in 10 million adolescents younger than 20 years old [3,4]. The disease is usually advanced at presentation and the prognosis is poor. Matched for stage, the prognosis of patients with young-onset CRC is similar to older patients [5]. We present two cases of colorectal in adolescent with different stages and different outcomes. The clinical presentation, diagnosis and treatment of colorectal cancer in children are also reviewed.
Two adolescents, 14-year-old and 16-year-old were treated for CRC between 2006 and 2022 in the medical oncology department, Habib Bourguiba Hospital University in south of Tunisia.
She was a fourteen-year-old girl. There was no history or family history of gastrointestinal problems. She suffered for paroxysmal abdominal pain since 3 months ago, general condition was moderate and marked by asthenia and weight loss. Clinical exam noted left inguinal lymph node. A scan was done in her region. It showed a non-stenosing circumferential thickening of the middle rectum extended to the recto-sigmoid hinge without digestive distension upstream (Figure 1, Figure 2 and Figure 3).
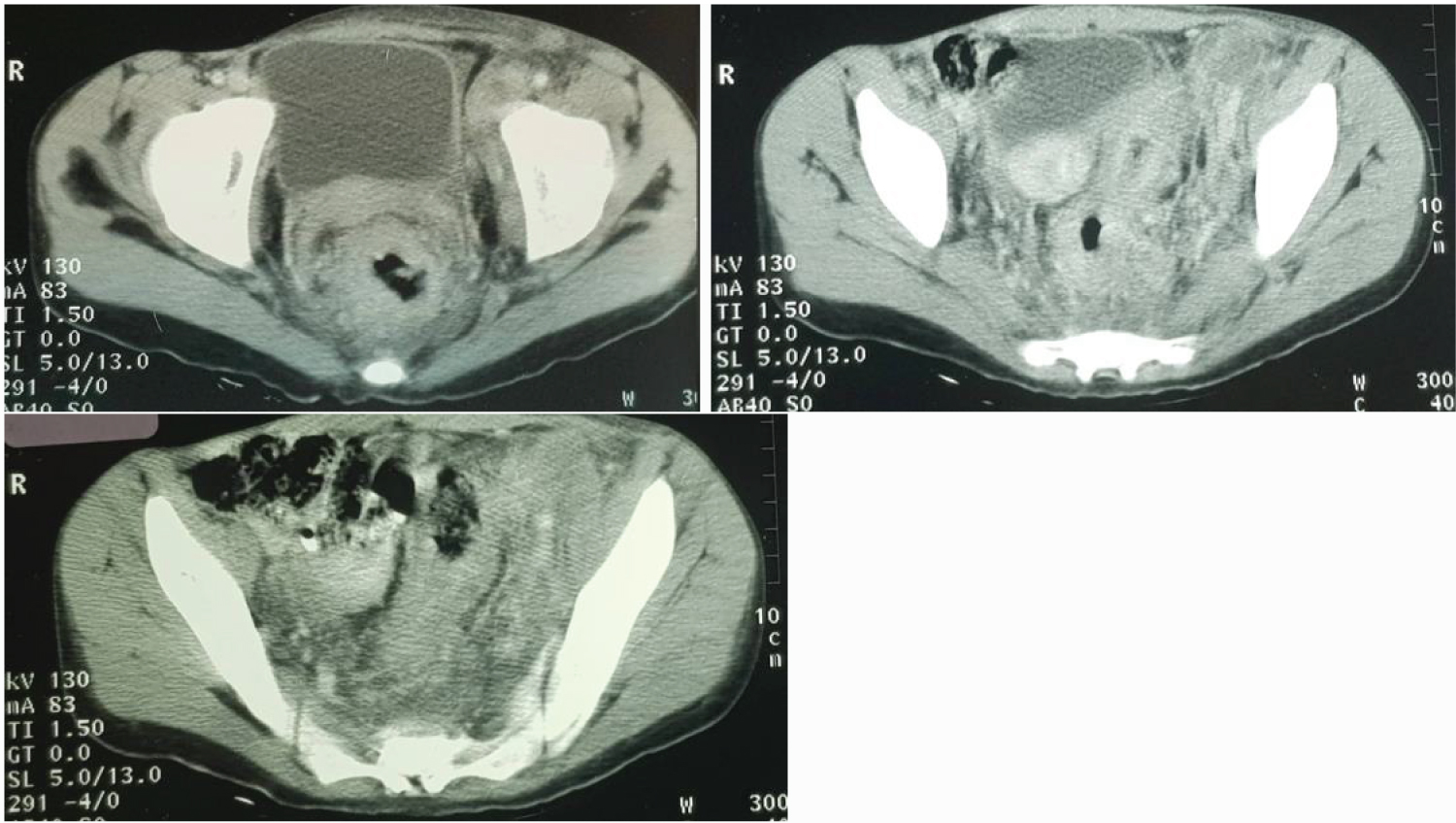 Figure 1,2,3: Cross sectional CT scanning demonstrating a non-stenosing circumferential thickening of the middle rectum extended to the recto-sigmoid hinge without digestive distension upstream.
View Figure 1-3
Figure 1,2,3: Cross sectional CT scanning demonstrating a non-stenosing circumferential thickening of the middle rectum extended to the recto-sigmoid hinge without digestive distension upstream.
View Figure 1-3
Left inguinal adenopathy 's biopsy revealed inflammatory tissue without malignant cells. One month later, she was addressed to our hospital for peritonitis. Scan noted recto- sigmoid tissue stenosing thickening with upstream colic distension, digestive perforation, and abscessed peritonitis (Figure 4 and Figure 5).
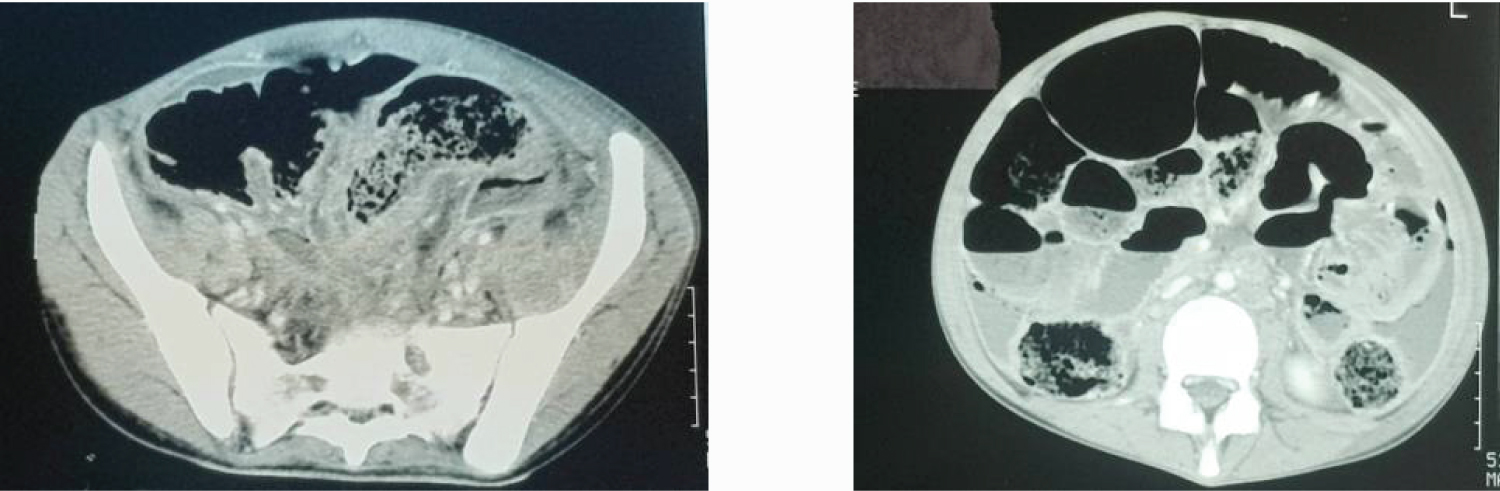 Figure 4,5: Cross sectional CT scanning demonstrating recto-sigmoid tissue stenosing thickening with upstream colic distension, digestive perforation, and abscessed peritonitis.
View Figure 4-5
Figure 4,5: Cross sectional CT scanning demonstrating recto-sigmoid tissue stenosing thickening with upstream colic distension, digestive perforation, and abscessed peritonitis.
View Figure 4-5
Per operative exploration noted advanced peritonitis, Douglas abscess and punctuate rectal perforation. She had a peritoneal lavage with placement of a percutaneous colostomy and a biopsy of an omental fringe. Histological examination was in favor of carcinomatous lymphangitis. Thereafter, the teenager presented a painful swelling of the left lower limb. Ultrasound exam concluded with multiple compressive inguinal nodes. The biopsy concluded with a lymph node metastasis of a digestive adenocarcinoma. Digital rectal examination noted budding ulcerative circumferential tumor 1 cm from the anal margin. She was proposed for rectal endoscopy and biopsy. Rectal endoscopy noted budding ulcerative circumferential and stenosing rectal tumor in continuity with pectineal line. The biopsy concluded with poorly differentiated Lieberkuhnian adenocarcinoma without any mucinous component. She presented during exploration bone pain; bone scan showed poly metastasis. Embryonic antigen carcinoma was elevated at 250 U/ml. The evolution was marked by onset of epileptic seizure. Cerebral scan revealed bilateral ischemic stroke. Anticoagulation and anti-epileptic treatment were prescribed. At admission in our department, clinical exam noted poor general condition, left lower limb flexed in vicious attitude, swelling of bilateral lower limb. The adolescent was cachectic. Abdomen was disdainful and tender. X-ray localized in left femur and hip didn’t note any fracture.
She had one cycle of FOLFIRI (Folinic acid, 5-fluorouracil, irinotecan) palliative chemotherapy. She was died 3 months after rectal cancer diagnosis.
She was a sixteen-year-old adolescent with family history of colonic adenocarcinoma in a paternal uncle at forty-year-old. She described right paroxysmal pelvic pain in the last 3 months without any other plaints. She consulted urgently for abdominal pain. Complicated appendicitis was suspected. During surgery, an infected sigmoid tumor was discovered. She had sigmoid and descending colon resection with placement of left colostomy. Histological examination revealed a poorly differentiated mucinous adenocarcinoma, infiltrating the pericolic fat. Two lymph nodes among the 22 removed were metastatic. Surgical limits were healthy. Chest X-ray, abdominal ultrasound and colonoscopy were without abnormalities. The tumor was classified as pT3N1M0. The patient had 12 cycles of adjuvant chemotherapy by FOLFOX (5fluorouracil, Folinic acid, Oxaliplatin). Currently, she was at 13 years failure free.
Family investigation based on colonoscopy detected a colonic adenocarcinoma in her father, so lynch syndrome was established.
CRC’s incidence is steadily rising in developing nations and it is typically a disease of older adults, with 90% of patients with CRC being above 55 years of age [6,7]. Because of introduction of population-based screening in many western countries, the incidence of CRC above age 50 is decreasing. At the same time, incidence rates under age 50 annually increase with particularly worrying rates in the youngest age group [8-10] explaining that many recent papers discuss CRC in adolescent and young adult peoples.
CRC rarely occurs before the age of 20 years [1,3,4,7,9]. The vast majority of children reported with CRC were over 10 years of age while the youngest reported patient is a 9-month- old female infant [4,11]. The reported peak age in pediatric population is 15 years old [4,12]. In our institution, for 16 years, since 2006 till 2022, only 2 patients were treated for CRC and were under 20 years old.
CRC usually presents with melena, abdominal pain, altered bowel habits, or with obstruction or perforation. If there is no difference in symptoms between adults and children [13], the differences in duration of symptoms, often exceeding 6 months among pediatric population are striking and have been noted in earlier reports [14]. This is because many of the clinical features are non-specific and similar to those found in common childhood problems such appendicitis, gastro-enteritis and simple constipation and the rarity of colon cancer in pediatric population [9,15]. CRC can also be found at surgery for intussusception, bowel obstruction, or perforation, as well as incidentally during a surgical or radiologic procedure for other reasons acute presentations, account for almost 50% of presentations in some pediatric reports [2,16]. Due to diagnostic delay, advanced stage at presentation is more likely in pediatric population compared to older adults with CRC [9,13].
One of our patients presented condition of complicated appendicitis. Per operative exploration discovered the CRC. The other one presented peritonitis and colonic perforation. The tumor was locally advanced with peritoneal carcinomatosis.
CRC usually metastasizes to regional lymph nodes, liver, lungs, and peritoneum; metastasis to bone is very rare and few cases have been reported in the literature [17,18]. This disease entity represents a very aggressive form of CRC. Our first patient presented bone metastasis and died after one cycle of chemotherapy.
CRC is usually more frequent in male in adult. Sex ratio is equal 1 in pediatric population [3]. In our institution for 16 years, we had only included two girls.
Several genetic syndromes are associated with CRC in the young. Well-defined CRC predisposition syndromes account for only about 3-5% of all cases of colon cancer; they include Peutz-Jeghers syndrome, familial juvenile polyposis, hereditary mixed polyposis syndrome, hereditary non-polyposis colon cancer or Lynch syndrome, and familial adenomatous polyposis. Mork, et al. noted an identifiable hereditary cancer syndrome in 35% of 193 adolescent and young adults with CRC supporting universal genetic testing for this population [19]. 22% of adolescent and young adult with CRC have a family history of the disease but most cases are sporadic [9].
One of our patients had family history of CRC fulfilling Amsterdam criteria and allowing the conclusion of a lynch syndrome. The other one had no personal or familial medical history and were sporadic case. A genetic testing should have been done but unfortunately it isn’t available in our institution.
CRC in adults is usually moderately differentiated or well differentiated adenocarcinomas. In contrast, more than half of reported cases of childhood CRC are poorly differentiated mucinous adenocarcinoma, and many are of the signet-ring cell type [1,20]. These tumors are more aggressive and are associated with extensive intramural spread and peritoneal carcinomatosis [4]. Higher incidence of unresectable and higher metastasis rate in childhood are reported [14,21]. Only 19 % of children and adolescents have localized disease [22].
CRC in children is carries a dismal prognosis and children. In many series, no child living longer than 1 year after diagnosis [21,23]. The 5-year survival rate for children ranges from 7% to 12% [24]. More recently, Sultan et al reported a 5-year relative survival in children- adolescents as 40% ± 4.2% [20]. Our patient who had localized tumor was 13 years failure free. In the absence of pediatric prospective clinical trials, treatment guidelines must be extrapolated from adult trials. Following adult principles of treatment, the mainstay of therapy is complete surgical resection [4]. The rate of complete resection has been less than optimal in children and it was possible in only in 40% of cases in [14]. Adjuvant multi-agent chemotherapy by Folfox is typically used in high-risk localized disease [4].
To conclude colorectal cancer in children though rare can be a reality, hence any children presenting with pain in abdomen along with doubtful history of constipation and rectal bleeding should be examined carefully with special emphasis on DRE.